
Abstract
The goal of our study was to evaluate the associations between various definitions of radiographic hand osteoarthritis (OA) and self-reported hand pain. We conducted a cross-sectional study with 3604 participants from the Osteoarthritis Initiative (OAI). Posteroanterior radiographs of the dominant hand were read using a modified Kellgren–Lawrence (KL) scale. For our primary analysis, hand OA at person level was defined as two or more finger joints with KL grade 2 or higher. In addition, for the purpose of exploratory analyses, we explored more conservative definitions of hand OA as well as different sum scores and digit- and row-based scores. The majority of definitions of radiographic hand OA were statistically significantly associated with self-reported hand pain. In our main analysis, persons with two or more finger joints with KL grade > 2 were approximately two times more likely to self-report hand pain than persons without radiographic hand OA. Increasing KL grades and increasing number of joints affected lead to stronger associations. Almost all definitions of hand OA were related to pain. Individuals with more severely affected joints or with higher number of affected joints are more likely to report hand pain than their peers. Specifically, individuals with hand joints with KL 3 or 4 have the greatest likelihood of hand pain.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hand osteoarthritis (OA) is a disabling disease that frequently occurs in the general population [1]. The diagnosis of hand OA is based on clinical examination and while the ACR endorsed criteria for hand OA omit radiographic assessments, they are often used to assess disease burden and progression [2]. Hand radiographs are widely available and cheap to obtain [3]. To assess the radiographic features of hand OA several different scoring methods exist [4]. The Kellgren and Lawrence (KL) scoring system is the most widely used one among them [4]. The KL system is based on the main features of radiographic hand OA: joint space narrowing (JSN), osteophytes, subchondral sclerosis and pseudocystic areas [5]. Generally, investigators define radiographic OA at a joint as a KL grade of 2 or higher [1, 6]. However, there are substantial variations in the definitions of overall radiographic hand OA in epidemiological studies [7].
At a person level, most studies have defined radiographic hand OA as having either 1 or more or 2 or more joints with KL grade ≥ 2 [8]. Radiographic hand OA has also been defined with sum scores of KL grades of the whole hand or of individual digits or joint rows [8]. Unfortunately, the sum scores consider all joints equal and might ignore important concepts, such as which joints are affected and the severity of each affected joint.
These various strategies to defining radiographic hand OA contribute to the inconsistent evidence of an association between radiographic hand OA and measures of pain [9,10,11]. A review of 16 articles showed evidence for a positive association between radiographic hand OA and hand pain, but the strength of the association varied between studies [8]. To improve comparability among hand OA studies, it is important to standardize the definitions of radiographic hand OA.
A comprehensive evaluation of the association between hand pain and radiographic hand OA may help researchers and clinicians conceptualize hand OA. Hence, the goal of our study was to evaluate the association of various definitions of radiographic hand OA and hand pain. We used a broad approach and evaluated multiple definitions of hand OA including individual KL grades, sum scores, as well as scores based on digits and rows to determine which definitions may offer stronger associations with hand pain. Our systematic approach will provide valuable information to inform a consensus on a standardized definition of radiographic hand OA, which would reduce variation between studies and enhance the comparability of studies on hand OA [12]. We defined hand pain based on self-reported hand pain as well as self-reported physician-diagnosed hand OA, which reflects hand pain sufficient to warrant medical attention. We hypothesize that individuals with more severely affected joints (higher KL grades) or with more affected joints are more likely to report hand pain or diagnosis than their peers.
