
Abstract
A once-daily modified release formulation of oral tacrolimus (Tac QD) has been developed in response to the problem of nonadherence. However, there have been no data available about the efficacy of Tac QD conversion from intravenous Tac (Tac i.v.) in allogeneic hematopoietic stem cell transplantation (allo-SCT). We analyzed the pharmacokinetics (PK) of Tac QD in allo-SCT recipients. A total of 10 patients with hematological malignancies who received allo-SCT from unrelated donors were enrolled. Patients received Tac i.v. at 0.03 mg/kg a day before transplantation. Administration of Tac i.v. was converted to Tac QD at a 1:4 ratio when the patients had recovered from regimen-related gastrointestinal toxicity and could tolerate oral medication. After conversion, six out of 10 patients (60 %) showed a sustained decrease in Tac exposure and required dose adjustment. The conversion from Tac i.v. to Tac QD should be performed under close medical supervision. Area under the curve (AUC) and the trough of Tac QD showed a correlation, and the trough should be maintained above 7.5 ng/ml to provide an adequate AUC. Although four patients received bone marrow from an HLA DRB1 1 antigen-mismatched unrelated donor, no patients developed grade III–IV acute graft-versus-host disease (GVHD). The modification of Tac QD to maintain a whole-blood trough concentration above 7.5 ng/ml may be as effective as Tac BID.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In solid organ transplantation, lifelong immunosuppression is required to preserve graft function. Medication nonadherence is a major risk factor for graft failure. Oral tacrolimus (Tac) was first developed as a twice-daily formulation (Tac BID) and has been widely used in solid organ and allogeneic hematopoietic stem cell transplantation (allo-SCT), but long-term adherence remains a concern. It has been reported that morning dosing is associated with significantly higher adherence than evening dosing in kidney transplant patients [1]. In response to this potential adherence problem, a once-daily modified release formulation of oral tacrolimus (Tac QD) has been developed with a morning dosing regimen that maximizes the potential for adherence [2]. Tac QD possibly contributes to reduce physical and mental stress for patients who need to take several different medications. In de novo kidney, liver, and heart transplantation, phase II studies have demonstrated that patients can be converted from Tac BID to Tac QD on a one-to-one total daily-dose basis [3], and the efficacy and safety of Tac QD were maintained in long-term graft survival [4]. Randomized phase III studies have reported that Tac QD was well tolerated with similar efficacy and safety profiles to Tac BID in kidney and liver transplantation [5, 6]. However, several investigators have recently reported a sustained decrease in Tac exposure after conversion from Tac BID to Tac QD, and it is necessary to use a higher dose of Tac QD than Tac BID to achieve similar trough levels [7–10]. Therefore, the switch from Tac BID to Tac QD should be performed under close medical supervision.
In allo-SCT, prevention and treatment of graft-versus-host disease (GVHD) are critical factors in transplant-related morbidity and mortality. Tac plus methotrexate has been used as one of the standard regimens for GVHD prophylaxis after allo-SCT from unrelated donors [11, 12]. However, there have been no data available about the efficacy and safety of Tac QD conversion from intravenous Tac (Tac i.v.) in allo-SCT recipients. In this study, we analyzed the pharmacokinetics (PK) of Tac QD. The aim of this study was to evaluate the PK profile of Tac QD in allo-SCT patients. This is the first report of a PK study of Tac QD in patients who received allo-SCT from unrelated donors for the prevention of GVHD.
Methods
This is a prospective clinical trial involving investigation of the PK of Tac QD in allo-SCT patients. Patients who were 15–65 years of age were eligible to participate in this study. Patients were excluded if their serum creatinine was over 2 mg/dl, performance status by the ECOG criteria was over 2, and serology was positive for human immunodeficiency virus, or if they had uncontrolled infections. This study was approved by the Institutional Review Board at Jikei University and was registered at www.umin.ac.jp/ctr/ as UMIN000002441. Each patient provided written informed consent in accordance with the Declaration of Helsinki.
