
Abstract
The right vertebral artery (VA) rarely arises from the right common carotid artery (CCA); however, the majority of anomalous right VAs are seen in combination with an aberrant right subclavian artery (SA). Independent (or isolated) right VA of the right CCA origin is extremely rare, with only a few cases reported previously. We herein report an additional case diagnosed incidentally using computed tomography angiography. This patient had a left VA arising from the aortic arch between the origins of the left CCA and left SA. The bilateral VAs took an anterior course and entered the C3 transverse foramina, at an extremely high level.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
According to a review article [6], the prevalence of the right vertebral artery (VA) arising from the right common carotid artery (CCA) is reported to be 0.14%, which is not extremely rare. However, the majority of patients with a right VA of right CCA origin also have an aberrant right subclavian artery (SA) [1,2,3, 7, 10]. Only a few cases of independent (or isolated) right VA arising from the right CCA have been reported in the relevant English-language literature [4, 5, 9].
We herein report an additional case diagnosed incidentally using computed tomography (CT) angiography. This patient also had a left VA arising from the aortic arch (AA) between the left CCA and left SA, the most prevalent VA origin variation. The bilateral VAs took an anterior course and entered the C3 transverse foramina (TF), at an extremely high level.
Case report
A 70-year-old woman with cerebral infarctions underwent craniocervical CT angiography for the evaluation of arterial lesions. The CT machine used was a 64-slice CT (SOMATOM Definition Flash; Siemens Healthineers, Erlangen, Germany). CT angiographic images were obtained using standard protocol. There was a stenotic lesion at the M1 segment of the right middle cerebral artery on CT angiography (not shown).
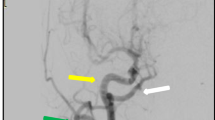
CT angiography of the neck region showed the right VA arising from the proximal right CCA, not from the right SA. There was no associated aberrant right SA. The left VA was hypoplastic and arose from the AA between the origins of the left CCA and left SA, not from the left SA. In addition, the bilateral VAs took an anterior course and entered the C3 TF (Fig. 1).

Slightly left anterior oblique (a) and right posterior oblique (b) projections of volume-rendering (VR) images of CT angiography show the right vertebral artery (VA) arising from the right common carotid artery (CCA) (long arrows). The hypoplastic left VA is arising from the aortic arch (AA) between the origins of the left CCA and left subclavian artery (SA) (short arrow). c AP projection of a VR image of CT angiography with the bone image shows that both VAs enter the C3 transverse foramina (long and short arrows). Bilateral carotid bifurcations are located at the level of the C3 vertebral bodies, slightly higher than usual. d Axial image of CT angiography (window level: 200 HU, window width: 400 HU, slice thickness: 2 mm) at the level of the C4 shows that bilateral VAs are located anteriorly, not in the transverse foramina (long and short arrows). e Axial image of CT angiography with same parameter at the level of the C3 shows that bilateral VAs are located in the transverse foramina (long and short arrows). The bilateral transverse foramina are larger than those of the C4
The patient was treated conservatively and showed a good clinical course.
Discussion
VA-originating variations are relatively common. The most common is the left VA arising from the AA between the origins of the left CCA and left SA, with a prevalence of approximately 4% [6, 9]. The second-most common variation is the right VA arising from the extremely proximal right SA, and its prevalence was reported to be approximately 3% [9]; however, this type of variation has not been widely recognized. Normally, seventh segmental arteries (LVA7 and RVA7) persist (Fig. 2a). These two common VA variations are formed when sixth segmental arteries (LVA6 and RVA6) persist instead of the LVA7 and RVA7, respectively (Fig. 2b). The prevalence of the right VA arising from the right CCA is reported to be 0.14% [6]. However, the majority of instances of this variation are associated with an aberrant right SA [1,2,3, 7, 10]. This relatively rare variation is formed when RVA6 persists instead of the RVA7, and the right AA regresses at the segment between the RVA6 and RSA (Fig. 2c).

