
Abstract
To evaluate the association between the index and ring finger’s (2D:4D) length ratio with the prevalence and severity of radiographic hand osteoarthritis (OA). A population-based sample included 802 males (mean age 46.98 ± 17.10 years) and 738 females (mean age 48.65 ± 16.62 years) who had participated in a Chuvashian skeletal aging study. Age, sex, basic demographics, anthropometric data and X-rays of both hands were acquired. Each hand was visually classified on X-ray as either type 1—index finger longer than the ring finger; type 2—index and ring finger equal in length; or type 3—index finger shorter than the ring finger. Hand OA was defined by the number of affected joints (Kellgren–Lawrence score ≥ 2) in both hands and the sum total of Kellgren–Lawrence scores (total OA score). After comparing the OA variables of individuals with different finger length ratio types (after adjustment for age and BMI) significant differences were found only in females between finger ratio types of the right hand in a number of affected joints (F = 3.153, p = 0.043) and finger ratio types of the left (F = 3.330, p = 0.036) and right (F = 2.397, p = 0.047) hands of the total OA score. Females with type 3 ratios had the highest adjusted values of hand OA parameters. We found that finger length ratios are associated with hand OA parameters. Females with a type 3 finger length pattern showed significantly higher hand OA values than those with types 1 and 2.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
It has been established that the index to ring finger ratio or 2D:4D ratio is a reliable biomarker of testosterone exposure during early intra-uterine life [1,2,3]. During the last decade, the 2D:4D ratio has been examined in relation to a number of physiological processes and psychological aspects [3], sporting abilities [4, 5] and diverse health conditions [6, 7].
Finger length ratio was also found to be associated with skeletal variables such as bone mineral density [8] and osteoarthritis (OA) in various sites of the body [9,10,11,12]. The type 3 finger length pattern of the index to ring finger ratio, i.e., low ratio or “male” pattern was found associated, to a statistically significant degree, with OA [10,11,12,13]. Sigurjonsdottir et al. [11] found that the type 3 finger ratio was associated with total knee replacements but not total hip replacements. The underlying mechanism for such findings is unknown.
We carried out a radiographic study on a large population sample who had participated in a Chuvashian skeletal aging study project, investigating different aspects of skeletal aging within a Chuvashian population [14]. The aim of this study was to evaluate the association between the index to ring finger (2D: 4D) length ratio and the severity of radiographic hand OA.
Methods
Study design
A cross-sectional population-based analytic study.
Sample
The population sampled was native Chuvashians residing in numerous small villages in the Chuvasha and Bashkortostan Autonomy regions of the Russian Federation. The Chuvashians participating in this investigation were randomly chosen volunteers described in detail elsewhere [15, 16]. The study cohort included 802 males, aged 18–89 years and 738 females, aged 18–90 years. The data collected included sex, age, anthropometrical characteristics (height, weight), occupation, as well as the nature and extent of their physical activities and details on their chronic morbidity and medical treatments. Excluded from the study were individuals with known bone diseases, amenorrhea, post-traumatic, rheumatoid or psoriatic arthritis, as well as intake of hormone replacement therapy or steroids. X-ray films of both hands were obtained from the study participants in addition to the necessary examinations, measurements, and interviews. All these procedures were consensual. The subjects signed an informed consent form. The entire project was approved by the Helsinki Ethics Committee, Tel Aviv University.
Body mass index (BMI)
BMI was computed as the ratio of weight (in kg) divided by height (in meters) squared.
Hand radiographs
Single plain radiographs of both hands using a standard roentgenographic technique as described in detail by Pavlovsky and Kobyliansky were taken in the posteroanterior position with an X-ray source located 60 cm above the patient [17, 18]. Hands were placed on the same film-containing plate to avoid any film or development variation and exposed for 5–10 s at 100–150 mA without intensifying screens at 50 kV. All X-rays were digitized. The radiographic measurements were performed using digital images.
