
Abstract
Hepatocellular carcinoma (HCC) is a unique malignancy that can be diagnosed and treated based on non-invasive imaging criteria without histological confirmation in cirrhotic patients, which opens the possibility, although rare, of false-positive diagnosis of the tumor. This brief review illustrates benign and non-HCC malignant lesions arising in cirrhotic liver that could have been erroneously diagnosed as HCC based on imaging criteria: focal nodular hyperplasia–like nodules, serum amyloid A–positive nodules, dysplastic nodules, spontaneously regressing lesions, combined hepatocellular-cholangiocarcinoma, cholangiocarcinoma, sarcomatoid carcinoma, lymphoepithelioma-like carcinoma, hepatoblastoma, and metastatic adenocarcinoma. To determine the potential differences in clinical courses and post-treatment outcome of HCC diagnosed by imaging alone and those histologically, we suggest the terms HCCi and HCCp to distinguish between lesions that are diagnosed as HCC based on imaging alone from those diagnosed based on pathological examination, respectively.
Key Points
• Benign lesions, such as focal nodular hyperplasia–like nodules, serum amyloid A–positive nodules, dysplastic nodules, and spontaneously regressing lesions, may show imaging findings that mislead to the diagnosis of HCC.
• Non-hepatocellular malignant lesions, such as sarcomatoid carcinoma, lymphoepithelioma-like carcinoma, hepatoblastoma, and metastatic adenocarcinomas, can be erroneously diagnosed as HCC based on imaging findings alone, even in cirrhotic liver.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Hepatocellular carcinoma (HCC) is the only malignancy that can be diagnosed and treated based on non-invasive imaging criteria without histological confirmation before treatment in cirrhotic patients [1, 2]. The non-invasive imaging diagnosis of HCC requires demonstration of typical imaging features associating arterial phase hyperenhancement (APHE) and a “washout” appearance on later phases of dynamic imaging, as well as capsule appearance and threshold growth that add evidence to the diagnosis according to liver reporting and data system (LI-RADS) [3,4,5].
Although various benign or malignant lesions have been reported to mimic HCC in patients with cirrhosis or chronic liver disease, most of these lesions may be correctly differentiated from HCC if diagnostic imaging criteria are properly applied [6,7,8]. However, there are still several lesions that present imaging features typical of HCC and can be falsely diagnosed as such, if the diagnosis is made based on imaging criteria alone.
Various guidelines for imaging diagnosis proposed by expert bodies differ with regard to applicability and diagnostic criteria with potential differences in sensitivity or specificity [9]. For example, the guidelines of the European Association for the Study of the Liver limits the imaging diagnosis only to cirrhotic liver, of which a diagnosis method (histologically or clinically) is not specified [3]. In contrast, according to the American Association for Study of Liver Disease/Liver Reporting and Data System [10], imaging diagnosis can be applied to patients with cirrhosis or chronic hepatitis B, excluding cirrhosis related to certain vascular diseases [11].
In this review, we present benign and malignant hepatic lesions that have occurred in cirrhotic liver that could have been diagnosed as HCC based on non-invasive diagnostic criteria, but were confirmed otherwise. By doing so, we illustrate several limitations of non-invasive diagnosis of HCC by imaging examination alone, either computed tomography (CT) or magnetic resonance imaging (MRI). We suggest that these “HCC diagnosed by imaging criteria alone (HCCi)” may have the potential to show different clinical courses and post-treatment outcomes to those of “HCC diagnosed on pathologic examination (HCCp).”
Benign lesions
Focal nodular hyperplasia–like nodules
Focal nodular hyperplasia–like nodules (FNH-LNs) resemble focal nodular hyperplasia on histological examination, but arise in cirrhotic liver, especially in patients with alcoholic cirrhosis or vascular abnormalities [12, 13]. FNH-LN may mimic HCC by demonstrating either APHE or a “washout” and capsule appearance on CT or MRI, although the presence of both APHE and washout appearances is relatively rare [14, 15] (Fig. 1). In a study on 130 cirrhotic explanted livers, FNH-LNs were found in 15% [16]. Meanwhile, in a study including nine FNH-LNs arising in patients at risk for HCC, three (33.3%) could have been wrongly diagnosed as HCC based on imaging diagnosis criteria [14]. The presence of ancillary features of HCC, such as T2 heterogeneity, signs of diffusion restriction, and heterogeneous uptake of hepatocyte contrast material, may be useful to correctly distinguish HCC from FNH-LN [15]. In contrast, findings that are atypical for HCC, such as homogeneous hyperintensity on T1-weighted images, isointensity on T2-weighted images, and homogeneous hyperintensity with central scar on hepatocyte-specific contrast material–enhanced MRI, are indicative of diagnoses other than HCC and prompt histologic confirmation for the correct diagnosis of FNH-LN [15, 17].

