
Abstract
We report an unusual and multiple variation involving the right head and neck veins which were found during routine dissection in a 50-year-old male cadaver, facial vein draining into both external and internal jugular veins, fenestration in external jugular vein transmitting the supraclavicular nerve trunk, the anterior division of the retromandibular vein draining into anterior jugular vein and the absence of the common facial vein. The knowledge about these variations is important during various surgical and diagnostic procedures involving head and neck region.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Head and neck region is drained by both superficial and deep veins. The superficial veins mainly receive the blood from face as well as scalp and drain into deep veins. Some of the superficial veins of the head and neck region include the facial vein (FV), retromandibular vein (RMV), anterior jugular vein (AJV) and external jugular vein (EJV). Among these the RMV is formed within substance of parotid gland by the union of both superficial temporal vein and maxillary vein. After emerging from the apex of parotid gland it divides into an anterior and posterior division. The anterior division unites with FV to form common facial vein (CFV) and drains into internal jugular vein (IJV). The posterior division unites with posterior auricular vein inferior to parotid gland to form EJV and empties into subclavian vein [10].
Variations involving the FV and EJV have been reported in the past [2, 6, 11]. Fenestration in EJV has also been reported in various studies [16, 18]. But variations involving the RMV, FV, AJV associated with the fenestration in EJV has not been reported yet to the best of our knowledge.
The anatomical knowledge of the venous variations of head and neck region are decisive to surgeons [17]. The ultrasound-guided venepuncture is a viable possibility in cases of variations in the patterns of superficial veins [7]. Both the EJV and FV have been used as a graft for the carotid endarterectomy [14]. The EJV has been known to have multiple uses. It is used for the insertion of temporary hemodialysis catheter [9], as a draining site for shunt procedures involving hydrocephalus surgery [2] and as a recipient vessel in head and neck reconstruction using free flap transfers [20]. The variations involving the FV is important during reconstructive surgeries and knowledge about these variations help to prevent intraoperative bleeding [13]. Literature also state that EJV with double segments raise the potential for deep vein thrombosis owing to the changes in flow velocities [4]. We present a unique case of multiple venous variations involving the veins of the head and neck region.
Case report
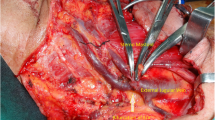
The multiple venous variations were observed on the right head and neck region of a 50-year-old male cadaver during routine dissection for undergraduates at JIPMER, Puducherry in February 2018. The posterior division of RMV and posterior auricular vein joined to form the EJV at the apex of parotid gland. EJV then descended downwards and backwards on the anterior surface of sternocleidomastoid and along the roof of posterior triangle. At a distance of 8.3 cm below the angle of mandible it presented a fenestration by dividing into anterior and posterior loops. The loops remained separate for a distance of 1.2 cm beyond which they fused to form single trunk, which then drained into the subclavian vein. The width of the EJV measured at 3 cm, 5 cm and 8 cm from angle of the mandible was 0.38 cm, 0.55 cm and 0.98 cm, respectively. The anterior loop had a width of 0.78 cm and received the AJV. The posterior loop had a width of 0.9 cm and received the posterior external jugular vein. Between the anterior and posterior loops emerged the trunk of supraclavicular nerves (Fig. 1a, b).

a Photograph showing the dissected right head and neck region with variant superficial veins following the reflection of sternocleidomastoid. b Schematic diagram showing the facial vein draining into external jugular vein, fenestration in external jugular vein transmitting the supraclavicular nerve trunk and the anterior division of retromandibular vein draining into anterior jugular vein. SCM sternocleidomastoid, FV facial vein, EJV external jugular vein, SCN supraclavicular nerve trunk, Black arrow fenestration in EJV, ARMV anterior division of retromandibular vein, AJV anterior jugular vein, PAG parotid gland, MA masseter, SMG submandibular gland, IJV internal jugular vein, CCA common carotid artery, OH omohyoid
The CFV was absent. The FV, after receiving the connecting veins V1 and V2 drained into the EJV at distance of 3.24 cm below the angle of mandible. The connecting veins V1 and V2 emerged at a distance of 2.58 cm and 2.84 cm below the angle of mandible from the FV. The anterior division of the RMV, after receiving the connecting vein V1, extended forwards and medially, draining into the AJV at the lower part of the neck region. The connecting vein V2 from FV joined the lingual and superior thyroid vein to form common thyrolinguofacial trunk (CTFT) which drained into the IJV. The connecting veins V1, V2 and CTFT measured 0.59 cm, 0.62 cm and 1.18 cm in length, respectively.
Discussion
The present case reports multiple venous abnormalities which include the absence of CFV, FV draining into both EJV and IJV, fenestration in EJV transmitting the supraclavicular nerve trunk and the anterior division of RMV draining into AJV.
