
Abstract
Rheumatoid arthritis (RA) is an autoimmune disease characterized by chronic inflammation that, if left untreated, can cause joint destruction and physical impairments. The inflammatory process is systematic, and it is associated with increased morbidity and mortality. Over the last years, mortality presents a decreasing trend; still, there is a high burden of cardiovascular disease (CVD) in RA that seems to be related to coronary atherosclerosis. Chronic inflammation, physical inactivity, and drugs used to treat RA are some of the reasons. Thus, the management of CVD risk is essential and involves the patient's stratification using distinct parameters that include assessment of the blood lipid profile. However, 'dyslipidemia' in RA patients follows a different pattern under the impact of inflammatory processes, while therapies that target the underlying disease change the levels of specific lipid components. In this review, we explore the relationship between blood lipids and inflammation in the so-called ΄lipid paradox΄ in RA, and we present the existing knowledge over the influence of antirheumatic drugs on the lipid profile of RA patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory disease that can cause the destruction of the synovial joints [1, 2]. The inflammatory process is systemic and may lead to several extra-articular manifestations. Among those, cardiovascular disease (CVD) is the most critical [2, 3]. Studies so far indicate that patients with RA have a 1.5-fold higher risk for heart attack, twofold risk for heart failure, and even higher for peripheral vascular disease compared to the general population [4,5,6]. Not surprisingly, the increased CVD risk among RA patients has led to an adjustment of the existing RA treatment guidelines. In 2017, the European League Against Rheumatism (EULAR) updated the recommendations for the screening and management of RA patients with CVD risk suggesting a cardiovascular assessment at least once every 5 years and further management of identified CVD risk factors [7]. According to these recommendations, total cholesterol (TC) and high-density lipoprotein cholesterol (HDL-C) should be used as part of the CVD risk assessment, while the TC/HDL-C ratio seems to be a better CVD risk predictor than the individual lipid components [7, 8]. In addition, these parameters should be measured when disease activity is stable or in remission, as current data show that in RA patients with active disease TC, low-density lipoprotein cholesterol (LDL-C), and HDL-C levels tend to be reduced [9]. The so-called lipid paradox is in contradiction to the conventional view that an atherogenic lipid profile is made up of increased TC, LDL-C, triglycerides (TGs), and decreased HDL-C. Interestingly, conventional synthetic(cs)and biological(b) disease-modifying antirheumatic drugs (DMARDs) increase lipid levels in RA patients and cause antiatherogenic changes in lipid composition and function [10].
Lipids and lipoproteins
Dyslipidemia is a term used when the plasma levels of lipids are altered. With increased cholesterol and TGsin plasma, atherogenicity occurs. The increased lipid levels are potentially related to increased lipid synthesis and/or decreased removal (clearance) or absorption. On the contrary, decreased lipid levels may be the result of decreased lipid synthesis and/or increased removal from the circulation (clearance).
An overview of current knowledge about the lipid metabolism is essential for understating the above processes: In general, lipids (cholesterol and TGs) are insoluble in water, and their transport via the blood circulation relies on their association with proteins. These proteins are called lipoproteins and are complex particles consisting of a central core that contains cholesterol esters and TGs. They are surrounded by a shell consisting of free cholesterol, phospholipids, and apolipoproteins, which facilitate lipoprotein formation and function (Fig. 1). Lipoproteins are classified according to their size, lipid composition, and apolipoproteins. There are several classes: chylomicrons and chylomicron remnants, very low-density lipoprotein (VLDL), intermediate-density lipoprotein (IDL), low-density lipoprotein (LDL), high-density lipoprotein (HDL)and lipoprotein-a (Lp-a). Chylomicron remnants, VLDL, IDL, LDL, and Lp-a, are all proatherogenic, while HDL is antiatherogenic.

Schematic representation of lipoprotein structure
The transport of dietary lipids in the blood is regulated by endogenous and exogenous pathways that act independently and achieve the lipid movement from the small intestine to the liver and peripheral tissues. A reverse transport mechanism exists, called reverse cholesterol transport (RChT), which removes excess cholesterol from peripheral tissues to the liver.
The exogenous lipoprotein pathway starts with the incorporation of dietary lipids into chylomicrons in the intestine. Chylomicrons are further metabolized in muscles and adipose tissue by the enzyme lipoprotein lipase (LPL), leading to the formation of free fatty acids (FFAs) and chylomicron remnants. These are then taken up by the liver (Fig. 2). The endogenous lipoprotein pathway starts in the liver with the formation of VLDL. The TGs carried in VLDL are metabolized in the peripheral tissues (muscles and adipose tissue) by LPL releasing FFAs, and IDL is formed. Then IDL is converted to LDL, which is taken up via the LDL receptor (LDLR) in numerous tissues, especially by the liver, a primary site of LDL uptake (Fig. 2). RChT starts with the formation of nascent HDL by the liver and intestine (Figs. 2, 3). The enzyme ATP-binding cassette transporter A1 (ABCA1) mediates the transfer of cellular cholesterol and phospholipids from peripheral tissues to the nascent HDL (lipid-poor HDL), leading to the formation of mature HDL. The last process is mediated by lecithin cholesterol acyltransferase (LCAT) (Figs. 2, 3). Mature HDL can acquire additional cholesterol from cells via the enzyme ATP-binding cassette transporter G1 (ABCG1) and class-B-scavenger receptor B1 (SR-B1). Then HDL transports the cholesterol to the liver by interacting with the hepatic SR-B1, or by transferring the cholesterol to LDL, a process mediated by the cholesteryl ester transfer protein (CETP) [11,12,13,14,15]. Once delivered to the liver, it can leave the body via biliary excretion (Fig. 3).

Schematic representation of the endogenous and exogenous cholesterol pathways

Schematic representation of reverse cholesterol transport
LDL can be grouped based on its size: large low-density LDL particles are designated as pattern A, and small high-density LDL particles are designated as pattern B. Pattern B has been associated with CVD since smaller particles are more easily able to penetrate the endothelium of the target cells. Oxidized LDL (ox-LDL) is a general term for LDL particles with oxidative modified structural components. As a result, in combination with free radicals’ attack, both lipids and protein parts of LDL can be oxidized in the vascular wall. Atherogenicity of ox-LDL has been explained by a lack of recognition of ox-LDL structures by the LDLR, preventing the normal metabolism of LDL particles and subsequently leading to atherosclerotic development [11,12,13,14,15].