Focal nodular hyperplasia–like nodule in a 34-year-old woman with alcoholic cirrhosis. Arterial (a) and equilibrium (b) phase images of multiphase dynamic CT examination obtained after administration of 2 mL/kg of 300 mgI/mL of low osmolar non-ionic contrast material show a nodular mass (arrows) with arterial hyperenhancement, washout appearance, and capsule appearance. Gadoxetate-enhanced arterial (c) and venous (d) phase images (0.025 mmol/kg) also show a globally hyperenhancing mass with washout and capsule appearance (arrows)
Serum amyloid A–positive nodules
Serum amyloid A (SAA)–positive nodules are benign nodules that have similar characteristics to those of FNH-LN arising in alcoholic cirrhosis, but also share histologic features with inflammatory hepatocellular adenoma based on SAA expression, sinusoidal dilation, and ductular and inflammatory reactions [18]. The differential diagnosis of SAA-positive nodules from HCC can be more difficult than that for FNH-LN, as they show hypointensity on hepatobiliary phase images of hepatobiliary contrast material–enhanced MRI as well as APHE and washout appearance [19]. However, SAA-positive nodules may be distinguished based on the presence of small (< 2 cm) and multiple lesions. The incidence of presenting both APHE and washout appearance in SAS-positive nodules is not well known, although it has been reported that two-thirds (8/12, 67%) of SAA-positive nodules show hypointensity in the hepatobiliary phase of gadoxetate-enhanced MRI [18]. At our institute, among 400 transplanted livers, we noted two SAA-positive nodules in one patient that were difficult to differentiate from HCC (Suppl. Fig. 1).
Dysplastic nodules
Both low- and high-grade dysplastic nodules may demonstrate focal areas of arterial blood supply on CT hepatic arteriography [20]. On dynamic imaging, it may not be uncommon for dysplastic nodules to show APHE or washout appearance [21,22,23]. Rarely, both APHE and washout appearance can be observed in dysplastic nodules, making differentiation from HCC difficult (Suppl. Fig. 2). In one study, among seven high-grade dysplastic nodules, six showed APHE and five showed “washout” appearance; the specificity of the non-invasive diagnosis was 81% when these nodules were counted as false positive [24]. Therefore, for small lesions (1–1.5 cm) in particular, even though a lesion in cirrhotic liver may show both APHE and washout appearance, the presence of any atypical findings should prompt an alternative diagnostic examination to reduce false diagnosis of HCC [25, 26]. The coexistence of hyperintensity on T2-weighted images or diffusion restriction may favor the diagnosis of HCC, but these findings may also be present in dysplastic nodules [26,27,28].
Spontaneously regressing lesions
It is well known that arterially enhancing lesions seen in cirrhotic liver without washout appearance commonly disappear on follow-up examination [29]. However, lesions that show both APHE and washout appearance may also undergo spontaneous regression [30, 31] (Suppl. Fig. 3). The exact incidence of spontaneously regressing hypervascular and washout lesions overall is unknown, although according to a study that included 52 subcentimeter hypervascular and hepatobiliary hypointense lesions, 10 (67%) of 15 lesions showing both APHE and washout appearance turn out to be benign [30]. In such cases, there are two possibilities. One possibility is that the disappearing lesions may actually be benign lesions that undergo regression. Another possibility is that they are actually HCC, but undergo spontaneous necrosis. There have been reports that histologically confirmed HCC showed spontaneous necrosis or regression [32,33,34,35]. However, HCC undergoing spontaneous necrosis can also show late recurrence. Therefore, lesions that show spontaneous necrosis should be closely followed, because tumor recurrence may occur from remnant tumors or elsewhere in the liver.
Non-HCC malignancies
Combined hepatocellular-cholangiocarcinoma
Combined hepatocellular-cholangiocarcinoma (cHCC-CCA) has been considered a rare hepatic malignancy, but is increasingly recognized in cirrhotic liver [36]. Based on our hospital records and in previous reports [37, 38], cHCC-CCA is the second most common primary liver carcinoma in cirrhotic liver, followed by intrahepatic cholangiocarcinoma excluding perihilar cholangiocarcinoma. Therefore, cHCC-CCA should be the first differential diagnosis of HCC in patients with cirrhosis. There have been reports that 93.5–93.9% of cHCC-CCA may demonstrate at least one ancillary feature indicating non-HCC malignancy, such as targetoid enhancement pattern including rim-like APHE, liver surface retraction, or biliary obstruction [39, 40]. However, another study indicated that cHCC-CCAs showed identical imaging features in 16 (23%)–18 (25%) of 70 cHCC-CCAs with those of HCC showing no obvious imaging features suggestive of non-HCC malignancy and that these may not be differentiable from HCC based on imaging features alone [41] (Fig. 2). Nonetheless, there is a great necessity for a correct diagnosis and identification of histologic characteristics of cHCC-CCA, according to which the methods of surgical treatment and chemotherapeutic regimen may require to be adapted [42, 43].

