
Abstract
Purpose
In the present study, we aimed to determine the relationship of HV angle with angles and measurements obtained from lateral and anteroposterior (AP) radiological images of the foot in individuals with HV.
Methods
The present study had a retrospective design, and the participants consisted of 66 female patients between the ages of 19 and 64 who applied to Orthopedics and Traumatology and were diagnosed with Hallux valgus. Metatarsus adductus angle, metatarsus primus adductus angle, hallux valgus angle, hallux interphalangeal angle, metatarsal break angle, first metatarsal protrusion distance, metatarsal width, talocalcaneal angle, AP Meary’s angle were measured on AP view and calcaneal inclination angle, talar declination angle, lateral talocalcaneal angle, first metatarsal declination angle, fifth metatarsal declination angle, navicular height, lateral Meary’s angle, tibiotalar angle were measured on a lateral radiograph. The IBM SPSS 21.0. program was used for statistical analysis, and the level of significance was taken as p < 0.05.
Results
There were statistically significant differences between the right and left feet in MPA and AMA measurements. The results showed that HV angle (HVA) had a weak relationship with MAA and MW, as well as a moderately positive relationship with MPA. However, it had a moderately negative relationship with AMA and a weak negative relationship with HIPA.
Conclusion
We believe that in addition to the HVA angle, MPA and AMA angles should be considered in the diagnosis of HV, especially as the HVA angle is moderately positively correlated with the MPA angle and moderately negatively correlated with the AMA angle.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hallux valgus (HV) is a very common foot deformity that affects the anterior side of the foot and it presents with a gradual subluxation of the first metatarsophalangeal joint caused by lateral deviation of the hallux and medial deviation of the first metatarsal bone. This deformity typically results in the development of soft tissue and bony protrusion in the medial of the first metatarsal head [9].
HV is a complex condition characterized by a series of deformities of variable severity, suggesting that several factors may be involved in its formation. The role of heredity and sex in the occurrence of this deformity is significant. However, other anatomical and biomechanical factors, such as variations in the metatarsal bones, particularly the first metatarsal bone, round articular face, bunion, medial prominence, degenerative osteoarthrosis and metatarsus primus varus deformation, are also critical. These variations may render them more prone to hypermobility of the first row, flat feet, and loosening of the ligaments [5, 23, 25]. This pathology is also associated with bone deviation from axes and the deterioration of muscle stabilization around this joint. The first metatarsal, in particular, deviates medially, and the hallux rotates and deviates to some extent laterally in the two main segments of the joint. As a result, the medial capsular ligament is torn and weakened, and the sesamoid bones and metatarsal head are moved away from the normal plantar joints [5, 10, 11].
The incidence of HV is higher in women. Although the rate is 2:1 in infants, it increases drastically to 15:1 in adults. These findings indicate that the prevalence of this deformity in women, especially at older ages, is attributable to the use of narrow and high-heeled shoes that may induce it [5, 20, 23, 30].
As a deformity, HV is clearly visible and can be easily diagnosed in the clinic with a simple examination. Although there are still studies in the literature conducted on the reliability and validity of X-ray measurements, these measurements are still considered the gold standard in the preoperative evaluation of deformities. In the radiological evaluation of the patient, 15° is generally accepted as the upper limit of the normal range for the hallux valgus angle (HVA) [3, 9, 10, 14]. Sex, genetic factors, shoe selection, body mass index, first metatarsal shape and length, pes planus, race, and ligamentous laxity have all been associated with HV in previous studies. This deformity is considered that it is diagnosed at a higher rate in women than in men as they prefer narrow and high-heeled shoes, especially at older ages [4, 7, 11, 22, 23].
Despite this high prevalence and its impact on quality of life, only a small number of studies have been performed on women. In the present study, we aimed to determine the relationship of HV angle with angles and measurements obtained from lateral and anteroposterior (AP) radiological images of the foot in individuals with HV.