Schematic illustrations of the double AA model modified from [9]. a Normally, the seventh segmental arteries (RVA7 and LVA7) persist, and the right AA regresses at the segment distal to the RSA (arrow). b In cases where the right VA arises from the extreme proximal right SA, the sixth segmental artery (RVA6) persists instead of the RVA7. In cases where the left VA arises from the AA between the origins of the left CCA and left SA, the LVA6 persists instead of the LVA7. c In cases where the right VA arises from the right CCA associated with an aberrant right SA, the RVA6 persists instead of the RVA7, and the right AA regresses at the segment between the RVA6 and RSA. d In the present case, the fifth segmental artery (RVA5) may have persisted instead of the RVA7, resulting in the right VA arising from the proximal right CCA instead of the right SA. The LVA6 also persisted instead of the LVA7, forming an AA-originating left VA
Our patient had a right VA arising from the proximal right CCA without an association with an aberrant right SA. Such independent (or isolated) right VA variation is extremely rare, and only a few cases have been reported [4, 5, 9]. Ishikawa et al. [4] speculated that when the fifth segmental artery (RVA5) persists instead of the RVA7, this variation may be formed. In their patient, the right CCA arose more distally than the normal point of the brachiocephalic trunk (BCT). Kesler et al. [5] reported a case of right VA arising from the mid portion of the right CCA, not from the proximal CCA. They speculated that when the fourth segmental artery (RVA4) persists instead of the RVA7, this variation may be formed. In our patient, the right VA arose from the proximal right VA, similar to the case reported by Ishihara, but the right CCA arose from the normal point of the BCT, similar to the case reported by Kesler. We concluded that the right VA origin variation in our patient was formed by the persistence of the RVA5 instead of the RVA7, as in the case reported by Ishikawa (Fig. 2d). Both our patient and Ishikawa’s patient had also a left VA with an AA origin, the most prevalent origin variation of the VA.
Approximately, 93%, 5%, 1%, and 1% of VAs enter the C6, C5, C4, and C7 TFs, respectively [9]. In addition, variations in the VA origin and level of entry into the TF are strongly related [9]. Extremely rarely, the VA enters the C3 TF [8]. The right VA of our patient entered the C3 TF, and the two of the three previously reported cases of independent (or isolated) right VA arising from the right CCA entered the C4 TF [4, 9]; the entry level of the TF was not described in the other case [5]. In both our patient and Ishikawa’s patient, the associating left VA of the AA origin entered the C3 TF. When the VA enters at a higher level of the TF, it takes an anterior course, which is a dangerous situation in cases requiring anterior neck surgery.
The clinical significance of these arterial variations is limited; however, to avoid complications, it is important to recognize the presence of these variations before performing anterior neck surgery. Recognition of these arterial variations before such a procedure is also important to both reduce the examination time and prevent failure of VA catheterization.
Conclusions
We encountered an extremely rare case of a right VA arising from the proximal right CCA without the association of an aberrant right SA. This variation may be formed when the fifth segmental artery persists instead of the seventh segmental artery. The right VA enters the C3 TF at an extremely high level. The anterior course it takes can make anterior neck surgery dangerous.
References
Ali A, Sedora Roman NI, Cox M, Kung D, Choudhri O, Hurst RW, Pukenas BA (2018) Anomalous origin of the right vertebral artery from the right common carotid artery. Cureus 10:e3602
Buffoli B, Verzeletti V, Hirtler L, Rezzani R, Rodella LF (2021) Retroeshophageal right subclavian artery associated with a bicarotid trunk and an ectopic origin of vertebral arteries. Surg Radiol Anat 43:1491–1495
Elnaggar ME, Abduljawad H, Assiri A, Ebrahim WH (2021) Anomalous origin of right vertebral artery from right common carotid artery. Radiol Case Rep 16:1574–1579
Ishikawa K, Yamanouchi T, Mamiya T, Shimato S, Nishizawa T, Kato K (2018) Independent anomalous origin of the right vertebral artery from the right common carotid artery. J Vasc Interv Neurol 10:25–27
Kesler WW, Sabat SB (2018) Isolated anomalous origin of the vertebral artery from the common carotid artery. Interact Cardiovasc Thorac Surg 27:615–616
Lazaridis N, Piagkou M, Loukas M, Piperaki ET, Totlis T, Noussios G, Natsis K (2018) A systematic classification of the vertebral artery variable origin: clinical and surgical implications. Surg Radiol Anat 40:779–797
Moshayedi P, Walker GB, Tavakoli S, Desai SM, Jadhav AP (2018) Dual origin of the right vertebral artery from the right common carotid and aberrant right subclavian arteries. J Clin Neurosci 53:258–260
Uchino A, Mochizuki A, Ishihara S (2021) Right vertebral artery entering the third transverse foramen diagnosed by magnetic resonance angiography: a report of two cases. Surg Radiol Anat 43:455–458
Uchino A, Saito N, Takahashi M, Okada Y, Kozawa E, Nishi N, Mizukoshi W, Nakajima R, Watanabe Y (2013) Variations in the origin of the vertebral artery and its level of entry into the transverse foramen diagnosed by CT angiography. Neuroradiology 55:585–594
Vitošević F, Vitošević Z, Rasulić L (2020) The right vertebral artery arising from the right common carotid artery: report of a rare case. Surg Radiol Anat 42:1263–1266
Author information
Authors and Affiliations
Contributions
AU carried out the study design and drafted the manuscript. All the authors reviewed the manuscript critically, and have read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
We declare that we have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Uchino, A., Tokushige, K. Right vertebral artery arising from the right common carotid artery without association with an aberrant right subclavian artery and entering the C3 transverse foramen. Surg Radiol Anat 44, 319–322 (2022). https://doi.org/10.1007/s00276-021-02861-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-021-02861-z