Materials and methods
Study design and cohort
To study the association between radiographic hand OA and hand pain, we conducted a cross-sectional study of participants from the Osteoarthritis Initiative (OAI) who had radiographs of the dominant hand and assessment of hand symptoms. The OAI is a longitudinal cohort study of 4796 men and women aged 45–79 years with, or at risk for, knee OA at the beginning of the study (February 2004 and May 2006). The eligibility criteria for the OAI and the OAI protocol are publicly available on the OAI website [13]. For example, a potential participant with rheumatoid arthritis or inflammatory arthritis (defined by self-reported diagnosis and ever use of rheumatoid arthritis-specific medications) was excluded from the OAI. If a potential participant reported being diagnosed but had none of the medications then they were excluded if the responses to questions about symptoms were suggestive of rheumatoid arthritis. The OAI staff also excluded adults with severe knee OA, which was defined as (1) OARSI joint space narrowing grade of 3 in both knees, (2) OARSI joint space narrowing grade of 3 in one knee if the other knee had a total knee replacement, (3) bilateral total knee replacements, or (4) plans to get bilateral total knee replacements within 3 years of starting the study. A person with a MRI contra-indication was also excluded from the OAI (e.g., men over 285 pounds, women over 250 pounds). Specific to this project, we excluded OAI participants without radiographs of the dominant hand (n = 1180, 24.6%). Another 10 participants had hand radiographs that were of insufficient quality to score. Two participants were omitted from the study due to coding errors. See Fig. 1 for a flowchart of the study. Institutional review boards at the OAI clinical sites and the coordinating center (University of California, San Francisco) approved the OAI study (University of California Internal Review Board Approval Number 10–00532, Approval Date: 2/24/2017, Expiration Date: 2/23/2018). All participants provided informed consent.

Flow chart of the study. OAI Osteoarthritis Initiative, n = number
Definition of dominant hand
To determine the dominant hand, the OAI staff asked 95% of the study participants if they were right or left handed. If a participant answered ambidextrous or unknown or if data was missing and the person had unilateral hand radiographs that hand was selected (4% of sample). If a participant answered ambidextrous or unknown or if data were missing and the person had bilateral hand radiographs, we selected the dominant hand based on the ipsilateral hand to the foot a person reported using to kick a ball (1% of sample).
Hand radiograph reading procedure
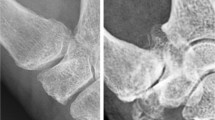
One investigator (LFS) read the posteroanterior radiographs of the dominant hand using a custom software-based data entry tool, which displays the two images side by side but blinds the reader to time-point. The software offered a graphical user interface (GUI) for electronic scoring. In total, 16 joints per hand were scored: 2nd–5th distal interphalangeal (DIP) joints, 2nd–5th proximal interphalangeal (PIP) joints, 1st–5th metacarpophalangeal (MCP) joints, thumb interphalangeal (IP) joint, and the thumb base joints (i.e., first carpometacarpal (CMC-1) joint and the scaphotrapezial (ST) joint). The joints were scored according to the modified Kellgren–Lawrence (KL) scale that was used in the Framingham Study [1]:
KL grade 0: no osteoarthritis (OA), i.e. no osteophyte or joint space narrowing.
KL grade 1: minimal OA, i.e. questionable osteophyte and/or joint space narrowing.
KL grade 2: mild OA, i.e. small osteophyte(s) and/or mild joint space narrowing, sclerosis may be present.
KL grade 3: moderate OA, i.e. moderate osteophyte(s) and/or moderate joint-space narrowing, sclerosis and erosions may be present.
KL grade 4: severe OA, i.e. large osteophyte(s) and/or severe joint-space narrowing, sclerosis and erosions may be present.
The reader scored 100 randomly selected pairs of hand radiographs twice. Intra-reader agreement, based on weighted kappas, was good (weighted kappa > 0.84).
Definition of hand OA
For our primary analysis, radiographic hand OA at person level was defined as persons with two or more finger joints (DIP, PIP, MCP joints) with KL grade 2 or higher. To reduce misclassification due to the presence of post-traumatic OA, the joint involvement had to be present in at least two separate digits. We repeated the analyses with inclusion of the thumb base. Thumb base OA was defined as KL grade of 2 or higher in either the first CMC or the ST joint.