Combined hepatocellular and cholangiocarcinoma in a 50-year-old man with B-viral cirrhosis. Gadoxetate-enhanced arterial (a), portal (b), and hepatobiliary (c) phase images show a 5-cm mass with arterial phase hyperenhancement, washout, and capsule appearance. Diffusion-weighted (d, b = 800 s/mm2) and apparent diffusion coefficient map (e) images show a mass with moderate diffusion restriction. f Gross specimen shows a mass with mosaic pattern and capsulation
Mass-forming intrahepatic cholangiocarcinoma
Excluding perihilar cholangiocarcinoma, mass-forming intrahepatic cholangiocarcinoma (MF-iCCA) is less common than cHCC-CCA in cirrhotic liver, but should be another important differential diagnosis of HCC [44, 45]. MF-iCCA is typically characterized by an irregularly marginated mass with rim-like enhancement on arterial phase and progressive central enhancement on late dynamic phase [46]. However, in cirrhotic liver, atypical global APHE and washout appearance may be more commonly seen in MF-iCCA than those arising in non-cirrhotic liver [45,46,47]. In a study by Huang et al [45], 7% of small iCCAs (3 cm or smaller) arising in cirrhotic liver showed wash-in and washout enhancement patterns, mimicking HCC. Moreover, peritumoral biliary dilation, which may be useful to correctly differentiate MF-iCCA from HCC, may be less common than that arising in non-cirrhotic liver [48]. MF-iCCA manifesting as HCC-like hypervascular enhancement pattern exhibits less fibrosis and more ductular components and can be subclassified into small duct-type cholangiocarcinoma [49, 50] (Fig. 3). Studies have reported that MF-iCCA showing APHE tended to have better post-surgical outcomes than those showing classical rim-like or poor enhancement [49, 51,52,53].

Cholangiocarcinoma in a 60-year-old woman with B-viral cirrhosis. On both post-contrast CT (a, b) and MRI (c, d), a mass shows arterial phase hyperenhancement (a, c) and washout appearance (b, d), mimicking hepatocellular carcinoma. Poorly enhancing area noted on both CT and MR images corresponds to tumor necrosis. (e) Corresponding gross specimen shows an area of coagulative necrosis (arrow)
Sarcomatoid carcinoma
Sarcomatoid carcinomas in the liver are conventional carcinomas containing a spindle cell component, which do not have specific mesenchymal differentiation as that of a carcinosarcoma [54]. Sarcomatoid carcinoma can be divided into sarcomatoid HCC, sarcomatoid CCA, sarcomatoid cHCC-CCA, or unclassified sarcomatoid carcinoma [55, 56]. Sarcomatoid carcinomas usually present as large, irregular, and peripherally enhancing masses with areas of central necrosis [55, 57, 58]. Therefore, typical imaging patterns indicating HCC (non-rim APHE and washout appearance) are less commonly seen in sarcomatoid carcinomas [59] and are mostly suspected as non-HCC malignancy in preoperative imaging. However, some sarcomatoid HCCs, especially those that are small, may show diagnostic imaging features of HCC and cannot be differentiated from HCC (Fig. 4). In our unpublished data, approximately 12% of sarcomatoid carcinomas could be classified as definitely HCC (LR-5) when the LI-RADS was applied. As sarcomatoid HCC may be considered a histologic variant of HCC, imaging diagnosis of sarcomatoid HCC as HCC may not be entirely incorrect. However, it is desirable to identify sarcomatoid carcinomas given that they have worse outcomes after treatment [59].

