
Abstract
Purpose
The aim of this study is to report rare anatomical variations of the cephalic vein (CV) in a 77-year-old Korean male cadaver.
Case report
On the right upper arm, the CV located lateral to the deltopectoral groove passed anterior to the clavicle at the lateral one-fourth of the clavicle without anastomosis to the axillary vein. It was connected to the transverse cervical and suprascapular veins by two communicating branches in the middle of its course at the neck, and opened into the external jugular vein at its junction with the internal jugular veins. The suprascapular and anterior jugular veins were flowed into the subclavian vein at the jugulo-subclavian venous confluence, and were connected by a short communicating branch.
Conclusion
Detailed knowledge of the variations in the CV is expected to be helpful in decreasing unpredicted injuries and possible postoperative complications when invasive venous access is performed through the CV.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The cephalic vein (CV) and basilic vein are the superficial veins that drain the blood of the hand and subcutaneous tissue of the upper limb [9]. The CV originates from the posterior part of the radial styloid process, curves around the lateral side of forearm, and ascends along the lateral aspect of the lower and upper arms. It passes the gap between the pectoralis major and deltoid muscles (deltopectoral groove), and finally drains into the axillary vein and pierces the clavipectoral fascia just below the clavicle [14]. In invasive procedures, such as central venous access and the transvenous lead placement of a pacemaker [12, 15], the CV has been considered as an alternative approach, while the subclavian or axillary veins can also be successful in most cases [11] due to their consistent anatomical characteristics [17], sufficient size for easy cannulation [7, 18], and a lower incidence rate of injury to adjacent structures [7]. The morphological structure and anatomical variations of the CV could therefore be of considerable interest to physicians who perform venous access and lead introduction via the CV to avoid inadvertent injury.
Many studies have found anatomical variations in the number, course, and termination of the CV [1,2,3,4,5,6, 8, 13, 16]. We encountered a rare case during routine dissection where the CV crossed superficial to the lateral one fourth of the clavicle, connected to the transverse cervical and suprascapular veins via additional communicating branches, and entered into the external jugular vein at its junction with the internal jugular vein.
Case report
During routine dissection for educational purposes at Kangwon National University School of Medicine, a rare anatomical presentation of a right supraclavicular CV communicating with the transverse cervical and suprascapular veins was found in a 77-year-old Korean male cadaver, whose cause of death was hepatocellular carcinoma. This study was approved by the institutional review board of our university for anatomy research.
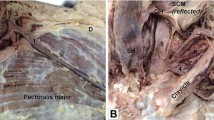
The CV did not ascend along the deltopectoral groove but instead was identified on the deltoid muscle. It was located 5.9 mm, 9.6 mm, and 6.2 mm lateral to the inferior, middle, and superior parts of the lateral border of the deltopectoral triangle, respectively (Fig. 1A). The CV passed anterior to the clavicle at the lateral one-fourth of the clavicle without anastomosis to the axillary vein, and ascended to the neck region. Further dissection to reflect the platysma and sternocleidomastoid muscles was needed to trace its entire path. After passing over the anterior surface of the clavicle, the CV was connected with the transverse cervical and suprascapular veins by two communicating branches in the middle of its course at the neck, and finally flowed into the external jugular vein at its junction with the internal jugular veins (Fig. 1B). The transverse cervical vein normally drained into the external jugular vein, and the suprascapular vein opened into the subclavian vein at the jugulo-subclavian venous confluence. The anterior jugular vein entered into the subclavian vein, and was connected with the suprascapular vein via a short communicating branch.