Visual classification of finger length ratio
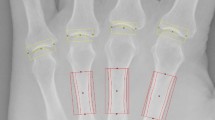
All X-rays were evaluated by an experienced radiological researcher (L.K.). Each hand was classified according to the length of the index finger; longer (Type 1), equal to (Type 2) or shorter than the ring finger (Type 3), by visual comparison of the soft tissue outline of the fingertips on the radiograph. As in a study of Robertson et al. [19], X-ray findings were classified as ‘definite’ or ‘probable’ according to the certainty of the observer. Each X-ray classified as “probable” was assessed by an additional reader and a consensus classification was recorded. Inter-reader correlation was high (κ = 0.86).
The data on actual finger (2D:4D) length ratio in Chuvash population was presented in details in our previous publication [20].
Radiographic assessment of OA
Each radiograph was read by an experienced and specially trained physician. The development of OA was evaluated for each of the 14 joints (4 DIP, 4 PIP, 5 MP, and IP-1) according to the Kellgren and Lawrence (K–L) grading scheme, which utilizes photographs from the Atlas of Standard Radiographs [21]. The extent of each of the above-mentioned indexes for each joint, ranged from 0 to 4. Joints scored as K–L ≥ 2 were considered affected. Each individual was characterized by the total number of affected joints and total OA score (total sum of K–L scores of all 28 joints of both hands). Summing up K–L scores of the hand joints in evaluating hand OA is common in epidemiological studies [22,23,24]. In addition, we divided all subjects to ones with vs. ones without hand OA (at least one joint with K–L ≥ 2).
Reliability of OA assessment
Initially, two experienced researchers (an orthopedic surgeon and a physician experienced in interpreting X-rays) read a batch of radiographs and decided on the protocol for evaluating the K–L scores. 10 X-rays were read using this protocol and then re-read by two separate investigators to estimate the intra- and inter-rater reliability of the readings. All discrepancies were reviewed for systematic errors. This exercise continued until the reliability was high (ICC > 0.8). Once high intra-rater and inter-rater reliability was established, one investigator still blinded to patient identifiers and patients’ ages, read all the X-rays. The intra-observer reliability (kappa statistics) was 0.85 (p < 0.01).
Statistical analysis
All statistical computations were performed using SPSS 17.0 for Windows (SPSS, Chicago, IL, USA). Mean and standard deviation for age and body mass index (BMI) measurements and frequencies of visual classification types were calculated separately, for each sex, using descriptive statistics. To compare the continuous variables (age, BMI, the number of affected joints and total OA score) between the males and females a one-way analysis of variance (ANOVA) was used; to compare the finger ratio types, the Pearson’s Chi-square test was used; to test the association between OA variables (number of affected joints and total OA score) and age and BMI, the Pearson correlation analysis was used; to test the association between OA variables (number of affected joints and total OA score) and age and BMI and to compare the OA variables between individuals with different finger length ratio types (after adjustment for age and BMI) a one-way analysis of covariance (ANCOVA) was used. These analyses were performed four times, separately for males and females and for finger length ratio types of right and left hands.
In addition, to test the association between finger length ratios and hand OA traits we performed two linear regression analyses, with number of affected joints and total OA score as dependent variables and age, sex, BMI and right and left finger ratios as independent predictors, and one bivariate logistic regression analysis with dichotomous variable of presence or absence of hand OA (at least one joint with K–L ≥ 2) as a dependent variable and same independent predictors.
Results
The study sample (Table 1) included 802 males (mean age 46.98 ± 17.10 years) and 783 females (mean age 48.65 ± 16.62 years) (age difference between males and females was not significant p = 0.053). The male BMI (23.19 ± 3.26 kg/m2) was lower than the female BMI (25.16 ± 4.87 kg/m2) (p < 0.001). Females exhibited a significantly higher number of affected joints (p = 0.039) and total OA score (p = 0.001).
Distribution of finger length ratio types in the studied sample is shown in Table 2. No significant differences (p > 0.05) in the prevalence of each type of finger ratio in males and in females were shown between the right and left hand. However, when comparing the distribution of finger length ratio types between males and females, a significant difference was observed (d.f. = 2, χ 2 = 11.769, p = 0.003) in the right hand with no significant differences (d.f. = 2, χ 2 = 5.107, p = 0.078) in the left.