Sarcomatoid hepatocellular carcinoma in a 45-year-old man with B-viral cirrhosis. Precontrast (a), post-contrast arterial (b), portal venous (c), and equilibrium (d) phase CT images show a small nodular lesion with subtle arterial phase hyperenhancement and washout appearance (arrows). The lesion was not considered diagnostic of hepatocellular carcinoma at this examination. On the gadoxetate-enhanced MRI obtained 2 months after CT, the lesion shows obvious arterial phase hyperenhancement (e) and washout and capsule appearance (f). The lesion is hypointense on hepatobiliary phase image (g). T2-weighted (h) and diffusion-weighted (i, b = 800 s/mm2) images show a diffusion-restricted lesion. j Surgical specimen shows a small nodular mass in a cirrhotic liver
Lymphoepithelioma-like carcinoma
Lymphoepithelioma-like carcinoma (LELC) is a rare tumor composed of pleomorphic epithelial cells with a prominent lymphoid infiltrate and may present as one of two forms: lymphoepithelioma-like hepatocellular carcinoma or lymphoepithelioma-like cholangiocarcinoma [60]. As both forms of LELC have different pathogeneses and a better clinical course than HCC and iCCA, they should be distinguished from HCC [61]. The imaging findings of LELC are not well known, but may mimic those of HCC by exhibiting APHE and washout appearance [62, 63] or those of iCCA by exhibiting rim-like APHE [64] (Suppl. Fig. 4). There is no report on a collective series of imaging features of LELC. However, according to a report by Lee et al [65] regarding the false-positive diagnosis of HCC in 837 liver resection patients, one LELC was recorded among the 18 (2.2%) false-positive diagnoses of HCC.
Hepatoblastoma
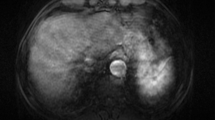
Hepatoblastoma is the most common primary malignant hepatic tumor in children, mostly occurring at the ages of 6 months and 3 years, but is extremely rare in adults [66, 67]. Differential diagnosis of hepatoblastoma arising in adults from HCC is difficult even on pathological examination because the two tumors share similar gross and microscopic characteristics [66]. Similar to pediatric forms, adult hepatoblastoma commonly shows capsulation or pseudocapsule formation and elevation of serum alpha-fetoprotein level [66]. Approximately 25% of adult hepatoblastomas have been reported in cirrhotic liver [68]. Imaging diagnosis of adult hepatoblastoma is also challenging because of its extremely low prevalence in adults and similar tumor characteristics to those of HCC. However, hepatoblastoma may be characterized by a more heterogeneous texture because of its mixed histologic components [69] (Fig. 5). According to the abovementioned series of Lee et al [65], two hepatoblastomas were included among the 18 (2.2%) false-positive diagnoses of HCC.

Hepatoblastoma in a 75-year-old man with B-viral cirrhosis. Dynamic CT precontrast (a), arterial (b), venous (c), and equilibrium (d) phase images show a heterogeneously hypervascular mass with washout and capsule appearance. Gadoxetate-enhanced MRI, precontrast (e), arterial (f), and venous (g) phase images show an encapsulated mass with arterial hyperenhancement and washout. Diffusion-weighted image (h, b = 800 s/mm2) and apparent diffusion coefficient map (i) image show a mass with diffusion restriction. j Corresponding surgical specimen
Metastatic adenocarcinoma
Metastatic carcinoma is relatively uncommon in cirrhotic liver, probably due to alteration of hemodynamics and microstructural environment in the liver [8]. When metastatic cancers are found in cirrhotic liver, they usually show rim-like APHE and can be categorized as non-HCC malignancy according to the imaging criteria of LI-RADS [37]. However, when a metastasis in cirrhotic liver demonstrates both non-rim APHE and washout appearance, it can be misdiagnosed as HCC (Fig. 6). As the current guidelines do not recommend restraining imaging diagnosis in patients with extrahepatic malignancy when they have cirrhosis, imaging diagnosis of HCC should be conducted with caution in patients with both extrahepatic malignancy and cirrhosis. According to our unpublished data, three (6.6%) out of 45 metastases arising in patients with cirrhosis or chronic hepatitis B could not be differentiated from HCC.

Metastatic adenocarcinoma from gastric cancer in a 65-year-old man with B-viral cirrhosis. Gadoxetate-enhanced MRI, precontrast (a), arterial phase (b), and venous phase (c) images show a nodular lesion in the caudate lobe of the liver, presenting with arterial phase hyperenhancement and washout appearance. T2-weighted fast spin-echo (d) and diffusion-weighted (e, b = 800 s/mm2) images show a hyperintense lesion. f Gross specimen shows the corresponding lesion
Conclusion
We have illustrated benign and malignant lesions found in histologically proven cirrhotic liver, showing imaging features compatible with HCC. Other lesions that were not addressed in this review but have been reported in cirrhotic liver by mimicking HCC include bile duct adenoma [70], inflammatory pseudotumor [71], angiomyolipoma [65], and chronic abscess [72]. The lesions we presented above may have been diagnosed clinically as HCC and would have been treated as such, if imaging criteria alone had been used for planning a locoregional treatment without histologic diagnosis. Although we only presented HCC-like tumors found in cirrhotic liver, there could have been more diverse entities showing the typical appearances of HCC, if we had included cases found in patients with chronic B-viral hepatitis or with other risk factors for HCC. Moreover, even though patients undergo locoregional treatment without histologic confirmation, they would be given a diagnosis of HCC and treated as such on further management.