For the purpose of exploratory analyses, we explored more conservative definitions of hand OA as well as different sum scores of KL grades and their associations with self-reported hand pain. We calculated sum scores of all joints within one hand, all joints without the thumb base joints (first CMC and ST joint), and the thumb base joints alone. We also analyzed the number of joints with mild (KL = 2), moderate (KL = 3), or severe (KL = 4) OA within the entire hand, each digit, and across three rows (DIP row, PIP row and MCP row; Tables 2, 3, 4).
OAI hand pain variables
Self-reported hand or finger pain was defined based on a homunculus with the question “During the past 30 days, which of these joints have had pain, aching, or stiffness on most days? By most days, we mean more than half the days of a month.” Participants indicated left or right hand pain. Self-reported physician-diagnosed hand OA was based on the response to “Has a doctor ever told you that you have osteoarthritis or degenerative arthritis in your hand or fingers?”. This variable is publicly available at the OAI website.
Statistical methods
To explore the association between various definitions of radiographic hand OA (predictor) and self-reported hand pain (outcome), we performed a series of logistic regression models. We calculated unadjusted and adjusted odds ratios (OR) with 95% confidence intervals (CI) to assess the likelihood that persons with radiographic hand OA would have self-reported hand pain at baseline compared with persons without radiographic hand OA. Models were adjusted for baseline age, sex, race, and baseline body mass index. We used Poisson distribution to model the count-like data for the sum scores of all joints within one hand, all joints without the thumb base joints (first CMC and ST joint) and the thumb base joints alone. Finally, we determined the set of structural characteristics that was most strongly associated with hand pain using area-under-the receiver operating characteristics curves (AUC) to evaluate the performance of model prediction for each pathway and outcome.
We performed the described analyses also considering self-reported physician-diagnosed hand OA as an outcome.
Results
The demographic characteristics for the 3604 subjects are given in Table 1.
Hand pain and radiographic OA within the entire hand
All definitions of radiographic hand OA were statistically significantly associated with hand pain (Tables 2, 3, 4). In our main analyses, persons with two or more finger joints with KL grade ≥ 2 at different digits (including or excluding the thumb base) were approximately two times more likely to self-report hand pain than persons without radiographic hand OA (Table 2). For the thumb base alone, the result was similar (OR = 1.74; 95% CI = 1.46–2.08). When we summed the KL scores, we found that for each increase in KL grade a person was 33 to 51% more likely to report pain.
When we defined radiographic severity based on the number of joints involved with a specific minimum KL grade, the association between radiographic hand OA and self-reported pain tended to be greater when more joints were affected and when we used higher KL grades to define radiographic hand OA (Table 2). People were 2.09–2.48, 4.40–8.30, or 3.73–6.78 times more likely to report hand pain if we required at least two or five joints with KL ≥ 2, KL ≥ 3, or KL = 4, respectively (Table 2).
For the adjusted AUC analysis, the sum scores provided lower correlation with pain than the other groups (sum of all joints: OR = 1.48; 95% CI = 1.44–1.51).
For ROC curves of the results see Fig. 2.

Receiver operating characteristics (ROC) curves of the results. KL Kellgren–Lawrence
Hand pain and radiographic OA by digit and row
For the single-digit analyses, the association with pain was similar for all five digits (Table 3). Similarly, we found that the association between radiographic hand OA severity and self-reported pain was similar for the three rows (DIP row, PIP row, MCP row; Table 4). The association between radiographic hand OA severity and self-reported pain tended to be greater when more joints were affected within each digit or within each row and when we used higher KL grades to define radiographic hand OA (Tables 3, 4). This was confirmed by the AUC analysis, with higher AUC values for KL grades of 3 or 4. However, when we used more stringent criteria to define radiographic hand OA the confidence intervals (95% CI) widened due to a decrease in the size of the subgroups.
For ROC curves of the results see Fig. 2.