In normal situations, HDL is responsible for the inhibition of ox-LDL and the cholesterol efflux from foam cells of the vessel wall [16]. There is no single explanation of the antiatherogenic and anti-inflammatory properties of HDL; however, it has become clear that the functional status of HDL depends on its protein component. In situations where there is an increased lipid production or decreased lipid clearance, a residual fraction of LDL is oxidized. Ox-LDL is incorporated or phagocytosed by macrophages and form the foam cells, which are further deposited on the arterial wall leading to atherosclerotic plaques. Thus, cholesterol movement or efflux through the RChT pathway is critical for maintaining cellular cholesterol homeostasis, not only in the context of the atherosclerotic lesion prevention but also for the restriction of “toxic” levels of cholesterol in every cell (Fig. 3).
Apolipoproteins are synthesized in the liver or intestine and are involved in lipid metabolism, as proteins that bind to lipids to form lipoproteins. They also act as ligands for lipoprotein receptors and co-factors of enzymes involved in lipoprotein metabolism. Particularly, apolipoprotein A-I (apo A-I), which is synthesized by the liver, is the major structural component of HDL, accounting for approximately 70% of the HDL protein structure while apolipoprotein A-II (apo A-II) accounts for 20%. Apolipoprotein B-48 (apo B-48) is synthesized exclusively by the intestine and is the major structural protein of chylomicrons and chylomicron remnants. Finally, apolipoprotein B-100 (apo B) is produced mainly in the liver and is the major structural protein component for VLDL, IDL, and LDL [11,12,13,14,15].
CVD risk factors in RA
Traditional CVD risk factors, including smoking, hypertension, dyslipidemia, insulin resistance, obesity, and physical inactivity, play an essential role, but alone do not fully explain the higher CVD risk in RA [17,18,19,20]. Non-traditional factors such as uncontrolled systemic inflammation, autoantibodies, and genetic factors are also essential pieces of this complex puzzle [21] (Fig. 4). Indeed, the elevation of the C-reactive protein (CRP) level has been shown to predict CVD in the general population [22], and also in RA patients where a significant association is observed between CRP and erythrocyte sedimentation rate (ESR) with atherosclerosis and higher risk for myocardial infarction and stroke [23,24,25]. Seropositivity, with either positive rheumatoid factor (RF) or anti-citrullinated protein antibodies (ACPA), is associated with increased coronary heart disease (CHD) and mortality from CHD, even in patients without articular symptoms [26]. This probably relates to the genetic contribution of the HLA-DRB1 shared epitope that is restricted to autoantibody-positive RA patients and is also associated with a higher cardiovascular mortality rate [27].

Schematic representation of chronic inflammatory disease process in RA patients and the development of CVD. Data suggests a complex interplay between traditional CVD risk factors, such as dyslipidemia, insulin resistance, hypertension, limited physical activity, and obesity, and RA-related characteristics, including chronic high-grade inflammation and autoimmune activation
The lipid paradox in RA
'Dyslipidemia' plays a fundamental role in atherosclerosis, but in RA patients is paradoxical to the general population. To address this issue, we conducted a comprehensive search of the literature published up until January 2020 using the Medline and Embase electronic databases [keywords “rheumatoid arthritis (AND) lipid profile or lipoprotein metabolism”]. Our search was restricted to articles published in English, and the most relevant publications were included.[28, 29]. According to the existing literature, RA patients with active disease present low levels of TC, LDL-C, and HDL-C, which elevate with treatments that target the RA inflammatory pathways [9]. In this frequently so-called 'lipid paradox,' a qualitative U-shaped relationship is proposed between patients' lipid profile and CV risk, where patients with the lowest LDL-C levels have higher CV risk than those with moderate levels [30]. The HDL-C level reduction in RA patients results in a high atherogenic index of TC/HDLC ratio [30, 31]. This 'atherogenic' lipid profile is a feature of early RA and established disease [31, 32], while reports are showing a reduction in TC and LDL-C even 5 years before RA diagnosis, a pattern that needs further study [33]. An inverse correlation between lipid concentrations and inflammatory markers is observed in RA patients, mainly between LDL-C levels and CRP [34]. Still, HDL-C levels appear to remain relatively stable with changes in inflammation, although data over the impact of treatments on the HDL-C are conflicting [35,36,37]. Interestingly, changes in lipid levels are more closely associated with changes in CRP than the Disease Activity Score-28 for Rheumatoid Arthritis (DAS28), which includes clinical and laboratory data for the assessment of disease activity [38] (Fig. 5).

Schematic representation of LDL-C levels during the RA disease course in relation to inflammatory markers. In early untreated disease with high levels of acute-phase reactants, the levels of LDL-C are low, while after treatment, when the disease is in remission with low acute phase reactants, the levels of LDL-C increase
The exact underlying mechanism for the altered lipid profile in RA remains unknown. Studies indicate that this lipid paradox is driven by the inflammatory process and is associated mainly with the increased cholesterol catabolism. Proinflammatory cytokines such as tumor necrosis factor-alpha (TNF-a) and interleukin (IL)-6, up-regulate LDLR and SRB1 receptors on hepatocytes, resulting in an increased uptake of LDL by the liver and secretion of cholesterol into the bile [39, 40]. As a consequence, circulating LDL levels decrease. This process was demonstrated by studies that measured cholesterol metabolism by labeling lipids with stable isotopes, a method that is considered the gold standard for studying lipids and lipoprotein metabolism in humans [41]. Interestingly, Strang et al. showed a decrease of LDLR expression after treatment with anti-IL-6 inhibitor, tocilizumab [42]. To measure catabolic clearance, the fractional catabolic rate (FCR) was used in two studies: the first one, by Charles-Schoeman et al., demonstrated that the cholesterol ester FCR, at baseline, was higher in RA patients as compared to control groups suggesting higher catabolism of cholesterol esters leading to lower cholesterol levels in these patients. When tofacitinib, a JAK1 and JAK3 inhibitor, was used as a treatment option in these patients, the FCR for the cholesterol ester decreased, and cholesterol levels increased [43]. In a study by Robertson et al., the FCR of LDL at baseline was in hyper-catabolic range compared to that expected in the general population, suggestive of an active turnover. After treatment with tocilizumab, the FCR decreased, being approximately similar to that of the general population [44]. Another mechanism potentially leading to reduced circulating LDL levels is oxidation, with studies showing that RA patients have higher levels of ox-LDL and antibodies against it [45, 46].
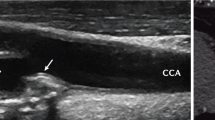
The level of inflammation correlates with the impact of LDL on CVD risk when ESR is more than 30 mm/h [47]. Also, high CRP in RA represents high inflammation, which correlates with the lipid paradox, and at the same time, it is associated with increased CVD risk [32, 48]. Indeed, studies have shown that markers of inflammation, such as the ESR and CRP, are associated with intima–media thickness [49, 50]. Interestingly, Ridker et al., while studying the effects of canakinumab, an interleukin-1 (IL-1) monoclonal antibody, in non-RA patients found that reduction of inflammation resulted in a decrease of CV events by 15% [51].