Therefore, we suggest that lesions that were diagnosed as HCC on imaging alone should be referred to with a different term, such as HCCi, meaning “HCC diagnosed based on imaging but not pathologic examinations.” In contrast, HCCs that were diagnosed as HCCs based on pathology may be designated as HCCp when they need to be distinguished from HCCi. Distinction of HCCi and HCCp would be relevant because histologic evaluation is important not only for the correct diagnosis of HCC but also for the identification of distinct subtype for estimation of prognosis and planning targeted therapy [73]. By using different terms (HCCi or HCCp) for the different HCCs diagnosed histologically or by imaging, it will be possible to evaluate the potential differences in prognosis between HCCi and HCCp after a certain treatment, especially locoregional treatment in which histological diagnosis is not typically obtained.
In conclusion, some benign and non-HCC malignant lesions can be diagnosed as HCC by satisfying imaging criteria. We propose distinguishing HCCs diagnosed based on imaging from those diagnosed by histologic examination using terms such as HCCi and HCCp.
Abbreviations
- APHE:
-
Arterial phase hyperenhancement
- cHCC-CCA:
-
Combined hepatocellular-cholangiocarcinoma
- FNH-LNs:
-
Focal nodular hyperplasia–like nodules
- HCC:
-
Hepatocellular carcinoma
- HCCi:
-
HCC diagnosed by imaging criteria alone
- HCCp:
-
HCC diagnosed on pathologic examination
- LELC:
-
Lymphoepithelioma-like carcinoma
- LI-RADS:
-
Liver reporting and data system
- MF-iCCA:
-
Mass-forming intrahepatic cholangiocarcinoma
- SAA:
-
Serum amyloid A
References
Kudo M, Trevisani F, Abou-Alfa GK, Rimassa L (2016) Hepatocellular carcinoma: therapeutic guidelines and medical treatment. Liver Cancer 6:16–26
Heimbach JK, Kulik LM, Finn RS et al (2018) AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 67:358–380
European Association for the Study of the Liver (2018) EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 69:182–236
Park HJ, Choi BI, Lee ES, Park SB, Lee JB (2017) How to differentiate borderline hepatic nodules in hepatocarcinogenesis: emphasis on imaging diagnosis. Liver Cancer 6:189–203
Chernyak V, Fowler KJ, Kamaya A et al (2018) Liver Imaging Reporting and Data System (LI-RADS) version 2018: imaging of hepatocellular carcinoma in at-risk patients. Radiology 289:816–830
Ronot M, Dioguardi Burgio M, Purcell Y, Pommier R, Brancatelli G, Vilgrain V (2017) Focal lesions in cirrhosis: not always HCC. Eur J Radiol 93:157–168
Galia M, Taibbi A, Marin D et al (2014) Focal lesions in cirrhotic liver: what else beyond hepatocellular carcinoma? Diagn Interv Radiol 20:222–228
Elsayes KM, Chernyak V, Morshid AI et al (2018) Spectrum of pitfalls, pseudolesions, and potential misdiagnoses in cirrhosis. AJR Am J Roentgenol 211:87–96
Cruite I, Tang A, Sirlin CB (2013) Imaging-based diagnostic systems for hepatocellular carcinoma. AJR Am J Roentgenol 201:41–55
Tang A, Bashir MR, Corwin MT et al (2018) Evidence supporting LI-RADS major features for CT- and MR imaging-based diagnosis of hepatocellular carcinoma: a systematic review. Radiology 286:29–48
Tang A, Hallouch O, Chernyak V, Kamaya A, Sirlin CB (2018) Epidemiology of hepatocellular carcinoma: target population for surveillance and diagnosis. Abdom Radiol (NY) 43:13–25
Lee YH, Kim SH, Cho MY, Shim KY, Kim MS (2007) Focal nodular hyperplasia-like nodules in alcoholic liver cirrhosis: radiologic-pathologic correlation. AJR Am J Roentgenol 188:W459–W463
Marin D, Galluzzo A, Plessier A, Brancatelli G, Valla D, Vilgrain V (2011) Focal nodular hyperplasia-like lesions in patients with cavernous transformation of the portal vein: prevalence, MR findings and natural history. Eur Radiol 21:2074–2082
Choi JY, Lee HC, Yim JH et al (2011) Focal nodular hyperplasia or focal nodular hyperplasia-like lesions of the liver: a special emphasis on diagnosis. J Gastroenterol Hepatol 26:1004–1009