Study design
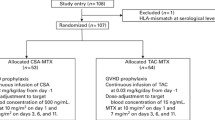
The patients were treated with various conditioning regimens (Table 1) and received unrelated bone marrow or umbilical cord blood transplantation. Micafungin was administered at a dose of 50 mg/day intravenously as antifungal prophylaxis until granulocyte counts exceeded 0.5 × 109/l. All patients received Tac i.v. at 0.03 mg/kg by continuous infusion beginning a day before transplantation with short-term methotrexate, 10 mg/m2 on day 1, and 7 mg/m2 on days 3, 6, and 11 in unrelated bone marrow, or 15 mg/m2 on day 1 and 10 mg/m2 on days 3 and 6 in umbilical cord blood. The dose of Tac i.v. was adjusted to maintain the whole-blood Tac concentration between 10 and 20 ng/ml. Administration of Tac i.v. was converted to Tac QD at a 1:4 ratio when the patients had recovered from regimen-related gastrointestinal toxicity and could tolerate oral medication. Tac QD exposure was adjusted to maintain a whole-blood trough concentration of 8–12 ng/ml. A dose reduction of Tac QD was recommended if serum creatinine increased more than 1.5 times from the baseline or if other serious toxicities associated with the agent appeared.
PK sampling and analysis
When the patients did not require a dose adjustment after conversion to Tac QD, blood samples were collected 0, 1, 2, 3, 6, 12, and 24 h after exposure. These blood samples were frozen at −20 °C within 2 h after collection and stored until shipment to the SRL laboratory in Tokyo, Japan, for analysis. The plasma concentration of Tac was determined by the ACMIA method. Area under the curve (AUC) was determined by the linear trapezoidal rule using a noncompartmental approach.
Statistical analysis
The primary endpoint of this study was analysis of the pharmacokinetic behavior of Tac QD. The secondary endpoints were to assess the development of grade II–IV acute GVHD after the conversion. Acute GVHD was evaluated according to the standard criteria [13]. Neutrophil engraftment was defined as the first of three consecutive days with an absolute neutrophil count of greater than 0.5 × 109/l. Adverse events were graded according to the Common Terminology Criteria for Adverse Events Version 4.0. Spearman’s rank correlation coefficient was calculated to assess the correlation between AUC and the trough of Tac QD. EZR was used for statistical analysis [14].
Results
Patient characteristics
This study included 10 consecutive patients with acute myeloid leukemia (AML) (n = 6), acute lymphoblastic leukemia (ALL) (n = 1), myelodysplastic syndrome (MDS) (n = 2), and non-Hodgkin lymphoma (NHL) (n = 1) who underwent allo-SCT from unrelated donors between October 2009 and May 2011. These patients’ characteristics are summarized in Table 1. Median age was 45 (23–65) years. Six patients were classified into a standard-risk group (first complete remission: CR1 = 3, CR2 = 3) and four patients into an advanced-risk group (non-CR = 3, refractory anemia with excess blast-1 = 1) at allo-SCT. Stem cell sources were bone marrow (BM) from an HLA-matched unrelated donor (n = 4), BM from an HLA DRB1 1 antigen-mismatched unrelated donor (n = 4), or umbilical cord blood (n = 2).
Tac trough concentration after conversion from Tac i.v. to Tac QD
All patients received Tac i.v. at 0.03 mg/kg by continuous infusion beginning a day before transplantation. When the patients had recovered from regimen-related gastrointestinal toxicity and could tolerate oral medication, we converted Tac i.v. to Tac QD at a 1:4 ratio. After conversion, six out of 10 patients (60 %) showed a sustained decrease in Tac exposure and required dose adjustment (Fig. 1). It took a median of 11 (2–33) days to reach stable Tac exposure after the conversion. According to the conditioning regimens, five out of seven patients (71 %) who received total body irradiation (TBI ≥ 10 Gy) or high-dose melphalan (≥80 mg/m2) needed an increase in the dose of Tac QD, whereas one out of three patients (33 %) treated with busulfan without TBI and melphalan required dose escalation.