Materials and methods
The present study had a retrospective design. The study included 66 women (age, 19–64 years) diagnosed with HV who had sought treatment from the Orthopedics and Traumatology Department of Cukurova University Balcali Hospital Health Practice and Research Center between 2008 and 2020. The patient images were retrieved from the archive system. In this study, we evaluated the radiographic images of a total of 114 feet of 66 people who were admitted to the Orthopedics and Traumatology Department, with HV on physical and radiological examinations and were indicated for surgery. In our study, 48 of 66 participants were diagnosed with HV in both feet, whereas 18 patients were diagnosed with HV in only one foot. Radiographic images of these feet were available. The inclusion criteria were a minimum age of 18 years, closed epiphysis, and a positive HV diagnosis. The patients with a history of surgical operation on the foot and ankle region, fractures, trauma, congenital anomalies, and inadequate radiographs were excluded from the study. The study obtained the approval of the Ethics Committee with the number 11.06.2021/112 from the Cukurova University Faculty of Medicine Non-Invasive Clinical Research Ethics Committee. The radiographic measurements were performed on 114 feet of 66 participants (48 bilateral, 18 unilateral) on standard weight-bearing AP and lateral images. A total of 17 angle and distance measurements were recorded, 9 on the AP and 8 on the lateral radiographic images. The images were viewed using the Enlil PACS system software (Eskisehir, Turkey). The required measurements were performed using PACS measurement tools. Tables 1 and 2 show detailed descriptions of the angle and distance measurements, and Figs. 1 and 2 show some of the measured angle and distance values. The angle values in the opposite direction of the normal angle values were evaluated as negative and used as an example in the measurements, as presented in Fig. 3 on the hallux interphalangeal angle (HIPA) angle measurement.

a Measurements in anteroposterior view of the weight-bearing foot; MAA Metatarsus adductus angle, HIPA Hallux interphalangeal angle, MBA Metatarsal break (parabola) angle, MW Metatarsal width. b Measurements in anteroposterior view of the weight-bearing foot; MPA Metatarsus primus adductus angle, HVA Hallux valgus angle, HIPA Kite angle: Talocalcaneal angle, AMA AP Meary’s angle

a Measurements in lateral view of the weight-bearing foot; CIA Calcaneal inclination angle, TDA Talar declination angle, 1MDA First metatarsal declination angle, LMA Lateral Meary’s angle. b Measurements in lateral view of the weight-bearing foot; TCA Lateral talocalcaneal angle, 5MDA Fifth metatarsal declination angle, NHT Navicular height, TTA Tibiotalar angle

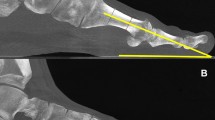
The image of positive (A) and negative (B) measurement values of HIPA angle measurement in AP foot radiographs
All angles and distances were measured twice, independently by two authors (A.K.A., F.B.). Intraclass correlation coefficients (ICC with 95% confidence intervals) were used for reliability testing. When the intra-observer reliability was examined in all measurements, the ICC value was 0.94–0.98 in both observers, while it was 0.92–0.96 in the interobserver reliability. All measurements had excellent intra- and interobserver reliability [16].
Statistical analysis
The conformity of the variables to the normal distribution was assessed using a Shapiro–Wilk test and graphics. The mean, standard deviation, median, and range (minimum–maximum) of the measurements were calculated using descriptive analysis. The Paired Samples t test was performed for the right and left foot comparison of the normally distributed data. The relationship between quantitative variables was assessed using the correlation analysis, and the level of the relationship was determined using the Pearson Correlation Coefficient. The statistical analysis was performed using the IBM SPSS (version 21; SPSS, Armonk, NY, USA) software, with a significance level of p < 0.05.
Results
In our study, we evaluated AP and lateral radiographs of the feet from 66 patients with HV (mean age 44.35 ± 13.12 years; range 19–64 years). Table 3 shows the descriptive statistics of the radiological angle and distance measurements obtained from 114 AP and lateral foot images of 66 patients included in the study.
The differences between the radiographic measurements of the right and left feet of 48 patients (96 feet) with HV, who had radiographic images of both feet, were examined (Table 4). Although the MPA (p = 0.022) and AMA (p = 0.021) measurements showed significant differences between the right and left feet, there were no significant differences in other measurements.
The correlation between age and all measurements obtained from the AP and lateral foot images, as well as the metatarsus primus adductus angle (MPA), hallux valgus angle (HVA), hallux interphalangeal angle (HIPA), metatarsal break (parabola) angle (MBA), first metatarsal protrusion distance (MPD), metatarsal width (MW), and AP Meary's angle (AMA) measurements associated with the hallux, were also investigated (Table 5). The significant correlation coefficients between our measurement outcomes were − 0.188–0.658. The results showed that HV angle (HVA) had a weak relationship with MAA (r = 0.213, p = 0.023) and MW (r = 0.199, p = 0.034), as well as a moderately positive relationship with MPA (r = 0.480, p < 0.001). However, it had a moderately negative relationship with AMA (r = − 0.333, p < 0.001) and a weak negative relationship with HIPA (r = − 0.281, p = 0.002) [6].