Kim JW, Lee CH, Kim SB et al (2017) Washout appearance in Gd-EOB-DTPA-enhanced MR imaging: a differentiating feature between hepatocellular carcinoma with paradoxical uptake on the hepatobiliary phase and focal nodular hyperplasia-like nodules. J Magn Reson Imaging 45:1599–1608
Libbrecht L, Cassiman D, Verslype C et al (2006) Clinicopathological features of focal nodular hyperplasia-like nodules in 130 cirrhotic explant livers. Am J Gastroenterol 101:2341–2346
Kim MJ, Rhee HJ, Jeong HT (2012) Hyperintense lesions on gadoxetate disodium-enhanced hepatobiliary phase imaging. AJR Am J Roentgenol 199:W575–W586
Sasaki M, Yoneda N, Sawai Y et al (2015) Clinicopathological characteristics of serum amyloid A-positive hepatocellular neoplasms/nodules arising in alcoholic cirrhosis. Histopathology 66:836–845
Kim SR, Kondo F, Otono Y et al (2014) Serum amyloid A and C-reactive protein positive nodule in alcoholic liver cirrhosis, hard to make definite diagnosis. Hepatol Res 44:584–590
Lim JH, Cho JM, Kim EY, Park CK (2000) Dysplastic nodules in liver cirrhosis: evaluation of hemodynamics with CT during arterial portography and CT hepatic arteriography. Radiology 214:869–874
Chou CT, Chou JM, Chang TA et al (2013) Differentiation between dysplastic nodule and early-stage hepatocellular carcinoma: the utility of conventional MR imaging. World J Gastroenterol 19:7433–7439
Lim JH, Kim MJ, Park CK, Kang SS, Lee WJ, Lim HK (2004) Dysplastic nodules in liver cirrhosis: detection with triple phase helical dynamic CT. Br J Radiol 77:911–916
Inchingolo R, De Gaetano AM, Curione D et al (2015) Role of diffusion-weighted imaging, apparent diffusion coefficient and correlation with hepatobiliary phase findings in the differentiation of hepatocellular carcinoma from dysplastic nodules in cirrhotic liver. Eur Radiol 25:1087–1096
Sersté T, Barrau V, Ozenne V et al (2012) Accuracy and disagreement of computed tomography and magnetic resonance imaging for the diagnosis of small hepatocellular carcinoma and dysplastic nodules: role of biopsy. Hepatology 55:800–806
Choi MH, Choi JI, Lee YJ, Park MY, Rha SE, Lall C (2016) MRI of small hepatocellular carcinoma: typical features are less frequent below a size cutoff of 1.5 cm. AJR Am J Roentgenol. https://doi.org/10.2214/AJR.16.16414:1-8
Rhee H, Kim MJ, Park MS, Kim KA (2012) Differentiation of early hepatocellular carcinoma from benign hepatocellular nodules on gadoxetic acid-enhanced MRI. Br J Radiol 85:e837–e844
Kim TK, Lee KH, Jang HJ et al (2011) Analysis of gadobenate dimeglumine-enhanced MR findings for characterizing small (1-2-cm) hepatic nodules in patients at high risk for hepatocellular carcinoma. Radiology 259:730–738
Renzulli M, Biselli M, Brocchi S et al (2018) New hallmark of hepatocellular carcinoma, early hepatocellular carcinoma and high-grade dysplastic nodules on Gd-EOB-DTPA MRI in patients with cirrhosis: a new diagnostic algorithm. Gut 67:1674–1682
Byrnes V, Shi H, Kiryu S, Rofsky NM, Afdhal NH (2007) The clinical outcome of small (<20 mm) arterially enhancing nodules on MRI in the cirrhotic liver. Am J Gastroenterol 102:1654–1659
Park CJ, An C, Park S, Choi JY, Kim MJ (2018) Management of subcentimetre arterially enhancing and hepatobiliary hypointense lesions on gadoxetic acid-enhanced MRI in patients at risk for HCC. Eur Radiol 28:1476–1484
Kim JE, Kim SH, Lee SJ, Rhim H (2011) Hypervascular hepatocellular carcinoma 1 cm or smaller in patients with chronic liver disease: characterization with gadoxetic acid-enhanced MRI that includes diffusion-weighted imaging. AJR Am J Roentgenol 196:W758–W765
Lee SC, Chung HW, Chung JB et al (2002) Total necrosis of hepatocellular carcinoma due to spontaneous occlusion of feeding artery. Yonsei Med J 43:123–127
Del Poggio P, Mattiello M, Gilardoni L, Jamoletti C, Colombo S, Zabbialini G (2009) The mysterious case of spontaneous disappearance of hepatocellular carcinoma. Dig Liver Dis 41:e21–e25
