
Abstract
Anomalous origins of the vertebral arteries are uncommon and generally associated with other abnormalities of the supra-aortic vessels. We present an extremely rare case where the right vertebral artery is arising from the right common carotid artery, with an absent brachiocephalic trunk, and the right common carotid artery as the first branch of the aortic arch followed by right subclavian artery, without any other abnormalities of the supra-aortic vessels. This vessel variation can affect endovascular procedures, surgical interventions and cause some unexpected clinical symptoms.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Comprehensive knowledge about anatomy and anatomical variations of the aortic arch and its branches is crucial for endovascular head and neck procedures. The vertebral artery (VA) is generally the first branch of the ipsilateral subclavian artery (SCA). Anomalous origin of the right vertebral artery (RVA) is rarely seen compared to the left one and has mostly been described in combination with aberrant right subclavian artery (RSCA), whereby instead of being the first branch of brachiocephalic trunk, RSCA arises distal to the left subclavian artery (LSCA) and then curves back to reach the right side passing mostly posterior to the esophagus, sometimes causing dysphagia.
We present a rare case of a patient with the RVA arising from the cervical part of the right common carotid artery (RCCA), with an absent brachiocephalic trunk, and the RCCA as the first branch of the aortic arch, followed by RSCA, LCCA (left common carotid artery), and the LSCA.
Case report
A 62-year woman with hypertension presented to the emergency department with severe headache and right side ophthalmoplegia. Head CT, MRI and MRI angiography were performed and showed the aneurysm of the right posterior communicating artery (PCA). It was decided to perform the endovascular treatment of this aneurysm. During the pre-procedural digital subtraction angiography (DSA) imaging of the supra-aortic vessels it was seen that the RSCA and the RCCA are arising separately and directly from the aortic arch, with the absence of brachiocephalic trunk, and with the RCCA as the first branch of the aortic arch followed by RSCA. Moreover, the right vertebral artery was arising directly from the cervical part of the RCCA (Figs. 1, 2). Left vertebral artery was arising, as usual, from the posterosuperior aspect of the first part of the LSCA. The aneurysm of the right PCA was coiled and the patient was discharged in good clinical and neurological condition.

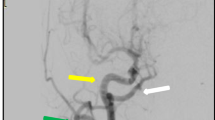
a Digital subtraction angiography of the aortic arch showing on antero-posterior view that the right vertebral artery is arising from the right common carotid artery, an absent brachiocephalic trunk, and the right common carotid artery as the first branch of the aortic arch, followed by right subclavian artery, left common carotid artery, and the left subclavian artery. b Outlined branches of the aortic arch on the antero-posterior view digital subtraction angiography: blue, right common carotid artery; yellow, right vertebral artery; red, right subclavian artery; green, left common carotid artery; white, left subclavian artery; purple, left vertebral artery (color figure online)

Antero-posterior view of the selective digital subtraction angiography of the right common carotid artery showing that the right vertebral artery is arising from the cervical part of the right common carotid artery
Discussion
Both the right and left vertebral arteries usually arise from the posterosuperior aspect of the first part of the SCA and extend inward and upward to the transverse process of C6, pass through the foramina of all of the upper cervical transverse processes, curve medially behind the lateral mass of the atlas, and then enter the cranium through the foramen magnum [8].
Anomalous VA origins are usually found incidentally on diagnostic imaging or preprocedural angiograms during endovascular neuro-interventional procedures. The most common variation of the VA origin is the LVA arising straight from the aortic arch between the LCCA and LSCA, with a prevalence of 2.4–5.8% [4, 6]. An aberrant RSCA is the most common vascular ring anomaly in the aortic arch, with a reported incidence of 0.5–2% [3]. The incidence of the RVA arising from the RCCA and an aberrant RSCA is 0.18% [8]. To our knowledge, a RVA arising from the RCCA, with a RCCA as the first branch of the aortic arch followed by RSCA, LCCA, and LSCA has not been described in literature [6, 8]. The only similar pattern found in the literature is described in the review article by Lazaridis et al. [6]. The difference is that the LVA arose directly from aortic arch, between the LCCA and LSCA, whereas in our case the LVA arose, as usual, from the posterosuperior aspect of the first part of the LSCA. Additional difference was that in our case the first branch of the aortic arch was the RCCA, followed by RSCA.
In their article Lazaridis et al. [6] made a systematic classification of the vertebral artery origin according to side and branching pattern; in a class where RVA originates from extra-aortic position and LVA originates in typical pattern, the most related type to our case is where RVA originates from RCCA, but with the present brachiocephalic trunk, and this type was named RV.2. and was found in 5 cases in their review as well as in one more case by Kesler et al. [4]; in a class where RVA originates from extra-aortic position and LVA originates directly from aortic arch, the most related type to our case is above mentioned pattern in which RVA originates from RCCA and LVA originates directly from aortic arch between LCCA and LSCA, and this type was named RV.LA.1.
In some rare cases, the RVA originates from aorta and even more rarely from descending part of aorta [6]. As a rare variation, RVA can originate directly from the aortic arch with the RVA originating from ascending aortic arch as the rarest of all variations [1]. A case has been described by Lippert and Pabst [7] where the RVA originated directly from the aortic arch between the RSCA and the RCCA in a case of missing brachiocephalic arteries [8]. Another rare variation is the origin between the LCCA and the LSCA [2, 10]. The most common anomalous origin of the RVA from aortic arch occurs from distal to the origin of the LSCA in which the RVA represents the last branch of the aortic arch and has a retro-esophageal course to reach its entry into the vertebral foramen [8].