The whole-blood trough of Tac tended to decrease after the conversion from Tac i.v. to Tac QD
PK analysis
In the PK analysis, the median C 0 was 9.8 ng/ml and C max was 19.5 ng/ml at a T max of 4.5 h post-dose (Fig. 2). The median area under the curve (AUC0–24) was 246 ng·h/ml. There was a correlation between AUC and the trough of Tac QD (Fig. 3, ρ = 0.8754, P = 0.0009). To obtain AUC0–24 of more than 240 ng·h/ml, it is necessary to maintain the whole-blood trough at more than 7.5 ng/ml.

Pharmacokinetic analysis of Tac QD

There was a correlation between AUC and trough of Tac QD
Development of acute GVHD and adverse effect of Tac QD
Engraftment was confirmed in all patients. One patient experienced a rapid decrease in the trough concentration of Tac from 9.8 to 3.6 ng/ml right after the conversion, and he developed grade II acute GVHD in the skin. No patients developed grade III–IV acute GVHD within the first 100 days after allo-SCT. The most common adverse event was grade 1–2 elevation of AST or ALT (10 patients), but all patients improved promptly without dose modification of Tac QD. Three patients developed nephrotoxicity (grade 1 in one patient, grade 2 in two patients), and one patient needed to reduce the dose of Tac because of a transient increase of serum creatinine up to 1.85 mg/dl. Within the first 100 days after allo-SCT, all patients were alive and disease free. The probability of overall survival at 3 years was 70 %. Three patients died because of relapse in two patients and cardiac failure in one patient.
Discussion
GVHD remains one of the main causes of treatment-related mortality after allo-SCT, so that prevention of GVHD is an important issue for the treatment to succeed. The combination of calcineurin inhibitor and short-term methotrexate has been one of the standard prophylaxis methods. Calcineurin inhibitors are usually started intravenously a day before transplantation, and the agents are converted to an oral formulation when patients can tolerate oral medication. Twice-daily formulation of oral calcineurin inhibitors has been widely used in allo-SCT and solid organ transplantation. As lifelong immunosuppression is required to prevent graft dysfunction in solid organ transplantation, medication nonadherence is a matter of utmost concern. Tac QD has been developed to improve compliance in kidney and liver transplantation, and it has been well tolerated with similar efficacy to Tac BID [5, 6]. Although patients who have undergone allo-SCT are supposed to take oral Tac for a shorter period than solid transplant recipients, once-daily Tac may reduce physical and mental stress for patients who need to take several different medications. However, there have been no data available about the efficacy and safety of Tac QD conversion from Tac i.v. in the setting of allo-SCT. We speculated that the use of Tac QD instead of Tac BID for GVHD prophylaxis exhibits an equivalent effect.
Recently, the necessity of using higher doses of Tac QD to achieve a therapeutic level compared with the Tac BID dose in a kidney transplant has been reported [7–10], despite initial reports showing the bioequivalence of Tac QD with Tac BID. These reports suggest that lower Tac exposure is observed after conversion from Tac BID to Tac QD because of decreased bioavailability. In this study, the patients were converted from Tac i.v. to Tac QD at a 1:4 ratio according to one of the standard approaches for the conversion from Tac i.v. to Tac BID [15, 16]. The 1:4 ratio resulted in a decrease of Tac exposure for six out of 10 patients (60 %) and required dose adjustment. According to the conditioning regimens, most of the patients who needed dose adjustment received TBI ≥10 Gy or high-dose melphalan. Mucosal injury of the intestine might reduce absorption of the agent. Importantly, one patient experienced a rapid decrease in the trough concentration of Tac right after the conversion and he developed grade II acute GVHD in the skin. Therefore, the conversion from Tac i.v. to Tac QD should be performed under close medical supervision. The patients who receive high-dose TBI or melphalan as a conditioning regimen in particular may have to increase the conversion ratio to more than 1:4. Mita et al. reported that the optimal initial dose ratio of Tac i.v. to Tac QD was 1:8 in the setting of liver transplantation [17].