Matsuoka S, Tamura A, Moriyama M et al (2015) Pathological evidence of the cause of spontaneous regression in a case of resected hepatocellular carcinoma. Intern Med 54:25–30
Bhardwaj N, Li M, Price T, Maddern GJ (2014) Spontaneous regression of a biopsy confirmed hepatocellular carcinoma. BMJ Case Rep 2014
Brunt E, Aishima S, Clavien PA et al (2018) cHCC-CCA: consensus terminology for primary liver carcinomas with both hepatocytic and cholangiocytic differentiation. Hepatology 68:113–126
Fraum TJ, Tsai R, Rohe E et al (2018) Differentiation of hepatocellular carcinoma from other hepatic malignancies in patients at risk: diagnostic performance of the Liver Imaging Reporting and Data System version 2014. Radiology 286:158–172
Kim YY, An C, Kim S, Kim MJ (2018) Diagnostic accuracy of prospective application of the Liver Imaging Reporting and Data System (LI-RADS) in gadoxetate-enhanced MRI. Eur Radiol 28:2038–2046
Potretzke TA, Tan BR, Doyle MB, Brunt EM, Heiken JP, Fowler KJ (2016) Imaging features of biphenotypic primary liver carcinoma (hepatocholangiocarcinoma) and the potential to mimic hepatocellular carcinoma: LI-RADS analysis of CT and MRI features in 61 cases. AJR Am J Roentgenol 207:25–31
Lee HS, Kim MJ, An C (2018) How to utilize LR-M features of the LI-RADS to improve the diagnosis of combined hepatocellular-cholangiocarcinoma on gadoxetate-enhanced MRI? Eur Radiol. https://doi.org/10.1007/s00330-018-5893-1
Jeon SK, Joo I, Lee DH et al (2018) Combined hepatocellular cholangiocarcinoma: LI-RADS v2017 categorisation for differential diagnosis and prognostication on gadoxetic acid-enhanced MR imaging. Eur Radiol. https://doi.org/10.1007/s00330-018-5605-x
Rogers JE, Bolonesi RM, Rashid A et al (2017) Systemic therapy for unresectable, mixed hepatocellular-cholangiocarcinoma: treatment of a rare malignancy. J Gastrointest Oncol 8:347–351
Lunsford KE, Court C, Seok Lee Y et al (2018) Propensity-matched analysis of patients with mixed hepatocellular-cholangiocarcinoma and hepatocellular carcinoma undergoing liver transplantation. Liver Transpl 24:1384–1397
Choi SH, Lee SS, Kim SY et al (2017) Intrahepatic cholangiocarcinoma in patients with cirrhosis: differentiation from hepatocellular carcinoma by using gadoxetic acid-enhanced MR imaging and dynamic CT. Radiology 282:771–781
Huang B, Wu L, Lu XY et al (2016) Small intrahepatic cholangiocarcinoma and hepatocellular carcinoma in cirrhotic livers may share similar enhancement patterns at multiphase dynamic MR imaging. Radiology 281:150–157
Chung YE, Kim MJ, Park YN et al (2009) Varying appearances of cholangiocarcinoma: radiologic-pathologic correlation. Radiographics 29:683–700
Xu J, Igarashi S, Sasaki M et al (2012) Intrahepatic cholangiocarcinomas in cirrhosis are hypervascular in comparison with those in normal livers. Liver Int 32:1156–1164
Sheng RF, Zeng MS, Rao SX, Ji Y, Chen LL (2014) MRI of small intrahepatic mass-forming cholangiocarcinoma and atypical small hepatocellular carcinoma (≤3 cm) with cirrhosis and chronic viral hepatitis: a comparative study. Clin Imaging 38:265–272
Kim SA, Lee JM, Lee KB et al (2011) Intrahepatic mass-forming cholangiocarcinomas: enhancement patterns at multiphasic CT, with special emphasis on arterial enhancement pattern--correlation with clinicopathologic findings. Radiology 260:148–157
Jeong HT, Kim MJ, Chung YE, Choi JY, Park YN, Kim KW (2013) Gadoxetate disodium-enhanced MRI of mass-forming intrahepatic cholangiocarcinomas: imaging-histologic correlation. AJR Am J Roentgenol 201:W603–W611
Fujita N, Asayama Y, Nishie A et al (2017) Mass-forming intrahepatic cholangiocarcinoma: enhancement patterns in the arterial phase of dynamic hepatic CT - correlation with clinicopathological findings. Eur Radiol 27:498–506
Nanashima A, Abo T, Murakami G et al (2013) Intrahepatic cholangiocarcinoma: relationship between tumor imaging enhancement by measuring attenuation and clinicopathologic characteristics. Abdom Imaging 38:785–792