Physician-diagnosed hand OA
The majority of the different definitions of radiographic hand OA were statistically significantly associated with self-reported physician-diagnosed hand OA. The patterns were similar as for hand pain, but with slightly higher ORs for physician-diagnosed hand OA.
Discussion
In summary, almost all definitions of radiographic hand OA severity were statistically significantly associated with self-reported hand pain. This highlights the value of reading hand X-rays for the assessment of hand OA. Increasing disease severity (KL grades) or increasing number of joints affected lead to stronger associations. Hence, investigators may define radiographic hand OA based on the number of joints affected or higher KL grades indiscriminate of row or digit within a hand. However, as we required increasing number of joints affected the sample size dwindled quickly. For the digit- and row-based analyses, the AUC analysis emphasized the stronger association of advance-stage disease (KL grades 3 and 4) with hand pain. Nevertheless, the association is still significant for KL 2 and a definition merely based on advance-stage disease would misclassify a substantial number of individuals.
Several cross-sectional studies have investigated the association between radiographic hand OA and pain, but the results are inconsistent [9, 10]. A review of 16 articles suggested that radiographic hand OA was associated with hand pain, but the strength of the association varied between studies [8]. Our study with its large number of participants showed a strong and consistent association of radiographic hand OA with hand pain and, therefore, supports this association.
Our results complement prior studies that found a dose-dependent correlation of hand pain with radiographic hand OA severity, which accounted for the number of joints affected and higher KL grades [11, 14, 15]. However, our results contradicted prior findings that the strongest relation with pain was with thumb base OA [11]. In another study [16], the investigators reported the strongest correlation of hand pain with combined radiographic thumb and finger OA. Meanwhile, individuals with thumb only OA and the finger only OA had similar mean pain scores. In our analysis, we were unable to confirm that the presence of thumb base OA with finger-based OA led to stronger associations with hand pain compared to definitions that examined the thumb and fingers separately. Contrasting results may relate to different study populations and the use of different outcome measures. In the current study, we used self-reported hand pain without information about pain in different situations. Healthy thumb base joints are important for performance of several daily activities, and thumb base OA may lead to pain when performing specific activities. Specific hand OA questionnaires, such as the AUSCAN, include questions about pain in different situations. A limitation to our data is that the job details of the participants are unknown. Physical work with the hands can lead to minor repetitive trauma. This could be a potential risk factor for hand pain. Despite this, we still observed consistent associations between hand pain and radiographic hand OA.
Limitations
While our study offers an in-depth analysis of the association between radiographic hand OA severity and hand pain, it is important to acknowledge some limitations. We used a nonspecific question on hand pain that could include pain attributable to other musculoskeletal complaints. This could cause us to underestimate the true association between hand pain and radiographic hand OA severity. Despite the possibility that we underestimated this association, we found consistent associations between radiographic hand OA severity and hand pain. Another limitation is a potential selection bias since we did not use data from a population-based cohort study but from a preselected sample of individuals with or at risk for knee OA. Nevertheless, the OAI is a publicly available cohort, which gave us the opportunity to study a large sample size of subjects.
In summary, we consistently found an association between radiographic hand OA severity and self-reported hand pain. This highlights the value of reading hand X-rays for the assessment of hand OA. Individuals with more severely affected joints (higher KL grades) or with more affected joints are more likely to report hand pain than their peers. Specifically, individuals with hand joints with advance-stage disease (KL 3 or 4) may have the greatest likelihood of hand pain. Hence, investigators may define radiographic hand OA based on the number of joints affected or higher KL grades indiscriminate of row or digit within a hand. Nevertheless, the association is still significant for KL 2 and a definition merely based on advance-stage disease would misclassify a substantial amount of individuals.