Moreover, the inflammation affects the antioxidant capacity of HDL. It has been demonstrated that the anti-inflammatory properties of HDL are impaired in animals [52, 53] and humans [54] during inflammation as it loses its ability to remove cholesterol from atherosclerotic plaques and becomes proatherogenic [29, 33]. This impaired HDL is proinflammatory and is characterized by a decrease of antioxidant factors [55] and gain of proinflammatory proteins [52]. It is also characterized by increased lipid hyperoxide content [54], leading to reduced potential efflux of cholesterol [56] and diminished ability to prevent ox-LDL [57]. As such, the levels of paraoxonase (PON), an antioxidant enzyme associated with HDL, are lower in RA than in controls [58], while in a study by Popa et al., changes in HDL antioxidant function were seen, expressed by an increased PON, after treatment with TNF-a inhibitor [59]. In addition, Watanabe et al. demonstrated that proinflammatory HDL in RA contains an altered proteome, including an increased amount of acute-phase proteins (such as fibrinogen, haptoglobin, and serum alpha-amyloid) and proteins of the complement system (C3, C4, and B-factor) [60]. Another study reported a reduction of the secretory phospholipase A2 and serum alpha-amyloid, during treatment with tocilizumab with modification of lipoprotein composition [61].
All the above indicate that the lipid paradox observed in RA and the high risk of CVD in these patients is mostly related to the qualitative aspects of lipids, especially the HDL, which loses its antiatherogenic function and finally becomes proatherogenic. Paradoxically, the treatment of RA patients reduces the inflammatory process but increases TC, LDL-C, and HDL-C, which is not associated with a rise in CV events [30].
The effect of antirheumatic drugs on lipid profile
The introduction of biological agents with the application of a treat to target therapy contributed to a better understanding of the underlying pathways related to CVD in RA. Studies provide considerable evidence on both csDMARDs and bDMARDs, but further work is needed to confirm and translate research findings into clinical practice.
DMARDs and corticosteroids
Corticosteroids are widely used in RA for symptomatic pain relief and reduction of the inflammatory process. They have many adverse effects, including an increase in CV risk factors such as carotid plaque formation and hypertension [62, 63]. Studies show that patients receiving high dose steroids (> 7.5 mg/day prednisone) have twice the risk of heart disease compared with those not taking steroids, while short-term, low-dose corticosteroids markedly affect plasma lipid levels mainly by elevating HDL-C levels [64].
The impact of csDMARDs on lipid profile has been studied extensively [29, 35, 65,66,67,68,69]. Hydroxychloroquine (HCQ), an antimalarial drug, is used to treat mild symptoms of RA and has been reported to increase HDL levels, either by reducing disease activity or by affecting lipid metabolism directly [65]. Methotrexate (MTX)is currently the first-line treatment for RA, and a recent meta-analysis showed that its use is related to 21% fewer CV events [66]. Evidence supports that MTX has an atheroprotective effect by promoting RChT and by limiting foam cell formation in THP-1 macrophages [67]. However, so far, in some human studies, MTX did not cause significant changes in lipid profile when administered alone or in combination with other cs or bDMARDs [68,69,70,71]. In contrast to the previous reports, other studies are indicating a significant increase in TC, LDL-C, and HDL-C cholesterol concentrations and cholesterol efflux capacity [35, 72, 73]. Nevertheless, the magnitude of the reported changes in the lipid fractions was smaller after 2 years of follow-up [74]. Interestingly, in patients with early RA, Georgiadis et al. [31, 32] showed, after 1 year of treatment with a steady dose of MTX in combination with prednisolone, elevations in TC, and HDL-C levels, although the TC/HDL-C ratio declined. A strong inverse relationship between CRP and HDL-C levels was observed, with no change in serum LDL-C levels.
Anti-tumor necrosis factor-alpha (anti-TNF-a) agents
Several short-term studies report a rapid increase in serum LDL-C or apoB levels after treatment with anti-TNF-a agents [75, 76]. In contrast, others indicate a neutral influence of infliximab treatment on lipid profile, since neither LDL-C levels nor TC/HDL-C and TGs/HDL-C ratios change significantly during therapy [77,78,79]. However, existing meta-analyses show a modest overall effect of TNF-a inhibitors on TC and HDL-C levels in RA patients with no significant effect on the atherogenic index [80,81,82]. Moreover, studies using a combination of anti-TNF-a agents, csDMARDs, and steroids show no significant interference with RA patients’ lipid profiles [83]. Thus, the overall favorable effect of infliximab treatment on cardiovascular comorbidity may relate to other factors such as arterial stiffness and insulin resistance improvement, but further investigation is needed to confirm this hypothesis [84, 85].
Anti-interleukin-6 (IL-6) agents
Tocilizumab, a humanized anti-IL-6-receptor monoclonal antibody that inhibits IL-6 signaling, presents a great therapeutic efficacy in RA patients. Current knowledge indicates that IL-6 affects lipid metabolism by stimulating lipid uptake via VLDLR induction, increasing hepatic and adipose tissue lipolysis, and decreasing hepatic lipid synthesis [86]. Several trials report that anti-IL6 therapy elevates serum TC, HDL-C, and TGs levels [87, 88]. Notably, the effect on the atherogenic index is inconsistent, but multiple studies show an increase in LDL-C levels by around 15–20% [88].
Janus kinase inhibitors (JAK inhibitors)
JAK inhibitors function by blocking the signaling JAK–STAT pathway, which results in the downregulation of immune response and RA remission. In phase III trials of tofacitinib, a dual JAK1–JAK3 inhibitor, LDL-C and HDL-C serum levels increased to approximately 21% and 14%, respectively, within 12 months of treatment [89]. Of note, these increases, in a head-to-head comparison between adalimumab and JAK inhibitors, were much higher than those seen after treatment with anti-TNF-a agents [90, 91]. A suggested mechanism for the increased cholesterol levels includes the reduction of cholesterol ester FCR that followsJAK inhibitor treatment in RA patients [43].
Other agents
Rituximab (RTX), a chimerical monoclonal antibody to CD20 of B-lymphocytes, has been successfully used in the treatment of highly active RA. Some studies demonstrate that RTX improves lipid profile as well as the atherogenicity index [92, 93]. On the contrary, a study by Mathieu et al. [94], which included 33 patients with RA mostly non-responders to previous anti-TNF therapies, showed no improvement of arterial stiffness and even an increase of LDL-C and the atherogenicity index. Further prospective studies are needed to clarify the effects of RTX on cardiovascular risk factors in RA.