PK analysis showed that there was a correlation between AUC and the trough of Tac QD (Fig. 3). We set a target AUC0–24 of Tac QD of more than 240 ng·h/ml because we had adjusted the dose of Tac i.v. by continuous infusion to maintain the whole-blood Tac concentration between 10 and 20 ng/ml, and preservation of Tac blood concentration 10 ng/ml for 24 h would obtain an AUC0–24 of 240 ng·h/ml. Patients required a whole-blood Tac QD trough of at least 7.5 ng/ml to achieve an AUC of more than 240 ng·h/ml (Fig. 3). Although four patients received bone marrow from an HLA DRB1 1 antigen-mismatched unrelated donor, no patients developed grade III–IV acute GVHD. Obtaining a Tac QD trough above 7.5 ng/ml may be a valid approach for the prevention of acute GVHD.
In this study, engraftment was confirmed in all patients, and no patients died within 100 days after transplantation. Grade 1–2 renal and hepatic toxicities were observed, but they were mild and transient. The increased frequency of nephrotoxicity found in previous studies might have resulted from the higher doses of Tac or the higher ranges of blood concentration [18, 19]. One patient developed transient congestive heart failure on day 6 after allo-SCT. The symptom of heart failure immediately resolved after the treatment, and left ventricular ejection fraction recovered from 41 to 54 %, as measured by echocardiography. This patient could be discharged with no complications on day 55; however, he died of cardiac failure on day 220. Autopsy confirmed dilated cardiomyopathy. Although there have been several reports about Tac-associated reversible myocardial hypertrophy [20–22], only a few case reports of Tac-related dilated cardiomyopathy have been publicized in the setting of allo-SCT. However, we could not completely rule out an effect of Tac on this cardiac complication.
In conclusion, despite initial reports showing the bioequivalence of Tac QD with Tac BID, we found that 60 % of patients experienced a sustained decrease in Tac exposure. The conversion from Tac i.v. to Tac QD should be performed under close medical supervision. AUC and the trough of Tac QD showed a correlation in allo-SCT recipients. The whole-blood trough should be maintained around at least 7.5 ng/ml to provide an adequate level of AUC. The modification of Tac QD to maintain a whole-blood trough concentration above 7.5 ng/ml may be as effective as Tac BID.
References
Ichimaru N, Kakuta Y, Abe T et al (2008) Treatment adherence in renal transplant recipients: a questionnaire survey on immunosuppressants. Transplant Proc 40:1362–1365
First MR (2008) First clinical experience with the new once-daily formulation of tacrolimus. Ther Drug Monit 30:159–166
Comuzzi C, Lorenzin D, Rossetto A et al (2010) Safety of conversion from twice-daily tacrolimus (Prograf) to once-daily prolonged-release tacrolimus (Advagraf) in stable liver transplant recipients. Transplant Proc 42:1320–1321
van Hooff JP, Alloway RR, Trunečka P, Mourad M (2011) Four-year experience with tacrolimus once-daily prolonged release in patients from phase II conversion and de novo kidney, liver, and heart studies. Clin Transplant 25:E1–E12
Krämer BK, Charpentier B, Bäckman L et al (2010) Tacrolimus once daily (ADVAGRAF) versus twice daily (PROGRAF) in de novo renal transplantation: a randomized phase III study. Am J Transplant 10:2632–2643
Trunečka P, Boillot O, Seehofer D et al (2010) Once-daily prolonged-release tacrolimus (ADVAGRAF) versus twice-daily tacrolimus (PROGRAF) in liver transplantation. Am J Transplant 10:2313–2323
Crespo M, Mir M, Marin M et al (2009) De novo kidney transplant recipients need higher doses of Advagraf compared with Prograf to get therapeutic levels. Transplant Proc 41:2115–2117