References
Haugen IK, Englund M, Aliabadi P, Niu J, Clancy M, Kvien TK, Felson DT (2011) Prevalence, incidence and progression of hand osteoarthritis in the general population: the Framingham Osteoarthritis Study. Ann Rheum Dis 70(9):1581–1586. https://doi.org/10.1136/ard.2011.150078
Altman R, Alarcon G, Appelrouth D, Bloch D, Borenstein D, Brandt K, Brown C, Cooke TD, Daniel W, Gray R et al (1990) The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hand. Arthritis Rheum 33(11):1601–1610
Hunter DJ, Arden N, Cicuttini F, Crema MD, Dardzinski B, Duryea J, Guermazi A, Haugen IK, Kloppenburg M, Maheu E, Miller CG, Martel-Pelletier J, Ochoa-Albiztegui RE, Pelletier JP, Peterfy C, Roemer F, Gold GE (2015) OARSI Clinical Trials Recommendations: hand imaging in clinical trials in osteoarthritis. Osteoarthr Cartil 23(5):732–746. https://doi.org/10.1016/j.joca.2015.03.003
Visser AW, Boyesen P, Haugen IK, Schoones JW, van der Heijde DM, Rosendaal FR, Kloppenburg M (2014) Radiographic scoring methods in hand osteoarthritis–a systematic literature search and descriptive review. Osteoarthr Cartil 22(10):1710–1723. https://doi.org/10.1016/j.joca.2014.05.026
Kellgren J, Lawrence J (1957) Radiological assessment of osteo-arthrosis. Ann Rheum Dis 16(4):494–502
Niu J, Zhang Y, LaValley M, Chaisson CE, Aliabadi P, Felson DT (2003) Symmetry and clustering of symptomatic hand osteoarthritis in elderly men and women: the Framingham Study. Rheumatology 42(2):343–348
Kerkhof HJ, Meulenbelt I, Akune T, Arden NK, Aromaa A, Bierma-Zeinstra SM, Carr A, Cooper C, Dai J, Doherty M, Doherty SA, Felson D, Gonzalez A, Gordon A, Harilainen A, Hart DJ, Hauksson VB, Heliovaara M, Hofman A, Ikegawa S, Ingvarsson T, Jiang Q, Jonsson H, Jonsdottir I, Kawaguchi H, Kloppenburg M, Kujala UM, Lane NE, Leino-Arjas P, Lohmander LS, Luyten FP, Malizos KN, Nakajima M, Nevitt MC, Pols HA, Rivadeneira F, Shi D, Slagboom E, Spector TD, Stefansson K, Sudo A, Tamm A, Tamm AE, Tsezou A, Uchida A, Uitterlinden AG, Wilkinson JM, Yoshimura N, Valdes AM, van Meurs JB (2011) Recommendations for standardization and phenotype definitions in genetic studies of osteoarthritis: the TREAT-OA consortium. Osteoarthr Cartil 19(3):254–264. https://doi.org/10.1016/j.joca.2010.10.027
Dahaghin S, Bierma-Zeinstra SM, Hazes JM, Koes BW (2006) Clinical burden of radiographic hand osteoarthritis: a systematic appraisal. Arthritis Rheum 55(4):636–647. https://doi.org/10.1002/art.22109
Jones G, Cooley HM, Bellamy N (2001) A cross-sectional study of the association between Heberden’s nodes, radiographic osteoarthritis of the hands, grip strength, disability and pain. Osteoarthr Cartil 9(7):606–611. https://doi.org/10.1053/joca.2001.0460
Hart D, Spector T, Egger P, Coggon D, Cooper C (1994) Defining osteoarthritis of the hand for epidemiological studies: the Chingford Study. Ann Rheum Dis 53(4):220–223
Dahaghin S, Bierma-Zeinstra SM, Ginai AZ, Pols HA, Hazes JM, Koes BW (2005) Prevalence and pattern of radiographic hand osteoarthritis and association with pain and disability (the Rotterdam study). Ann Rheum Dis 64(5):682–687. https://doi.org/10.1136/ard.2004.023564
Haugen IK, Boyesen P (2011) Imaging modalities in hand osteoarthritis–and perspectives of conventional radiography, magnetic resonance imaging, and ultrasonography. Arthritis Res Ther 13(6):248. https://doi.org/10.1186/ar3509
The Osteoarthritis Initiative (2014). http://oai.epi-ucsf.org/. Accessed 2 Apr 2016