Statins are effective in improving the lipid profile and prevent CVD [95]. Similar to the general population, statins reduce CVD risk in RA patients as well [96, 97]. Regarding the lipid paradox in RA and the changes in lipid profile observed after RA treatment, statins should be used in accordance with CVD treatment guidelines for primary prevention in this population. So far, this approach is not regularly used in clinical practice [98].
Conclusions
In RA patients, the observed 'atherogenic' phenotype, which consists of reduced TC, HDL-C, and LDL-C levels, is linked to the increased CV risk. Emerging evidence indicates that chronic inflammation has a significant impact on patients’ ‘dyslipidemia’ in both early and advanced disease. Moreover, suppressing inflammation through an antirheumatic treatment has a different influence on the degree and pattern of lipid profile change. Further understanding of the mechanisms underlying this paradox could maximize the effectiveness of used treatments and improve CV outcomes in such patients.
Abbreviations
- ACPA:
-
Anti-cyclic citrullinated protein antibodies
- apo A-I:
-
Apolipoprotein A-I
- ABCA1:
-
ATP-binding cassette transporter A1
- ABCG1:
-
ATP-binding cassette transporter G1 (ABCG1)
- apo A-II:
-
Apolipoprotein A-II
- apo B-48:
-
Apolipoprotein B-48
- apo B:
-
Apolipoprotein B-100
- b:
-
Biological
- CETP:
-
Cholesteryl ester transfer protein
- CHD:
-
Coronary heart disease
- CHOL:
-
Cholesterol
- CRP:
-
C-reactive protein
- CVD:
-
Cardiovascular disease
- Cs:
-
Conventional synthetic
- DAS-28:
-
Disease Activity Score-28 for Rheumatoid Arthritis
- DMARDs:
-
Disease-modifying antirheumatic drugs
- ESR:
-
Erythrocyte sedimentation rate
- EULAR:
-
European League Against Rheumatism
- HDL:
-
High-density lipoproteins
- HDL-C:
-
High-density lipoprotein cholesterol
- HCQ:
-
Hydroxychloroquine
- IDL:
-
Intermediate-density lipoproteins
- IL-6:
-
Interleukin-6
- JAK inhibitors:
-
Janus kinase inhibitors
- LDL:
-
Low-density lipoproteins
- LDL-C:
-
Low-density lipoprotein cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- LDLR:
-
LDL receptor
- LCAT:
-
Lecithin cholesterol acyltransferase
- Lp(a):
-
Lipoprotein(a)
- LPL:
-
Lipoprotein lipase
- FCR:
-
Fractional catabolic rate
- FFA:
-
Free fatty acids
- MTX:
-
Methotrexate
- Ox-LDL:
-
Oxidized LDL
- PON:
-
Paraoxonase
- RA:
-
Rheumatoid arthritis
- RF:
-
Rheumatoid factor
- RChT:
-
Reverse cholesterol transport
- RTX:
-
Rituximab
- SR-B1:
-
Class-B-scavenger receptor B1
- TC:
-
Total cholesterol
- TGs:
-
Triglycerides
- TNF-a:
-
Tumor necrosis factor-alpha
- VLDL:
-
Very low-density lipoproteins
References
Alamanos Y, Voulgari PV, Drosos AA (2006) Incidence and prevalence of rheumatoid arthritis, based on the 1987 American College of Rheumatology criteria: a systematic review. Semin Arthritis Rheum 36:182–188. https://doi.org/10.1016/j.semarthrit.2006.08.006
Alamanos Y, Drosos AA (2005) Epidemiology of adult rheumatoid arthritis. Autoimmun Rev 4:130–136. https://doi.org/10.1016/j.autrev.2004.09.002
Crowson CS, Liao KP, Davis JM, Solomon DH, Matteson EL, Knutson KL et al (2013) Rheumatoid arthritis and cardiovascular disease. Am Heart J166:622–628. https://doi.org/10.1016/j.ahj.2013.07.010
Avina-Zubieta JA, Thomas J, Sadatsafavi M, Lehman AJ, Lacaille D (2012) Risk of incident cardiovascular events in patients with rheumatoid arthritis: a meta-analysis of observational studies. Ann Rheum Dis 71:1524–1529. https://doi.org/10.1136/annrheumdis-2011-200726
Chuang YW, Yu MC, Lin CL, Yu TM, Shu KH, Huang ST, Kao CH (2016) Risk of peripheral arterial occlusive disease in patients with rheumatoid arthritis. A nationwide population-based cohort study. Thromb Haemost 115:439–445. https://doi.org/10.1160/TH15-07-0600
Stamatelopoulos KS, Kitas GD, Papamichael CM, Kyrkou K, Zampeli E, Fragiadaki K et al (2010) Subclinical peripheral arterial disease in rheumatoid arthritis. Atherosclerosis 212:305–309. https://doi.org/10.1016/j.atherosclerosis.2010.05.007
Agca R, Heslinga SC, Rollefstad S, Heslinga M, McInnes IB, Peters MJ et al (2017) EULAR recommendations for cardiovascular disease risk management in patients with rheumatoid arthritis and other forms of inflammatory joint disorders: 2015/2016 update. Ann Rheum Dis 76:17–28. https://doi.org/10.1136/annrheumdis-2016-209775
Peters MJ, Voskuyl AE, Sattar N, Dijkmans BA, Smulders YM, Nurmohamed MT (2010) The interplay between inflammation, lipids and cardiovascular risk in rheumatoid arthritis: why ratios may be better. Int J Clin Pract 64:1440–1443. https://doi.org/10.1111/j.1742-1241.2009.02220.x
Myasoedova E, Crowson CS, Kremers HM, Roger VL, Fitz-Gibbon PD, Therneau TM et al (2011) Lipid paradox in rheumatoid arthritis: the impact of serum lipid measures and systemic inflammation on the risk of cardiovascular disease. Ann Rheum Dis 70:482–487. https://doi.org/10.1136/ard.2010.135871
Myasoedova E (2017) Lipids and lipid changes with synthetic and biologic disease-modifying antirheumatic drug therapy in rheumatoid arthritis: implications for cardiovascular risk. Curr Opin Rheumatol 29:277–284. https://doi.org/10.1097/BOR.0000000000000378
Feingold KR, Grunfeld C (2018) Introduction to lipids and lipoproteins. Source endotext. MDText.com Inc., South Dartmouth
Rodrigo VB, Alfonso VB (2013) Overview about lipid structure lipid metabolism, Rodrigo Valenzuela Baez. IntechOpenRijeka
Mahley RW, Innerarity TL, Rall SC, Weisgraber KH (1984) Plasma lipoproteins: apolipoprotein structure and function. J Lipid Res 25:1277–1294