Supraclavicular cephalic vein observed before (a) and after laterally (b) reflecting the sternocleidomastoid muscle in the same specimen. a Arrowheads indicate the deltopectoral groove between the deltoid and pectoralis major muscles. The CV runs lateral to the groove, ascends superficial to the clavicle, and joins to the EJV. b Arrows indicate the communicating branches connecting the CV to the TCV and SSV. The EJV drains into the IJV posterior to the intermediate tendon of the OM. CV cephalic vein, EJV external jugular vein, IJV internal jugular vein, SCV subclavian vein, TCV transverse cervical vein, PEJV posterior external jugular vein, SSV suprascapular vein, AJV anterior jugular vein, CCA common carotid artery, SCM sternocleidomastoid muscle, OM omohyoid muscle
Discussion
In anatomical textbooks, the CV follows the deltopectoral groove, and penetrates the clavipectoral fascia within the deltopectoral triangle [9, 14], but its morphological characteristics have been variously described regarding its number, course, and termination, such as being absent or very thin [6], dividing into two branches [1], or having a collateral branch connecting to the external jugular vein [7]. Other descriptions include the CV was not being located in the deltopectoral groove and perforating the pectoralis major [4], running between the clavicle and the subclavius muscle [16], or ascending superficial [3, 5, 7] or deep [13] to the clavicle. The termination of the CV has been sporadically detected in the basilic [17], subclavian [3, 7], external jugular [2, 5], and internal jugular [8, 13] veins. In the present case, the CV ascended superficial to the clavicle without any connection to the axillary vein and drained into the external jugular vein, which was similar to the findings of previous studies [2, 5]. However, the location of the CV was identified lateral to the deltopectoral groove and triangle, and was connected to the transverse cervical and suprascapular veins by additional communicating branches in the middle of its course, and flowed into the external jugular vein at its junction with the internal jugular vein. The suprascapular and anterior jugular veins also drained into the subclavian rather than the external jugular vein, and their terminal parts were connected to each other by another communicating branch. These combinations of anatomical variations have not been found in any previous study that we were aware of.
The anomalous venous patterns, in this case, could be explained on an embryological basis by the regression and retention of the anastomotic vasculature. According to Padget [10], during a normal development, the proximal end of the primitive cephalic vein appeared from the preaxial vein develops into the jugulocephalic vein (JCV) via anterosuperior anastomosing with the primitive subclavian vein and then posteroinferiorly anastomosed to form a cephalic venous ring surrounding the clavicle. Thereafter, the anterosuperior vascular anastomosis of the cephalic venous ring gradually degenerates, while the posteroinferior one is retained, where the external jugular vein and primary head vein join. The primitive cephalic, primitive subclavian, and primary head veins connected to the cephalic venous ring develop into the cephalic, subclavian, and internal jugular veins, respectively [5, 10]. In the present case, the CV may fail to lose connection with the external jugular vein (persistent JCV) as in a previous report [5]. However, the external jugular vein receiving the CV unusually connected to the middle of the internal jugular vein, and the internal jugular vein flowed into the subclavian vein. To the best of our knowledge, these anatomic variations have not been reported in the previous literatures. This might be due to the elongation of the neck without the complete separation of primitive cephalic, primitive subclavian, and primary head veins from the cephalic venous ring.
The findings of this study may have clinical implications for physicians who expect to observe the normal termination of the CV in the axillary vein. A guide wire or lead introduced via the CV may ascend anterior at the lateral one fourth of the clavicle, and indirectly enter into the internal jugular vein at its junction with the external jugular vein, forming a highly arched course at the middle of the neck. The communicating branches connecting the CV to the transverse cervical and suprascapular veins could cause accessory pathways that directly lead an introduced line or catheter in the wrong direction, and practitioners may encounter unpredicted puncturing at the axillary or supraclavicular structures during clinical procedures. Knowledge of these anatomical variations could be expected to be helpful for reducing the risk of unpredicted injuries and postoperative complications when clinicians perform venous access via the CV.
Conclusion
The case in this study differed somewhat from other that have been reported in the literatures: the supraclavicular-coursed CV connected to the transverse cervical and suprascapular veins by communicating branches, and indirectly drained into the body of the internal jugular vein through its junction with the external jugular vein. Because the possibility of the using the CV for invasive venous access is determined by the morphoanatomical parameters, knowledge of its anatomical variations can be of considerable interest to clinicians.
Availability of data and materials
Not applicable.
References
Charpy A (1903) Veines in Particulier. In: Poirier P, Charpy A (eds) Traite ́d’Anatomie Humaine. Masson et Cie Editeurs, Paris (cited by Vazquez and Sanudo 2016).