Discussion
In surgical planning, the reference lines, angles, and measurements in radiological images play a significant role. These provide the foundation for the precise evaluation of foot and ankle deformities in orthopedics, physical therapy, rehabilitation, and surgical sciences in general. HV deformity is among the most common musculoskeletal disorders in the foot and ankle impacting foot comfort. It is most commonly associated with a medial deviation of the first metatarsal bone, deformity of the phalangeal bone and interphalangeal joint, and pronation with sesamoid subluxation [13]. Sex, heredity, and osteoarthritis all influence the prevalence of HV [24]. According to the literature, its prevalence is higher in women than in men [21]. The reason for this may be attributable to the shoe preferences in women, which are influenced by sociocultural structure and lifestyles [24]. Although previous studies have often evaluated various radiographic measurement data of patients with HV, very few studies have assessed comprehensive radiographic measurement covering the patient’s entire foot and explored the relationship of these measurement data with HV, as we performed in the present study. Hence, we believe that the present study is significant as it evaluated the measurement data that may be useful in HV diagnosis.
Steinberg et al. investigated the relationship between lower extremity alignment and HV in women, claiming that it developed because of a chain reaction that started in the hip joint [27]. Cavalheiro et al. studied the relationship between HV and anatomical changes and radiographic findings on 22-foot radiographs of cadavers with HV. They determined that the hallux valgus angle (HVA) was 18.6° and the intermetatarsal angle (MPA) was 27.3° and hypothesized that anatomical changes in HV might depend on the degree of radiographic deformity [5].
Adult acquired flat foot (pes planus) is a condition that occurs or persists after the attainment of skeletal maturity and is characterized by the loss of height in the medial longitudinal arch and Some studies suggested the presence of a significant relationship between HV deformity and pes planus [1, 8, 15, 19, 25, 28]. Komeda et al. showed a significant relationship between HV deformity and pes planus [15]. These values were higher in the present study. Investigating the relation between HV and pes planus, Atbaşı et al. indicated that the mean values of HVA, MPA, Lateral Meary's angle (LMA), calcaneal inclination angle (CIA), and lateral talocalcaneal angle (TCA) angles in the AP and lateral radiographic images of the case group consisting of 56 participants with HV were 23.1°, 9.7°, 3.3°, 11.9°, and 32.8°, respectively. Their results also showed the presence of a high correlation between pes planus and HV [1]. However, the relationship between pes planus and HV remains controversial in the literature. In a study performed on men by Coughlin and Shurnas, no correlations were reported between HV and pes planus [8]. Saragas and Becker indicated that there were no differences in the incidence of pes planus between the HV and the control group in 110 African women with HV and healthy women [25]. However, Suh et al., investigated the relationship between HV and pes planus in 142 adult patients and concluded that there was no significant relationship between the two [28]. In our study, there was a significant and positive correlation between HVA and MAA, MPA, and MW measurements, as well as a negative correlation between AMA and HIPA measurements (p < 0.05). Furthermore, there was no significant correlation between age, HVA, HIPA, MPA, and MW measurements and foot lateral radiographic measurements. There were no significant relationships between HV deformity and pes planus angles in our study.
There are numerous studies in the literature that provide average values for different angle and length measurements of the feet of individuals with HV deformity. These studies compare the foot angle and length measurements of HV and healthy individuals on foot radiographic images and examine the relationship between HV and different foot pathologies. Preoperative radiography results in 516 patients with HV deformity were analyzed by Götze et al., who indicated that the mean HVA value was 34.5 and MPA 15.5° [12]. However, Lee et al. used radiographic images of 732 patients with HV to compute the mean of HVA, MPA, HIPA, MAA, and MPD measurements, which were 23°, 12°, 11°, 25°, and 2 mm respectively [18]. In a patient group of 30 participants, Bryant et al. compared the foot radiographic images of control, HV, and hallux limitus. Although no significant differences in lateral radiographic measurements were found across study groups, they did find significant differences between the groups in MPA, HVA, HIPA, MPD, and MW measurements obtained from AP radiographic images [2]. In our study, the mean values of MAA, MPA, HVA, HIPA, MBA, MPD, Kite angle, AMA, and MW measurements in AP radiographic foot images were 12.81°, 13.56°, 30.63°, 9.03°, 145.18°, 0.49 mm, 25.23°, − 1.01°, and 85.74 mm. On lateral radiographic images, the mean of CIA, TDA, TCA, 1MDA, 5MDA, NHT, LMA, and TTA measurements were 22.22°, 26.76°, 48.40°, 25.80°, 12.42°, 39.83 mm, 0.91°, and 65.85°, respectively. A comparison could not be established since the study used the mean values of the total population and the Study Group consisted of only women. The low number of male patients diagnosed with HV in our hospital archive, the lower number of female patients than predicted, and the small number of unilateral feet with an HV deformity in one foot but no deformity in the other (n = 18) were all limitations of our study. Moreover, multi-center studies with a larger sample size and a larger geographical area can be planned in future research.