Canbay A, Bechmann L, Gerken G (2007) Lipid metabolism in the liver. Z Gastroenterol 45:35–41. https://doi.org/10.1055/s-2006-927368
Nguyen P, Leray V, Diez M, Serisier S, Bloc'hJ Le, Siliart B et al (2008) Liver lipid metabolism. J Anim Physiol Anim Nutr (Berl) 92:272–283. https://doi.org/10.1111/j.1439-0396.2007.00752.x
Navab M, Hama SY, Anantharamaiah GM, Hassan K, Hough GP, Watson AD et al (2000) Normal high density lipoprotein inhibits three steps in the formation of mildly oxidized low density lipoprotein: steps 2 and 3. J Lipid Res 41:1495–1508
Wu MF, Xu KZ, Guo YG, Yu J, Wu Y, Lin LM (2019) Lipoprotein(a) and atherosclerotic cardiovascular disease: current understanding and future perspectives. Cardiovasc Drugs Ther 33:739–748. https://doi.org/10.1007/s10557-019-06906-9
Jagpal A, Navarro-Millán I (2018) Cardiovascular co-morbidity in patients with rheumatoid arthritis: a narrative review of risk factors, cardiovascular risk assessment and treatment. BMC Rheumatol 2:10. https://doi.org/10.1186/s41927-018-0014-y
Stavropoulos-Kalinoglou A, Metsios GS, Panoulas VF, Douglas KMJ, Nevill AM, Jamurtas AZ et al (2009) Associations of obesity with modifiable risk factors for the development of cardiovascular disease in patients with rheumatoid arthritis. Ann Rheum Dis 68:242–245. https://doi.org/10.1136/ard.2008.095596
Panoulas VF, Metsios GS, Pace AV, John H, Treharne GJ, Banks MJ et al (2008) Hypertension in rheumatoid arthritis. Rheumatology 47:1286–1298. https://doi.org/10.1093/rheumatology/ken159
Toms TE, Symmons DP, Kitas GD (2010) Dyslipidaemia in rheumatoid arthritis: the role of inflammation, drugs, lifestyle and genetic factors. Curr Vasc Pharmacol 8:301–326. https://doi.org/10.2174/157016110791112269
Osman R, L'Allier PL, Elgharib N, Tardif JC (2006) Critical appraisal of C-reactive protein throughout the spectrum of cardiovascular disease. Vasc Health Risk Manag 2:221–237.
Goodson NJ, Symmons DP, Scott DG, Bunn D, Lunt M, Silman AJ (2005) Baseline levels of C-reactive protein and prediction of death from cardiovascular disease in patients with inflammatory polyarthritis: a ten-year follow-up study of a primary care-based inception cohort. Arthritis Rheum 52:2293–2299. https://doi.org/10.1002/art.21204
Gonzalez-Gay MA, Gonzalez-Juanatey C, Pineiro A, Garcia-Porrua C, Testa A, Llorca J (2005) High-grade C-reactive protein elevation correlates with accelerated atherogenesis in patients with rheumatoid arthritis. J Rheumatol 32:1219–1223
Zhang J, Chen L, Delzell E, Muntner P, Hillegass WB, Safford MM et al (2014) The association between inflammatory markers, serum lipids and the risk of cardiovascular events in patients with rheumatoid arthritis. Ann Rheum Dis 73:1301–1308. https://doi.org/10.1136/annrheumdis-2013-204715
Goodson NJ, Wiles NJ, Lunt M, Barrett EM, Silman AJ, Symmons DP (2002) Mortality in early inflammatory polyarthritis: cardiovascular mortality is increased in seropositive patients. Arthritis Rheum 46:2010–2019. https://doi.org/10.1002/art.10419
Farragher TM, Goodson NJ, Naseem H, Silman AJ, Thomson W, Symmons D et al (2008) Association of the HLA-DRB1 gene with premature death, particularly from cardiovascular disease, in patients with rheumatoid arthritis and inflammatory polyarthritis. Arthritis Rheum 58:359–369. https://doi.org/10.1002/art.23149
Gasparyan AY, Ayvazyan L, Blackmore H, Kitas GD (2011) Writing a narrative biomedical review: considerations for authors, peer reviewers, and editors. Rheumatol Int 31:1409–1417. https://doi.org/10.1007/s00296-011-1999-3
Baker JD (2016) The purpose, process, and methods of writing a literature review. AORN J 103:265–269. https://doi.org/10.1016/j.aorn.2016.01.016
Robertson J, Peters MJ, McInnes IB, Sattar N (2013) Changes in lipid levels with inflammation and therapy in RA: a maturing paradigm. Nat Rev Rheumatol 9:513–523. https://doi.org/10.1038/nrrheum.2013.91
Georgiadis AN, Papavasiliou EC, Lourida ES, Alamanos Y, Kostara C, Tselepis AD et al (2006) Atherogenic lipid profile is a feature characteristic of patients with early rheumatoid arthritis: effect of early treatment: a prospective, controlled study. Arthritis Res Ther 8:R82. https://doi.org/10.1186/ar1952
Georgiadis AN, Voulgari PV, Argyropoulou MI, Alamanos Y, Elisaf M, Tselepis AD et al (2008) Early treatment reduces the cardiovascular risk factors in newly diagnosed rheumatoid arthritis patients. Semin Arthritis Rheum 38:13–19. https://doi.org/10.1016/j.semarthrit.2007.09.008
Myasoedova E, Crowson CS, Kremers HM, Fitz-Gibbon PD, Therneau TM et al (2010) Total cholesterol and LDL levels decrease before rheumatoid arthritis. Ann Rheum Dis 69:1310–1314. https://doi.org/10.1136/ard.2009.122374
Ridker PM, Danielson E, Fonseca FA, Genest J, Gotto AM Jr, Kastelein JJ et al (2009) Reduction in C-reactive protein and LDL cholesterol and cardiovascular event rates after initiation of rosuvastatin: a prospective study of the JUPITER trial. Lancet 373:1175–1182. https://doi.org/10.1016/S0140-6736(09)60447-5
Van Lenten BJ, Reddy ST, Navab M, Fogelman AM (2006) Understanding changes in high density lipoproteins during the acute phase response. Arterioscler Thromb Vasc Biol 26:1687–1688. https://doi.org/10.1161/01.ATV.0000232522.47018.a6
Jamnitski A, Levels JH, van den Oever IA, Nurmohamed MT (2013) High-density lipoprotein profiling changes in patients with rheumatoid arthritis treated with tumor necrosis factor inhibitors: a cohort study. J Rheumatol 40:825–830. https://doi.org/10.3899/jrheum.121358