Hougardy JM, Broeders N, Kianda M et al (2011) Conversion from Prograf to Advagraf among kidney transplant recipients results in sustained decrease in tacrolimus exposure. Transplantation 91:566–569
Jelassi ML, Lefeuvre S, Karras A, Moulonguet L, Billaud EM (2011) Therapeutic drug monitoring in de novo kidney transplant receiving the modified-release once-daily tacrolimus. Transplant Proc 43:491–494
Wu MJ, Cheng CY, Chen CH et al (2011) Lower variability of tacrolimus trough concentration after conversion from prograf to advagraf in stable kidney transplant recipients. Transplantation 92:648–652
Yanada M, Emi N, Naoe T et al (2004) Tacrolimus instead of cyclosporine used for prophylaxis against graft-versus-host disease improves outcome after hematopoietic stem cell transplantation from unrelated donors, but not from HLA-identical sibling donors: a nationwide survey conducted in Japan. Bone Marrow Transplant 34:331–337
Perkins J, Field T, Kim J et al (2010) A randomized phase II trial comparing tacrolimus and mycophenolate mofetil to tacrolimus and methotrexate for acute graft-versus-host disease prophylaxis. Biol Blood Marrow Transplant 16:937–947
Przepiorka D, Weisdorf D, Martin P et al (1995) 1994 consensus conference on acute GVHD grading. Bone Marrow Transplant 15:825–828
Kanda Y (2013) Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant 48:452–458
Osunkwo I, Bessmertny O, Harrison L et al (2004) A pilot study of tacrolimus and mycophenolate mofetil graft-versus-host disease prophylaxis in childhood and adolescent allogeneic stem cell transplant recipients. Biol Blood Marrow Transplant 10:246–258
Mehta P, Beltz S, Kedar A, Graham-Pole J, Wingard JR (1999) Increased clearance of tacrolimus in children: need for higher doses and earlier initiation prior to bone marrow transplantation. Bone Marrow Transplant 24:1323–1327
Mita A, Ikegami T, Masuda Y et al (2014) Optimal initial dose of orally administered once-daily extended-release tacrolimus following intravenous tacrolimus therapy after liver transplantation. Transplant Proc 46:794–796
The U.S. Multicenter FK506 Liver Study Group (1994) A comparison of tacrolimus (FK 506) and cyclosporine for immunosuppression in liver transplantation. N Engl J Med 331:1110–1115
Ratanatharathorn V, Nash RA, Przepiorka D et al (1998) Phase III study comparing methotrexate and tacrolimus (prograf, FK506) with methotrexate and cyclosporine for graft-versus-host disease prophylaxis after HLA-identical sibling bone marrow transplantation. Blood 92:2303–2314
Atkison P, Joubert G, Barron A et al (1995) Hypertrophic cardiomyopathy associated with tacrolimus in paediatric transplant patients. Lancet 345:894–896
Nakata Y, Yoshibayashi M, Yonemura T et al (2000) Tacrolimus and myocardial hypertrophy. Transplantation 69:1960–1962
Mano A, Nakatani T, Yahata Y et al (2009) Reversible myocardial hypertrophy induced by tacrolimus in a pediatric heart transplant recipient: case report. Transplant Proc 41:3831–3834
Acknowledgments
This work was supported by Health and Labour Sciences Research Grants for Clinical Cancer Research from the Ministry of Health, Labour and Welfare, Japan. We thank the nursing staff who cared for the patients at Jikei University Hospital and SRL laboratory staff who analyzed the plasma concentration of Tac.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Yano, S., Mori, S., Saito, T. et al. Pharmacokinetics for once-daily modified release formulation of tacrolimus hydrate in unrelated hematopoietic stem cell transplantation. Ann Hematol 94, 491–496 (2015). https://doi.org/10.1007/s00277-014-2233-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00277-014-2233-7