Conclusion
Based on the results, we determined that the HV angle (HVA) is related to MAA, MPA, AMA, HIPA angles, and MW measurement. We believe that in addition to the HVA angle, MPA and AMA angles should be considered in the diagnosis of HV, especially as the HVA angle is moderately positively correlated with MPA angle and moderately negatively correlated with the AMA angle.
Availability of data and material
All data can be shared transparently if there will be request.
Code availability
Not applicable.
References
Atbaşı Z, Erdem Y, Kose O, Demiralp B, Ilkbahar S, Tekin HO (2020) Relationship between hallux valgus and pes planus: real or fiction? J Foot Ankle Surg 59(3):513–517. https://doi.org/10.1053/j.jfas.2019.09.037
Bryant A, Tinley P, Singer K (2000) A comparison of radiographic measurements in normal, hallux valgus, and hallux limitus feet. J Foot Ankle Surg 39(1):39–43. https://doi.org/10.1016/S1067-2516(00)80062-9
Canella C (2020). Imaging evaluation of hallux valgus. Radiol Bras 53, VII–VII. https://doi.org/10.1590/0100-3984.2020.53.3e2
Carl A, Ross S, Evanski P, Waugh T (1988) Hypermobility in hallux valgus. Foot Ankle 8(5):264–270. https://doi.org/10.1177/107110078800800507
Cavalheiro CS, Arcuri MH, Guil VR, Gali JC (2020) Hallux valgus anatomical alterations and its correlation with the radiographic findings. Acta Ortop Bras 28(1):12–15. https://doi.org/10.1590/1413-785220202801226897
Chan YH (2003) Biostatistics 104: correlational analysis. Singapore Med J 44(12):614–619
Coughlin MJ, Jones CP (2007) Hallux valgus: demographics, etiology, and radiographic assessment. Foot Ankle Int 28(7):759–777. https://doi.org/10.3113/2FFAI.2007.0759
Coughlin MJ, Shurnas PS (2003) Hallux valgus in men part II: first ray mobility after bunionectomy and factors associated with hallux valgus deformity. Foot Ankle Int 24(1):73–78. https://doi.org/10.1177/2F107110070302400112
D'arcangelo PR, Landorf KB, Munteanu SE, Zammit GV, Menz HB (2010) Radiographic correlates of hallux valgus severity in older people. J Foot Ankle Res 3(1): 1–9. http://www.jfootankleres.com/content/3/1/20
Doğan A, Üzümcügil O, Akman YE (2007) Halluks valgus. TOTBİD Dergisi 2:88–94
Dykyj D (1989) Pathologic anatomy of hallux abducto valgus. Clin Podiatr Med Surg 6(1):1–15
Götze M, Hasmann SE, Hofmann UK, Walter C, Mittag F (2019) Preoperative analysis of radiographic findings in 516 patients with hallux valgus deformity. Acta Ortop Bras 27:16–19. https://doi.org/10.1590/1413-785220192701174203
Hujazi I, Yassa R, Sevenoaks H, Khalfaoui M, Barrie J (2019) Hallux valgus interphalangeus: reliability of radiological assessment. Foot Ankle Surg 25(4):507–510. https://doi.org/10.1016/j.fas.2018.03.005
Hummel J, Skweres J, Heineman N, Dessouky R, Xi Y, Zhang L, Wukich DK, Chhabra A (2019) Hallux valgus assessment on X-ray and Magnetic resonance Imaging (MRI): correlation with qualitative soft tissue and internal derangement findings on MRI. Eur J Radiol 113:24–31. https://doi.org/10.1016/j.ejrad.2019.01.035
Komeda T, Tanaka Y, Takakura Y, Fujii T, Samoto N, Tamai S (2001) Evaluation of the longitudinal arch of the foot with hallux valgus using a newly developed two-dimensional coordinate system. J Orthop Sci 6(2):110–118. https://doi.org/10.1007/s007760100056
Koo TK, Li MY (2016) A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med 15(2):155–163. https://doi.org/10.1016/j.jcm.2016.02.012