Navarro-Millán I, Charles-Schoeman C, Yang S, Bathon JM, Bridges SL Jr, Chen L (2013) Changes in lipoproteins associated with methotrexate or combination therapy in early rheumatoid arthritis: results from the treatment of early rheumatoid arthritis trial. Arthritis Rheum 65:1430–1438. https://doi.org/10.1002/art.37916
Liao KP, Playford MP, Frits M, Coblyn JS, Lannaccone C, Weinblatt ME et al (2015) The association between reduction in inflammation and changes in lipoprotein levels and HDL cholesterol efflux capacity in rheumatoid arthritis. J Am Heart Assoc 30:4. https://doi.org/10.1161/JAHA.114.001588
Hashizume M, Mihara M (2012) Atherogenic effects of TNF-α and IL-6 via up-regulation of scavenger receptors. Cytokine 58:424–430. https://doi.org/10.1016/j.cyto.2012.02.010
Lubrano V, Gabriele M, Puntoni MR, Longo V, Pucci L (2015) Relationship among IL-6, LDL cholesterol and lipid peroxidation. Cell Mol Biol Lett 20:310–322. https://doi.org/10.1515/cmble-2015-0020
Umpreby AM (2015) Hormone measurement guidelines: tracing lipid metabolism: the value of stable isotopes. J Endocrinol 226:G1–10. https://doi.org/10.1530/JOE-14-0610
Strang AC, BisoendialRJ KRS, Schulte DM et al (2013) Pro-atherogenic lipid changes and decreased hepatic LDL receptor expression by tocilizumab in rheumatoid arthritis. Atherosclerosis 229:174–181. https://doi.org/10.1016/j.atherosclerosis.2013.04.031
Charles-Schoeman C, Fleischmann R, Davignon J, Schwartz H, Turner SM, Beysen C et al (2015) Potential mechanisms leading to the abnormal lipid profile in patients with rheumatoid arthritis versus healthy volunteers and reversal by tofacitinib. Arthritis Rheumatol 67:616–625. https://doi.org/10.1002/art.38974
Robertson J, Porter D, Sattar N, Packard CJ, Caslake M, McInnes I et al (2017) Interleukin-6 blockade raises LDL via reduced catabolism rather than via increased synthesis: a cytokine-specific mechanism for cholesterol changes in rheumatoid arthritis. Ann Rheum Dis 76:1949–1952. https://doi.org/10.1136/annrheumdis-2017-211708
Chistiakov DA, Bobryshev YV, Orekhov AN (2016) Macrophage-mediated cholesterol handling in atherosclerosis. J Cell Mol Med 20:17–28. https://doi.org/10.1111/jcmm.12689
Lourida ES, Georgiadis AN, Papavasiliou EC, Papathanasiou AI, Drosos AA, Tselepis AD (2007) Patients with early rheumatoid arthritis exhibit elevated autoantibody titers against mildly oxidized low-density lipoprotein and exhibit decreased activity of the lipoprotein-associated phospholipase A2. Arthritis Res Ther 9:R19. https://doi.org/10.1186/ar2129
Maradit-Kremers H, Nicola PJ, Crowson CS, Ballman KV, Gabriel SE (2005) Cardiovascular death in rheumatoid arthritis: a population-based study. Arthritis Rheum 52:722–732. https://doi.org/10.1002/art.20878
Toms TE, Panoulas VF, Douglas KM, Nightingale P, Smith JP, Griffiths H et al (2011) Are lipid ratios less susceptible to change with systemic inflammation than individual lipid components in patients with rheumatoid arthritis? Angiology 62:167–175. https://doi.org/10.1177/0003319710373749
Del Rincon I, Polak JF, O’Leary DH, Battafarano DF, Erikson JM, Restrepo JF et al (2015) Systemic inflammation and cardiovascular risk factors predict rapid progression of atherosclerosis in rheumatoid arthritis. Ann Rheum Dis 74:1118–1123. https://doi.org/10.1136/annrheumdis-2013-205058
Ambrosino P, Lupoli R, Di Minno A, Tasso M, Peluso R, Di Minno MN (2015) Subclinical atherosclerosis in patients with rheumatoid arthritis. A meta-analysis of literature studies. Thromb Haemost 113:916–930. https://doi.org/10.1160/TH14-11-0921
Ridker PM, Everett BM, Thuren T, MacFadyen JG, Chang WH, Ballantyne C et al (2017) Antiinflammatory therapy with canakinumab for atherosclerotic disease. N Engl J Med 377:1119–1131. https://doi.org/10.1056/NEJMoa1707914
Van Lenten BJ, Hama SY, de Beer FC, Stafforini DM, McIntyre TM, Prescott SM et al (1995) Anti-inflammatory HDL becomes pro-inflammatory during the acute phase response. Loss of protective effect of HDL against LDL oxidation in aortic wall cell cocultures. J Clin Invest 96:2758–2767. https://doi.org/10.1172/JCI118345
Van Lenten BJ, Wagner AC, Nayak DP, Hama S, Navab M, Fogelman A (2001) High-density lipoprotein loses its anti-inflammatory properties during acute influenza a infection. Circulation 103:2283–2288. https://doi.org/10.1161/01.cir.103.18.2283
Ansell BJ, Navab M, Hama S, Kamranpour N, Fonarow G, Hough G, Rahmani S et al (2003) Inflammatory/antiinflammatory properties of high-density lipoprotein distinguish patients form control subjects better than high-density lipoprotein cholesterol levels and are favorably affected by simvastatin treatment. Circulation 108:2751–2756. https://doi.org/10.1161/01.CIR.0000103624.14436.4B
Mackness MI, Durrington PN, Mackness B (2004) The role of paraoxonase 1 activity in cardiovascular disease: potential for therapeutic intervention. Am J Cardiovasc Drugs 4:211–217. https://doi.org/10.2165/00129784-200404040-00002
Hayek T, Oiknine J, Brook JG, Aviram M (1994) Role of HDL apolipoprotein E in cellular cholesterol efflux: studies in apo E knockout transgenic mice. Biochem Biophys Res Commun 205:1072–1078. https://doi.org/10.1006/bbrc.1994.2775
Navab M, Ananthramaiah GM, Reddy ST, Van Lenten BJ, Ansell BJ, Hama S et al (2005) The double jeopardy of HDL. Ann Med 37(3):173–178. https://doi.org/10.1080/07853890510007322
Charles-Schoeman C, Lee YY, Grijalva V, Amjadi S, FitzGerald J, Ranganath VK et al (2012) Cholesterol efflux by high density lipoproteins is impaired in patients with active rheumatoid arthritis. Ann Rheum Dis 71:1157–1162. https://doi.org/10.1136/annrheumdis-2011-200493