Aherne EA, Pak LM, Goldman DA et al (2018) Intrahepatic cholangiocarcinoma: can imaging phenotypes predict survival and tumor genetics? Abdom Radiol (NY). https://doi.org/10.1007/s00261-018-1505-4
Torbenson MS (2017) Morphologic subtypes of hepatocellular carcinoma. Gastroenterol Clin North Am 46:365–391
Gu KW, Kim YK, Min JH, Ha SY, Jeong WK (2017) Imaging features of hepatic sarcomatous carcinoma on computed tomography and gadoxetic acid-enhanced magnetic resonance imaging. Abdom Radiol (NY) 42:1424–1433
Pua U, Low SC, Tan YM, Lim KH (2009) Combined hepatocellular and cholangiocarcinoma with sarcomatoid transformation: radiologic-pathologic correlation of a case. Hepatol Int 3:587–592
Koo HR, Park MS, Kim MJ et al (2008) Radiological and clinical features of sarcomatoid hepatocellular carcinoma in 11 cases. J Comput Assist Tomogr 32:745–749
Honda H, Hayashi T, Yoshida K et al (1996) Hepatocellular carcinoma with sarcomatous change: characteristic findings of two-phased incremental CT. Abdom Imaging 21:37–40
Liao SH, Su TH, Jeng YM et al (2018) Clinical manifestations and outcomes of patients with sarcomatoid hepatocellular carcinoma. Hepatology. https://doi.org/10.1002/hep.30162
Labgaa I, Stueck A, Ward SC (2017) Lymphoepithelioma-like carcinoma in liver. Am J Pathol 187:1438–1444
Chan AW, Tong JH, Pan Y et al (2015) Lymphoepithelioma-like hepatocellular carcinoma: an uncommon variant of hepatocellular carcinoma with favorable outcome. Am J Surg Pathol 39:304–312
Cacciato Insilla A, Faviana P, Pollina LE et al (2015) Lymphoepithelioma-like hepatocellular carcinoma: case report and review of the literature. World J Gastroenterol 21:10468–10474
Kim YC, Park MS, Chung YE et al (2010) MRI findings of uncommon non-hepatocyte origin primary liver tumours with pathological correlation. Br J Radiol 83:1080–1086
Liao TC, Liu CA, Chiu NC, Yeh YC, Chiou YY (2015) Lymphoepithelioma-like cholangiocarcinoma: a mimic of hepatocellular carcinoma on imaging features. World J Gastroenterol 21:4089–4095
Lee H, Yoon JH, Kim H et al (2017) False positive diagnosis of hepatocellular carcinoma in liver resection patients. J Korean Med Sci 32:315–320
Rougemont AL, McLin VA, Toso C, Wildhaber BE (2012) Adult hepatoblastoma: learning from children. J Hepatol 56:1392–1403
Sharma D, Subbarao G, Saxena R (2017) Hepatoblastoma. Semin Diagn Pathol 34:192–200
Roth CG, Mitchell DG (2014) Hepatocellular carcinoma and other hepatic malignancies: MR imaging. Radiol Clin N Am 52:683–707
Tan Y, Xiao EH (2013) Rare hepatic malignant tumors: dynamic CT, MRI, and clinicopathologic features: with analysis of 54 cases and review of the literature. Abdom Imaging 38:511–526
An C, Park S, Choi YJ (2013) Diffusion-weighted MRI in intrahepatic bile duct adenoma arising from the cirrhotic liver. Korean J Radiol 14:769–775
Chen CB, Chou CT, Hsueh C, Lee KW, Chen YL (2013) Hepatic inflammatory pseudotumor mimicking hepatocellular carcinoma. J Chin Med Assoc 76:299–301
Kim JW, Shin SS, Heo SH, Lim HS, Hur YH, Kim JH (2013) Hepatic abscess mimicking hepatocellular carcinoma in a patient with alcoholic liver disease. Clin Mol Hepatol 19:431–434
Kleiner DE (2018) Hepatocellular carcinoma: liver biopsy in the balance. Hepatology 68:13–15
Funding
The authors state that this work has not received any funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Myeong-Jin Kim.
Conflict of interest
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Statistics and biometry
Not applicable
Informed consent
Written informed consent was not required.
Ethical approval
Institutional Review Board approval was not required for this review.
Methodology
• Illustrative Review
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 4160 kb)
Rights and permissions
About this article

Cite this article
Kim, MJ., Lee, S. & An, C. Problematic lesions in cirrhotic liver mimicking hepatocellular carcinoma. Eur Radiol 29, 5101–5110 (2019). https://doi.org/10.1007/s00330-019-06030-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-019-06030-0