Lamm BM, Stasko PA, Gesheff MG, Bhave A (2016) Normal foot and ankle radiographic angles, measurements, and reference points. J Foot Ankle Surg 55(5):991–998. https://doi.org/10.1053/j.jfas.2016.05.005
Lee KM, Ahn S, Chung CY, Sung KH, Park MS (2012) Reliability and relationship of radiographic measurements in hallux valgus. Clin Orthop Relat Res 470(9):2613–2621. https://doi.org/10.1007/s11999-012-2368-6
Lee MS, Vanore JV, Thomas JL et al (2005) Clinical practice guideline adult flatfoot panel. Diagnosis and treatment of adult flatfoot. J Foot Ankle Surg 44(2):78–113. https://doi.org/10.1053/j.jfas.2004.12.001
Nery CA (2001) Hálux valgo. Rev Bras Ortop 36(6):183–200
Nix S, Smith M, Vicenzino B (2010) Prevalence of hallux valgus in the general population: a systematic review and meta-analysis. J Foot Ankle Res 3(1):1–9. https://doi.org/10.1186/1757-1146-3-21
Okuda H, Juman S, Ueda A, Miki T, Shima M (2014) Factors related to prevalence of hallux valgus in female university students: a cross-sectional study. J Epidemiol 24(3):200–208. https://doi.org/10.2188/jea.JE20130110
Perera AM, Mason L, Stephens MM (2011) The pathogenesis of hallux valgus. J Bone Joint Surg Am 93(17):1650–1661. https://doi.org/10.2106/JBJS.H.01630
Roddy E, Zhang W, Doherty M (2008) Prevalence and associations of hallux valgus in a primary care population. Arthritis Rheum 59(6):857–862. https://doi.org/10.1002/art.23709
Saragas NP, Becker PJ (1995) Comparative radiographic analysis of parameters in feet with and without hallux valgus. Foot Ankle Int 16(3):139–143. https://doi.org/10.1177/2F107110079501600306
Shelton TJ, Singh S, Bent Robinson E, Nardo L, Escobedo E, Jackson L, Kreulen CD, Giza E (2018) The influence of percentage weight-bearing on foot radiographs. Foot Ankle Spec 12(4):363–369. https://doi.org/10.1177/2F1938640018810412
Steinberg N, Finestone A, Noff M, Zeev A, Dar G (2013) Relationship between lower extremity alignment and hallux valgus in women. Foot Ankle Int 34(6):824–831. https://doi.org/10.1177/2F1071100713478407
Suh DH, Kim HJ, Park JH, Park YH, Koo BM, Choi GW (2021) Relationship between hallux valgus and pes planus in adult patients. J Foot Ankle Surg 60(2):297–301. https://doi.org/10.1053/j.jfas.2020.06.030
Thomas JL, Kunkel MW, Lopez R, Sparks D (2006) Radiographic values of the adult foot in a standardized population. J Foot Ankle Surg 45(1):3–12. https://doi.org/10.1053/j.jfas.2005.10.014
Wilkins EH (1941) Feet with particular reference to school children. Med Officer 66:5–29
Funding
There was no funding for this study.
Author information
Authors and Affiliations
Contributions
AKA: project development, study design, data collection, data analysis, statistics, manuscript writing. ŞDM: study design, data collection, FB: data collection, data analysis, supply of radiological data. MGB: study design, manuscript editing, supervision of the study, revision of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval
Ethical approval was waived by the Non-Invasive Clinical Research Ethics Committee of Çukurova University (11.06.2021/112) in view of the retrospective nature of the study and all the procedures being performed were part of the routine care.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Açikgöz, A.K., Mutluay, Ş.D., Binokay, F. et al. Evaluation of the relationship between hallux valgus and foot measurements in radiographic images of adult female. Surg Radiol Anat 44, 1281–1288 (2022). https://doi.org/10.1007/s00276-022-03012-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-022-03012-8