Popa C, van Tits LJ, Barrera P, Lemmers HL, van den Hoogen FH, van Riel PL et al (2009) Anti-inflammatory therapy with tumour necrosis factor alpha inhibitors improves high-density lipoprotein cholesterol antioxidative capacity in rheumatoid arthritis patients. Ann Rheum Dis 68:868–872. https://doi.org/10.1136/ard.2008.092171
Watanabe J, Charles-Schoeman C, Miao Y, Elashoff D, Lee YY, Katselis G, Lee TD, Reddy ST (2012) Proteomic profiling following immunoaffinity captre of high-density lipoprotein: association of acute-phase proteins and complement factors with proinflammatory high-density lipoprotein in rheumatoid arthritis. Arthritis Rheum 64:1828–1837. https://doi.org/10.1002/art.34363
McInnes IB, Thompson L, Giles JT, Bathon JM, Salmon JE, Beaulieu AD et al (2015) Effect of interleukin-6 receptor blockade on surrogates of vascular risk in rheumatoid arthritis: measure, a randomised, placebo-controlled study. Ann Rheum Dis 74:694–702. https://doi.org/10.1136/annrheumdis-2013-204345
Davis JM, Kremers ΜH, Crowson CS, Nicola PJ, Ballman KV, Therneau TM et al (2007) Glucocorticoids and cardiovascular events in rheumatoid arthritis: a population-based cohort study. Arthritis Rheum 56:820–830. https://doi.org/10.1002/art.22418
Zampeli E, Protogerou A, Stamatelopoulos K, Fragiadaki K, Katsiari CG, Kyrkou K, Papamichael CM et al (2012) Predictors of new atherosclerotic carotid plaque development in patients with rheumatoid arthritis: a longitudinal study. Arthritis Res Ther 14:R44. https://doi.org/10.1186/ar3757
Hafstrom I, Rohani M, Deneberg S, Wornert M, Jogestrand T, Frostegard J (2007) Effects of low-dose prednisolone on endothelial function, atherosclerosis, and traditional risk factors for atherosclerosis in patients with rheumatoid arthritis–a randomized study. J Rheumatol 34:1810–1816
Morris SJ, Wasko MCM, Antohe JL, Sartorius JA, Kirchner HL, Dancea S et al (2011) Hydroxychloroquine use associated with improvement in lipid profiles in rheumatoid arthritis patients. Arthritis Care Res 63:530–534. https://doi.org/10.1002/acr.20393
Micha R, Imamura F, Ballmoos MW, Solomon DH, Hernán MA, RidkerPM, et al (2011) Systematic review and meta-analysis of methotrexate use and risk of cardiovascular disease. Am J Cardiol 108:1362–1370. https://doi.org/10.1016/j.amjcard.2011.06.054
Reiss AB, Carsons SE, Anwar K, Rao S, Edelman SD, Zhang H et al (2008) Atheroprotective effects of methotrexate on reverse cholesterol transport proteins and foam cell transformation in human THP-1 monocyte/macrophages. Arthritis Rheum 58:3675–3683. https://doi.org/10.1002/art.24040
RhoYH OeserA, Chung CP, Milne GL, Stein CM (2009) Drugs used in the treatment of rheumatoid arthritis: relationship between current use and cardiovascular risk factors. Arch Drug Inf 2:34–40. https://doi.org/10.1111/j.1753-5174.2009.00019.x
Ormseth MJ, Yancey PG, Solus JF (2016) Effect of drug therapy on net cholesterol efflux capacity of high-density lipoprotein-enriched serum in rheumatoid arthritis. Arthritis Rheumatol 68:2099–2105.
O’Neill F, Charakida M, Topham E, McLoughlin E, Patel N, Sutill E et al (2017) Anti-inflammatory treatment improves high-density lipoprotein function in rheumatoid arthritis. Heart 103:766–773. https://doi.org/10.1136/heartjnl-2015-308953
Park YB, Choi HK, Kim MY (2002) Effects of antirheumatic therapy on serum lipid levels in patients with rheumatoid arthritis: a prospective study. Am J Med 113:188–193. https://doi.org/10.1016/S0002-9343(02)01186-5
RondaN GD, Adorni MP (2015) Newly identified antiatherosclerotic activity of methotrexate and adalimumab: complementary effects on lipoprotein function and macrophage cholesterol metabolism. Arthritis Rheumatol 67:1155–1164. https://doi.org/10.1002/art.39039
Rodriguez-Jimenez NA, Garcia-Gonzalez CE, Ayala-Lopez KP (2014) Modifications in lipid levels are independent of serum TNF-alpha in rheumatoid arthritis: results of an observational 24-week cohort study comparing patients receiving etanercept plus methotrexate or methotrexate as monotherapy. Biomed Res Int. https://doi.org/10.1155/2014/510305
Charles-Schoeman C, Wang X, Lee YY (2016) Association of triple therapy with improvement in cholesterol profiles over two-year follow up in the treatment of early aggressive rheumatoid arthritis trial. Arthritis Rheumatol 68:577–586. https://doi.org/10.1002/art.39502
Popa C, van den Hoogen FHJ, Radstake TRDJ, Netea MG, Eijsbouts AE et al (2007) Modulation of lipoprotein plasma concentrations during long-term anti-TNF therapy in patients with active rheumatoid arthritis. Ann Rheum Dis 66:1503–1507. https://doi.org/10.1136/ard.2006.066191
Wijbrandts CA, Leuven SI, Boom HD, Gerlag DM, Stroes EG, Kastelein JJ et al (2009) Sustained changes in lipid profile and macrophage migration inhibitory factor levels after anti-tumor necrosis factor therapy in rheumatoid arthritis. Ann Rheum Dis 68:1316–1321. https://doi.org/10.1136/ard.2007.086728
Kiortsis DN, Mavridis AK, Filippatos TD, Vasakos S, Nikas SN, Drosos AA (2006) Effects of infliximab treatment on lipoprotein profile in patients with rheumatoid arthritis and ankylosing spondylitis. J Rheumatol 33:921–923
Bergström U, Jovinge S, Persson J, Jacobsson L (2018) Effects of treatment with adalimumab on blood lipid levels and atherosclerosis in patients with rheumatoid arthritis. Curr Ther Res Clin Exp 89:1–6. https://doi.org/10.1016/j.curtheres.2018.07.001
Seriolo B, Paolino S, Sulli A, Fasciolo D, Cutolo M (2006) Effects of anti-TNF-alpha treatment on lipid profile in patients with active rheumatoid arthritis. Ann N Y Acad Sci 1069:414–419. https://doi.org/10.1196/annals.1351.039