Distribution of hand OA traits in the studied sample according to the age groups and sex is shown in Table 3. A number of affected joints, total OA score, and proportion of subjects with at least one affected joint, all gradually increased with age, especially after the 5th decade in males and females. Even, as we mentioned before, females had significantly higher number of affected joints than males (Table 1), in Table 3 one can see that until age 50, females had a lower number of affected joints than males, and the situation changed after 5th decade. Interestingly, almost all males after age 70 and females after age 60 had at least one joint with hand OA.
Hand OA parameters showed significant positive correlations (p < 0.001 for both variables) with age and BMI (Table 4). Results of comparisons of OA variables between individuals with different finger length ratio types (after adjustment for age and BMI) are shown in Table 5. In unadjusted data, the highest values of a number of affected joints and the total OA score was seen in individuals (males and females) with a type 3 (2 < 4) finger ratio. However, when adjusted for age and BMI, significant differences were seen only in females between finger ratio types of the right hand in a number of affected joints (F = 3.153, p = 0.043) and finger ratio types of the left (F = 3.330, p = 0.036) and right (F = 2.397, p = 0.047) hands. Females with a type 3 ratio displayed the highest adjusted values of hand OA parameters.
Linear regression analyses showed that after adjustment for age, sex and BMI, right finger length ratio showed significant positive association with total OA score (beta = 0.38, p = 0.040) and with a number of affected joints (beta = 0.50, p = 0.046). No association was found between left finger length ratio and hand OA traits. In a logistic regression analysis, no association was found between the dichotomous variable of presence or absence of hand OA and finger length ratios.
Discussion
In this large population-based study, a significant association between type 3 finger ratios and the severity of radiographic hand OA in females was observed. The association is independent of other established risk factors for OA, such as age and BMI.
Previous studies have shown diverse results. A large population-based Icelandic study [11] showed no association between type 3 ratio and hand OA. In this study, hand OA was assessed by hand photographs, not X-rays, which may explain the different results. Haugen et al. [25] in a Framingham community cohort study, found a significant association between a low 2D:4D ratio (similar to a type 3 pattern) and hand OA in females, but not in males. Similarly, another large population-based study from the Netherlands [10] also found that the type 3 finger length pattern was associated with the prevalence of radiographic hand OA. Thus, results of our study support the previous findings of an association between hand OA and type 3 finger length ratio patterns in females. Furthermore, this is interesting since we used a different method for defining hand OA.
Theoretically, severe OA could lead to shortening of the digits and an overestimation of the presence of type 3 finger length patterns [10]. However, in our previous study performed on the same population [26], no differences were found in the degeneration rate or severity between the second and fourth fingers. de Kruijf et al. [10] found that when individuals with severe OA in the second finger were excluded, the association between hand OA and the type 3 finger length ratio, remained significant. The type 3 finger length pattern was also found to be associated with OA in the knees [10,11,12,13] and hips [13].
One of the possible explanations for the association between the type 3 finer ratio and OA is a hormonal mechanism [27]; estrogen, in particular, has a complex and possibly protective relationship with OA [28]. An association of type 3 finger length ratios with hand OA (not weight bearing joints) supports this theory [10]. Testosterone may also be involved in the etiology of OA. Ma et al. [29] conducted in vivo investigations on male mice (orchiectomy versus controls) and determined that intact mice demonstrated more severe OA. Both estrogen and testosterone are also known for their role in bone metabolism [30, 31], however, current evidence does not suggest that the finger length ratio is associated with hormonal levels in adults [32]. Further studies are warranted to understand the mechanism of the association between finger length ratio, especially type 3 and OA. In conclusion, the finger length ratio was found to be associated with hand OA parameters. Females with a type 3 finger length pattern showed significantly higher hand OA values than types 1 and 2.