Also, RVA can originate directly from other vessels such as brachiocephalic or innominate artery instead of the RSCA. In such cases, most commonly, RVA originates from the RCCA with the anomalous origin of the RSCA as the last branch of the aortic arch and a retro-esophageal course, known as arteria lusoria. In a study of 102 patients with this anomalous origin of RSCA, Tsai et al. [9] found a VA anomaly in 15.7% of patients [8]. Other rare variants of RVA origin may include right carotid bulb, right external carotid artery, right internal carotid artery and right thyrocervical trunk (RTCT) [6].
RVA may also have a dual origin, as two separate vessels, and in most cases both RVAs are emerging from RSCA. In rare cases RVA may have a dual origin from RTCT and RSCA [6].
Embryologically, the subclavian and vertebral arteries derive from the development and degeneration of the seven cervical intersegmental arteries arising from the dorsal aorta. The 1st to 6th intersegmental arteries degenerates at the 14–17-mm stage, whereas the 7th intersegmental artery develops into both the vertebral and subclavian arteries [4]. If the 1st to 6th intersegmental arteries fail to regress, anatomical variants may ensue. If the 1st or 2nd intersegmental artery persists, an abnormal origin of the VA from the internal or external carotid artery results. If the persistent artery occurs from the 3rd to the 6th intersegmental artery, a VA arising from the CCA or the aorta occurs [4]. The second occurrence is the more common one. Also, an anomalous origin of the VA is more common on the left than on the right side.
The fact that the right aortic arch degenerates between the RCCA and RSCA rather than distal to them, preventing the fusion of these vessels to form the brachiocephalic trunk so that both RCCA and RSCA arise separately, could explain the embryological aspect of the missing brachiocephalic trunk. Also, some growth factors and chromosome aberrations may have a role in different variations of aortic arch branching.
Although VA variants are typically asymptomatic, some authors suggested that direct aortic origin of a LVA with its C4 entrance into the transverse foramen could result in ataxia during head rotation and that such anomalies have been associated with arterial dissection likely due to increased shear forces [4]. Kim et al. [5] showed a correlation between anomalous origin of the VA and VA hypoplasia.
We have reported an isolated case with the RVA arising straight from the RCCA and an absent brachiocephalic trunk, therefore RCCA is the first branch of the aortic arch followed by RSCA, LCCA, and LSCA. Although this anatomical variant did not cause any certain symptoms in our patient, who was diagnosed with symptomatic brain aneurysm, it fits within the current concept of development of the aortic arch and its branches. Such variants and knowledge of anatomy and anatomical variations of the aortic arch and its branches is important for planning and performing surgical and endovascular procedures involving head and neck vessels.
References
Akdeniz B, Yilmaz E, Pekel N, Ergul BU (2007) Anomalous origin of the right vertebral artery from the ascending aorta in the presence of an aberrant right subclavian artery. Int J Cardiovasc Imag 23(1):39–42. https://doi.org/10.1007/s10554-006-9116-5
Albayram S, Gailloud P, Wasserman BA (2002) Bilateral arch origin of the vertebral arteries. AJNR Am J Neuroradiol 23:455–458
Epstein DA, Debord JR (2002) Abnormalities associated with aberrant right subclavian arteries—a case report. Vasc Endovascular Surg 36(4):297–303. https://doi.org/10.1177/153857440203600408
Kesler WW, Sabat SB (2018) Isolated anomalous origin of the vertebral artery from the common carotid artery. Interact Cardiovasc Thorac Surg 27(4):615–616. https://doi.org/10.1093/icvts/ivy141
Kim C, Sohn JH, Choi HC (2017) Are the anomalous vertebral arteries more hypoplastic? Retrospective linear mixed model approach. BMC Neurol 17(1):168. https://doi.org/10.1186/s12883-017-0951-x
Lazaridis N, Piagkou M, Loukas M et al (2018) A systematic classification of the vertebral artery variable origin: clinical and surgical implications. Surg Radiol Anat 40(7):779–797. https://doi.org/10.1007/s00276-018-1987-3
Lippert H, Pabst R (1985) Arterial variations in man, vol 6. JF Bergmann Verlag, Germany
Maiti TK, Konar SK, Bir S, Nanda A, Cuellar H (2016) Anomalous origin of the right vertebral artery: incidence and significance. World Neurosurg 89:601–610. https://doi.org/10.1016/j.wneu.2015.11.018
Tsai IC, Tzeng WS, Lee T et al (2007) Vertebral and carotid artery anomalies in patients with aberrant right subclavian arteries. Pediatr Radiol 37(10):1007–1012. https://doi.org/10.1007/s00247-007-0574-2
Wasserman BA, Mikulis DJ, Manzione JV (1992) Origin of the right vertebral artery from the left side of the aortic arch proximal to the origin of the left subclavian artery. AJNR Am J Neuroradiol 13:355–358
Funding
This study was not supported by any funding.
Author information
Authors and Affiliations
Contributions
Filip Vitošević: manuscript writing, data collection. Zdravko Vitošević: manuscript writing (review and editing). Lukas Rasulić: project development.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
For this type of study formal consent is not required.
Informed consent
For this type of study informed consent is not required.
Consent for publication
For this type of study consent for publication is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Vitošević, F., Vitošević, Z. & Rasulić, L. The right vertebral artery arising from the right common carotid artery: report of a rare case. Surg Radiol Anat 42, 1263–1266 (2020). https://doi.org/10.1007/s00276-020-02514-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-020-02514-7