Daïen CI, Duny Y, Barnetche T, Daurès JP, Combe B, Morel J (2012) Effect of TNF inhibitors on lipid profile in rheumatoid arthritis: a systematic review with meta-analysis. Ann Rheum Dis 71:862–868. https://doi.org/10.1136/annrheumdis-2011-201148
Van Sijl AM, Peters MJ, Knol DL, de Vet RH, Sattar N, Dijkmans BA et al (2011) The effect of TNF-α blocking therapy on lipid levels in rheumatoid arthritis: a meta-analysis. Semin Arthritis Rheum 41:393–400. https://doi.org/10.1016/j.semarthrit.2011.04.003
Di Minno MN, Ambrosino P, Peluso R, Di Minno A, Lupoli R, Dentali F, CaRRDs Study Group (2014) Lipid profile changes in patients with rheumatic diseases receiving a treatment with TNF-α blockers: a meta-analysis of prospective studies. Ann Med 6:73–83
Cacciapaglia F, Anelli MG, Rinaldi A, Serafino L, Covelli M, Scioscia C et al (2014) Lipid profile of rheumatoid arthritis patients treated with anti-tumor necrosis factor-alpha drugs changes according to disease activity and predicts clinical response. Drug Dev Res 75(Suppl 1):S77–80. https://doi.org/10.1002/ddr.21203
Végh E, Kerekes G, Pusztai A, Hamar A, Szamosi S, Váncsa A et al (2020) Effects of 1-year anti-TNF-α therapy on vascular function in rheumatoid arthritis and ankylosing spondylitis. Rheumatol Int 40:427–436. https://doi.org/10.1007/s00296-019-04497-0
Kiortsis DN, Mavridis AK, Vasakos S, Nikas SN, Drosos AA (2005) Effects of infliximab treatment on insulin resistance in patients with rheumatoid arthritis and ankylosing spondylitis. Ann Rheum Dis 64:765–766. https://doi.org/10.1136/ard.2004.026534
Hashizume M, Yoshida H, Koike N, Suzuki M, Mihara M (2010) Overproduced interleukin 6 decreases blood lipid levels via upregulation of very-low-density lipoprotein receptor. Ann Rheum Dis 69:741–746. https://doi.org/10.1136/ard.2008.104844
Cacciapaglia F, Anelli MG, Rinaldi A, Fornaro M, Lopalco G, Scioscia C et al (2018) Lipids and atherogenic indices fluctuation in rheumatoid arthritis patients on long-term tocilizumab treatment. Mediat Inflamm. https://doi.org/10.1155/2018/2453265
Kawashiri SY, Kawakami A, Yamasaki S, Imazato T, Iwamoto N, Fujikawa K et al (2011) Effects of the anti-interleukin-6 receptor antibody, tocilizumab, on serum lipid levels in patients with rheumatoid arthritis. Rheumatol Int 31:451–456. https://doi.org/10.1007/s00296-009-1303-y
Fleischmann R, Kremer J, Cush J, Schulze-Koops H, Connell CA, Bradley JD et al (2012) Placebo-controlled trial of tofacitinib monotherapy in rheumatoid arthritis. N Engl J Med 367:495–507. https://doi.org/10.1056/NEJMoa1109071
Chen DY, Chen YM, Hsieh TY, Hsieh CW, Lin CC, Lan JL (2015) Significant effects of biologic therapy on lipid profiles and insulin resistance in patients with rheumatoid arthritis. Arthritis Res Ther 17:52. https://doi.org/10.1186/s13075-015-0559-8
Charles-Schoeman C, Gonzalez-Gay MA, Kaplan I, Boy M, Geier J, Luo Z et al (2016) Effects of tofacitinib and other DMARDs on lipid profiles in rheumatoid arthritis: implications for the rheumatologist. Semin Arthritis Rheum 46:71–80. https://doi.org/10.1016/j.semarthrit.2016.03.004
Novikova DS, Popkova TV, Lukina GV, Luchikhina EL, Karateev DE, Volkov AV et al (2016) The effects of rituximab on lipids, arterial stiffness and carotid intima-media thickness in rheumatoid arthritis. J Korean Med Sci 31:202–207.
Kerekes G, Soltész P, Dér H, Veres K, Szabó Z, Végvári A et al (2009) Effects of rituximab treatment on endothelial dysfunction, carotid atherosclerosis, and lipid profile in rheumatoid arthritis. Clin Rheumatol 28:705–710. https://doi.org/10.1007/s10067-009-1095-1
Mathieu S, Pereira B, Dubost JJ, Lusson JR, Soubrier M (2012) No significant change in arterial stiffness in RA after 6 months and 1 year of rituximab treatment. Rheumatology (Oxford) 51:1107–1111. https://doi.org/10.1093/rheumatology/kes006
Ridker PM, Cook NR (2013) Statins: new American guidelines for prevention of cardiovascular disease. Lancet 382:1762–1765. https://doi.org/10.1016/S0140-6736(13)62388-0
Kitas GD, Nightingale P, Armitage J, Sattar N, Belch JJ, Symmons DPM (2019) A multicenter, randomized, placebo-controlled trial of atorvastatin for the primary prevention of cardiovascular events in patients with rheumatoid arthritis. Arthritis Rheumatol 71:1437–1449. https://doi.org/10.1002/art.40892
An J, Alemao E, Reynolds K, Kawabata H, Solomon DH, Liao KP et al (2016) Cardiovascular outcomes associated with lowering low-density lipoprotein cholesterol in rheumatoid arthritis and matched nonrheumatoid arthritis. J Rheumatol 43:1989–1996. https://doi.org/10.3899/jrheum.160110
Jafri K, Taylor L, Nezamzadeh M, Baker JF, Mehta NN, Bartels C et al (2015) Management of hyperlipidemia among patients with rheumatoid arthritis in the primary care setting. BMC Musculoskelet Disord 16:237. https://doi.org/10.1186/s12891-015-0700-5
Acknowledgements
All authors declare that no part of this review, including graphics, ideas, and text, is copied or published elsewhere and that all co-authors take full responsibility for the integrity of the review.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
All authors made substantial contributions and approved the final version of the manuscript. (AIV and EP: drafting; PVV: review; AAD: conception and design of the work, review).
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Venetsanopoulou, A.I., Pelechas, E., Voulgari, P.V. et al. The lipid paradox in rheumatoid arthritis: the dark horse of the augmented cardiovascular risk. Rheumatol Int 40, 1181–1191 (2020). https://doi.org/10.1007/s00296-020-04616-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-020-04616-2