References
Lutchmaya S, Baron-Cohen S, Raggatt P, Knickmeyer R, Manning JT (2004) 2nd to 4th digit ratios, fetal testosterone and estradiol. Early Hum Dev 77(1–2):23–28. doi:10.1016/j.earlhumdev.2003.12.002
McIntyre MH (2006) The use of digit ratios as markers for perinatal androgen action. Reprod Biol Endocrinol 4:10. doi:10.1186/1477-7827-4-10
Putz D, Gaulin S, Sporter R, McBurney D (2004) Sex hormones and finger length: What does 2D: 4D indicate? Evol Hum Behav 25:182–199
Manning JT, Taylor RP (2001) Second to fourth digit ratio and male ability in sport: implications for sexual selection in humans. Evol Hum Behav 22:61–69
Paul SN, Kato BS, Hunkin JL, Vivekanandan S, Spector TD (2006) The big finger: the second to fourth digit ratio is a predictor of sporting ability in women. Br J Sports Med 40(12):981–983. doi:10.1136/bjsm.2006.027193
Manning JT, Bundred PE (2000) The ratio of 2nd to 4th digit length: a new predictor of disease predisposition? Med Hypotheses 54(5):855–857. doi:10.1054/mehy.1999.1150
Vehmas T, Solovieva S, Leino-Arjas P (2006) Radiographic 2D: 4D index in females: no relation to anthropometric, behavioural, nutritional, health-related, occupational or fertility variables. J Negat Results Biomed 5:12. doi:10.1186/1477-5751-5-12
Arazi H, Eghbali E, Saeedi T, Moghadam R (2016) The relationship of physical activity and anthropometric and physiological characteristics to bone mineral density in postmenopausal women. J Clin Densitom 19(3):382–388. doi:10.1016/j.jocd.2016.01.005
Hussain SM, Wang Y, Muller DC, Wluka AE, Giles GG, Manning JT, Graves S, Cicuttini FM (2014) Association between index-to-ring finger length ratio and risk of severe knee and hip osteoarthritis requiring total joint replacement. Rheumatology (Oxford) 53(7):1200–1207. doi:10.1093/rheumatology/keu021
de Kruijf M, Kerkhof HJ, Peters MJ, Bierma-Zeinstra S, Hofman A, Uitterlinden AG, Huggen FJ, van Meurs JB (2014) Finger length pattern as a biomarker for osteoarthritis and chronic joint pain: a population-based study and meta-analysis after systematic review. Arthritis Care Res (Hoboken) 66(9):1337–1343. doi:10.1002/acr.22320
Sigurjonsdottir K, Bjorgulfsson TM, Aspelund T, Eiriksdottir G, Sigurdsson S, Ingvarsson T, Harris TB, Launer L, Gudnason V, Jonsson H (2013) Type 3 finger length pattern is associated with total knee replacements due to osteoarthritis but not with hip replacements or hand osteoarthritis in the elderly: the AGES-Reykjavik study. BMC Musculoskelet Disord 14:112. doi:10.1186/1471-2474-14-112
Ferraro B, Wilder FV, Leaverton PE (2010) Site specific osteoarthritis and the index to ring finger length ratio. Osteoarthr Cartil 18(3):354–357. doi:10.1016/j.joca.2009.11.001
Zhang W, Robertson J, Doherty S, Liu JJ, Maciewicz RA, Muir KR, Doherty M (2008) Index to ring finger length ratio and the risk of osteoarthritis. Arthritis Rheum 58(1):137–144. doi:10.1002/art.23237
Kalichman L, Malkin I, Livshits G, Kobyliansky E (2006) The association between morbidity and radiographic hand osteoarthritis: a population-based study. Jt Bone Spine 73(4):406–410. doi:10.1016/j.jbspin.2005.11.013
Kalichman L, Cohen Z, Kobyliansky E, Livshits G (2002) Interrelationship between bone aging traits and basic anthropometric characteristics. Am J Hum Biol 14(3):380–390. doi:10.1002/ajhb.10051
Kalichman L, Livshits G, Kobyliansky E (2006) Indices of body composition and chronic morbidity: a cross-sectional study of a rural population in central Russia. Am J Hum Biol 18(3):350–358. doi:10.1002/ajhb.20506