Haugen IK, Slatkowsky-Christensen B, Boyesen P, van der Heijde D, Kvien TK (2013) Cross-sectional and longitudinal associations between radiographic features and measures of pain and physical function in hand osteoarthritis. Osteoarthr Cartil 21(9):1191–1198. https://doi.org/10.1016/j.joca.2013.04.004
Kodama R, Muraki S, Oka H, Iidaka T, Teraguchi M, Kagotani R, Asai Y, Yoshida M, Morizaki Y, Tanaka S, Kawaguchi H, Nakamura K, Akune T, Yoshimura N (2016) Prevalence of hand osteoarthritis and its relationship to hand pain and grip strength in Japan: the third survey of the ROAD study. Mod Rheumatol:1–7. https://doi.org/10.3109/14397595.2015.1130673
Marshall M, van der Windt D, Nicholls E, Myers H, Hay E, Dziedzic K (2009) Radiographic hand osteoarthritis: patterns and associations with hand pain and function in a community-dwelling sample. Osteoarthr Cartil 17(11):1440–1447. https://doi.org/10.1016/j.joca.2009.05.009
Funding
These analyses were financially supported by a grant from the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health under Award Number R01-AR066378. The OAI is a public–private partnership comprised of five contracts (N01-AR-2-2258; N01-AR-2-2259; N01-AR-2-2260; N01-AR-2-2261; N01-AR-2-2262) funded by the National Institutes of Health, a branch of the Department of Health and Human Services, and conducted by the OAI Study Investigators. Private funding partners include Merck Research Laboratories; Novartis Pharmaceuticals Corporation, GlaxoSmithKline; and Pfizer, Inc. Private sector funding for the OAI is managed by the Foundation for the National Institutes of Health. This manuscript was prepared using an OAI public use data set and does not necessarily reflect the opinions or views of the OAI investigators, the NIH, or the private funding partners.
Author information
Authors and Affiliations
Contributions
Study conception and design—TEM, JBD, CBE. Acquisition of data—JD, LFS, SES, IKH. Analysis and interpretation of data—JD, LFS, SES, TEM, JBD, CBE, MBR, IKH. Drafting the article or revising it critically for important intellectual content—JD, LFS, SES, TEM, JBD, CBE, MBR, IKH. Final approval of the version of the article to be published—JD, LFS, SES, TEM, JBD, CBE, MBR, IKH. LFS (lenafranziskaschaefer@yahoo.com) takes responsibility for the integrity of the work as a whole.
Corresponding author
Ethics declarations
Ethical approval
Institutional review boards at the OAI clinical sites and the coordinating center (University of California, San Francisco) approved the OAI study (University of California Internal Review Board Approval Number 10–00532, Approval Date: 2/24/2017 Expiration Date: 2/23/2018).
Informed consent
All participants provided informed consent.
Conflict of interest
Dr. Haugen reports personal fees from Abbvie outside the submitted work. Dr. McAlindon reports personal fees from Sanofi Aventis, Samumed, Regeneron, Federal Trade Commission, Seikagaku Corp, Astellas, Pfizer and Tufts Medical Center Physicians Organization outside the submitted work and fees to his institution from Sanofi, Samumed, Allergan and Abbvie outside the submitted work. He also reports a patent: #7,251,609: Online Clinical Trial Methodology outside the submitted work. All other authors declare that they have no conflicting interests.
Rights and permissions
About this article

Cite this article
Schaefer, L.F., McAlindon, T.E., Eaton, C.B. et al. The associations between radiographic hand osteoarthritis definitions and hand pain: data from the osteoarthritis initiative. Rheumatol Int 38, 403–413 (2018). https://doi.org/10.1007/s00296-017-3913-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-017-3913-0