Deslaugiers B, Vaysse P, Combes JM, Guitard J, Moscovici J, Visentin M, Vardon D, Bécue J (1994) Contribution to the study of the tributaries and the termination of the external jugular vein. Surg Radiol Anat 16:173–177. https://doi.org/10.1007/BF01627591
Go JY, Han DJ, Kim J, Yoon SP (2017) A supraclavicular cephalic vein drained into the subclavian vein. Surg Radiol Anat 39:1413–1415. https://doi.org/10.1007/s00276-017-1878-z
Hong JE, Kim BR, Kim J, Yoon SP (2016) A cephalic veindrained into one of the double axillary veins through the pectoralis major muscle. Folia Morphol (Warsz) 75:268–270. https://doi.org/10.5603/FM.a2015.0082
Kameda S, Tanaka O, Terayama H, Kanazawa T, Sakamoto R, Tetsu S, Sakabe K (2018) Variations of the cephalic vein anterior to the clavicle in humans. Folia Morphol (Warsz) 77:677–682. https://doi.org/10.5603/FM.a2018.0018
Le Saout J, Vallee B, Person H, Doutriaux M, Blanc J, Nguyen H (1983) Anatomical basis for the surgical use of the cephalic vein (V. Cephalica). 74 anatomical dissections. 189 surgical dissections. J Chir (Paris) 120:131–134
Loukas M, Myers CS, Wartmann ChT, Tubbs RS, Judge T, Curry B, Jordan R (2008) The clinical anatomy of the cephalic vein in the deltopectoral triangle. Folia Morphol (Warsz) 67:72–77
Lum C, Ladenheim ED (2013) An interesting clinical case: variant of the cephalic vein emptying into the internal jugular vein. Semin Dial 26:E11–E12. https://doi.org/10.1111/j.1525-139X.2012.01102.x
McMinn RMH (1990) Last’s anatomy, regional and applied, 8th edn. Churchill Livingstone, Edinburgh, p 94
Padget DH (1956) The cranial venous system in man in reference to development, adult configuration, and relation to the arteries. Am J Anat 98:307–355. https://doi.org/10.1002/aja.1000980302
Parsonnet V, Roelke M (1999) The cephalic vein cutdown versus subclavian puncture for pacemaker/ICD lead implantation. Pacing Clin Electrophysiol 22:695–697. https://doi.org/10.1111/j.1540-8159.1999.tb00531.x
Povoski SP (2000) A prospective analysis of the cephalic vein cutdown approach for chronic indwelling central venous access in 100 consecutive cancer patients. Ann Surg Oncol 7:496–502. https://doi.org/10.1007/s10434-000-0496-9
Saaid A, Drysdale I (2008) Unusual termination of the cephalic vein. Clin Anat 21:786–787. https://doi.org/10.1002/ca.20661
Standring S (2015) Gray’s anatomy: the anatomical basis of clinical practice, 41st edn. Elsevier, Philadelphia, pp 619–620
Świętoń EB, Steckiewicz R, Grabowski M, Stolarz P (2016) Selected clinical challenges of a supraclavicular cephalic vein in cardiac implantable electronic device implantation. Folia Morphol (Warsz) 75:376–381. https://doi.org/10.5603/FM.a2015.0125
Testut L (2016) Latarjet A (1929) Traite ́d’anatomie humanine, 8th edn. Gaston Doin & Cie Editeurs, Paris (cited by Vazquezand Sanudo
Vazquez T, Sanudo J (2016) Veins of the upper limb. In: Tubbs S, Shoja MM, Loukas M (eds) Bergman’s comprehensive encyclopedia of human anatomic variation. Willey Blackwell, New Jersey, pp 826–831
Vialle R, Pietin-Vialle C, Cronier P, Brillu C, Villapadierna F, Mercier P (2001) Anatomic relations between the cephalic vein and the sensory branches of the radial nerve: how can nerve lesions during vein puncture be prevented? Anesth Analg 93:1058–1061. https://doi.org/10.1097/00000539-200110000-00052
Acknowledgements
The authors express their gratitude to the body donor and the families who participated in the body donation program of the Kangwon National University School of Medicine. Results from such research can potentially increase mankind’s overall knowledge that can then improve patient care. The authors thank Kyung-Jin Lee and Soon-Jung Kim for their technical supports.
Funding
This study was supported by the Soonchunhyang University Research Fund (No. 20220446).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Writing and revision of the anatomic part of manuscript by HSW. Writing and revision of the embryologic part of manuscript by JOS and SMN. Project development, data collection, writing—original draft, and editing by HJW. HSW and JOS are co-first authors and contributed equally to this work.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare. Finally, no benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject matter of the manuscript.
Ethical approval
Approval was obtained from the institutional review board of the Kangwon National University for anatomy research (approval number KWNUIRB-2022–10-005).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Won, HS., Shin, JO., Nam, S.M. et al. Supraclavicular cephalic vein draining into the internal jugular vein via the external jugular vein. Surg Radiol Anat 45, 487–490 (2023). https://doi.org/10.1007/s00276-023-03109-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-023-03109-8