Kobyliansky E, Livshits G, Pavlovsky O (1995) Population biology of human aging: methods of assessment and sex variation. Hum Biol 67(1):87–109
Pavlovsky O, Kobyliansky E (1997) Population biology of human aging angelo pontecorboli editore. Firenze, Italy
Robertson J, Zhang W, Liu JJ, Muir KR, Maciewicz RA, Doherty M (2008) Radiographic assessment of the index to ring finger ratio (2D: 4D) in adults. J Anat 212(1):42–48. doi:10.1111/j.1469-7580.2007.00830.x
Kalichman L, Zorina D, Batsevich V, Kobyliansky E (2013) 2D: 4D finger length ratio in the Chuvashian population. Homo 64(3):233–240. doi:10.1016/j.jchb.2013.02.051
Kellgren J, Lawrence J (1963) Atlas of standard radiographs: the epidemiology of chronic rheumatism, vol 2. Blackwell Scientific Publications, Oxford
Cauley JA, Kwoh CK, Egeland G, Nevitt MC, Cooperstein L, Rohay J, Towers A, Gutai JP (1993) Serum sex hormones and severity of osteoarthritis of the hand. J Rheumatol 20(7):1170–1175
Demissie S, Cupples LA, Myers R, Aliabadi P, Levy D, Felson DT (2002) Genome scan for quantity of hand osteoarthritis: the Framingham Study. Arthritis Rheum 46(4):946–952. doi:10.1002/art.10149
Dominick KL, Jordan JM, Renner JB, Kraus VB (2005) Relationship of radiographic and clinical variables to pinch and grip strength among individuals with osteoarthritis. Arthritis Rheum 52(5):1424–1430. doi:10.1002/art.21035
Haugen IK, Niu J, Aliabadi P, Felson DT, Englund M (2011) The associations between finger length pattern, osteoarthritis, and knee injury: data from the Framingham community cohort. Arthritis Rheum 63(8):2284–2288. doi:10.1002/art.30408
Kalichman L, Kobyliansky E, Livshits G (2006) Characteristics of joint degeneration in hand osteoarthritis. Jt Bone Spine 73(1):72–76. doi:10.1016/j.jbspin.2004.05.018
Linn S, Murtaugh B, Casey E (2012) Role of sex hormones in the development of osteoarthritis. PM & R 4(5 Suppl):S169–S173. doi:10.1016/j.pmrj.2012.01.013
Tanamas SK, Wijethilake P, Wluka AE, Davies-Tuck ML, Urquhart DM, Wang Y, Cicuttini FM (2011) Sex hormones and structural changes in osteoarthritis: a systematic review. Maturitas 69(2):141–156. doi:10.1016/j.maturitas.2011.03.019
Ma HL, Blanchet TJ, Peluso D, Hopkins B, Morris EA, Glasson SS (2007) Osteoarthritis severity is sex dependent in a surgical mouse model. Osteoarthr cartil 15(6):695–700. doi:10.1016/j.joca.2006.11.005
Riggs BL (2000) The mechanisms of estrogen regulation of bone resorption. J Clin Investig 106(10):1203–1204. doi:10.1172/jci11468
Tuck SP, Francis RM (2009) Testosterone, bone and osteoporosis. Front Horm Res 37:123–132. doi:10.1159/000176049
Muller DC, Giles GG, Bassett J, Morris HA, Manning JT, Hopper JL, English DR, Severi G (2011) Second to fourth digit ratio (2D: 4D) and concentrations of circulating sex hormones in adulthood. Reprod Biol Endocrinol 9:57. doi:10.1186/1477-7827-9-57
Acknowledgements
The authors thank Mrs Phyllis Curchack Kornspan for her editorial services.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The author(s) declare that they have no conflicts of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Rights and permissions
About this article

Cite this article
Kalichman, L., Batsevich, V. & Kobyliansky, E. 2D:4D finger length ratio and radiographic hand osteoarthritis. Rheumatol Int 38, 865–870 (2018). https://doi.org/10.1007/s00296-017-3831-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-017-3831-1