Previous studies have reported the draining of the CFV into EJV [6, 11, 13]. Chauhan et al. reported the absence of CFV associated with an abnormal communicating channel between the proximal ends of anterior and external jugular venous systems [3]. Others have reported the absence of CFV associated with undivided RMV [2, 7, 13, 17]. The present case differs from above that it describes the absence of CFV associated with multiple venous variation, and thus not similar to the earlier reported cases. The FV draining into EJV associated with undivided RMV has been reported previously with an incidence varying between 1 and 30.8% [2, 6, 7, 13]. In the present report, the FV drained into both the EJV and IJV. The RMV also divided to form both the anterior and posterior divisions. These variations differed from the previous literature and to best of our knowledge has not been reported yet.
The cervical branch of facial nerve passing through the fenestrated EJV has been reported earlier [5]. Snoj and Cvetko reported a case of fenestration of EJV associated with its duplication [5, 18]. Singla et al. reported fenestration of EJV forming a venous ring around the supraclavicular nerves corroborating the findings in present case [16]. In addition, in the present study the anterior loop received the AJV and anterior division of RMV drained into AJV thus differing from the above reports. The AJV usually begins in the suprahyoid region through the confluence of several superficial veins and has variable communications with the retromandibular or the facial vein and the IJV [15].
Venous development of head and neck itself is an intricate and complex process. In 5 mm stage of embryo the venous blood of mandibular and hyoid arches is drained into the common cardinal vein by the ventral pharyngeal vein (VPV). At 10 mm stage of embryo as the neck elongates the termination of VPV is shifted to the cranial part of the precardinal vein which later becomes the IJV. Located more cranial to VPV is the primitive maxillary vein (PMV) which drains the blood from the area of head and neck region supplied by trigeminal nerve [2]. As the development proceeds the VPV receives tributaries from the face and tongue to become linguofacial vein (LFV) [19]. As the stem of the PMV reduces in size, its posterolateral tributary anastomoses with prominent lateral tributary of LFV. The LFV now becomes the FV and receives the RMV from temporal region at 18 mm stage of embryo. The stem of FV beyond drainage of RMV forms the CFV and drains into IJV [12].
Simultaneously the primitive cephalic vein and jugulocephalic vein form a venous plexus around the developing clavicle. At 22 mm stage of embryo, a cranial tributary from this plexus grows larger in the neck region indicating the emergence of EJV. As the embryo develops, the jugulocephalic vein disappears and the craniodorsal part of the venous ring forms the trunk of the adult EJV [12]. Thus, the EJV arises as a secondary channel from a capillary plexus in the facial region [8]. The developing EJV at its cranial end establishes anterior and posterior communications with the FV and RMV, respectively. The posterior auricular vein drains into posterior communication and forms the posterior division of RMV whereas the anterior communication regresses during a normal course of development [1, 13]. The anterior jugular vein normally develops from venous plexus around head mesenchyme [3].
Any developmental errors occurring at crucial stages of development results in abnormal venous patterns. Thus, in present case the fenestration of EJV could be due to defects in the development of its wall. Also in the present case, the persistence of the anterior communication of EJV with FV, disappearance of the complete CFV and terminal part of RMV has led to drainage of FV into both EJV and IJV. With the disappearance of CFV the anterior division of RMV could have established a secondary communications with AJV as well as with the FV.
An insight into variations of the superficial veins of head and neck help in surgical planning to reduce the chances of iatrogenic injuries. The knowledge of these variations would also be useful to radiologists during procedures of head and neck region.
Conclusion
Multiple anatomical variations are observed involving the CFV, EJV and IJV. Abnormal changes during the development from 5 mm stage to 22 mm stage of embryo are responsible for venous anomalies of head and neck. Awareness about the venous variation is important for surgeons and interventional radiologists before attempting any procedure in the region.
References
Balachandra N, Padmalatha K, Prakash BS, Ramesh BR (2012) Variation of the veins of the head and neck—external jugular vein and facial vein. Int J Anat Var 5:99–101
Choudhry R, Tuli A, Choudhry S (1997) Facial vein terminating in the external jugular vein. Surg Radiol Anat 19:73–77
Chauhan NK, Rani A, Chopra J, Srivastava AK, Kumar V (2011) Anomalous formation of external jugular vein and its clinical implication. Natl J Maxillofac Surg 2:51–53
Cvetko E (2015) A case of left-sided absence and right-sided fenestration of the external jugular vein and a review of the literature. Surg Radiol Anat 37:883–886
Cvetko E (2013) A case of unilateral fenestration of the external jugular vein, through which the cervical branch of the facial nerve passes. Anat Sci Int 88:151–152
D’Silva SS, Pulakunta T, Potu BK (2008) Termination of the facial vein into the external jugular vein: an anatomical variation. J Vasc Bras 7:174–175
Gupta V, Tuli A, Choudhry R, Agarwal S, Mangal A (2003) Facial vein draining into external jugular vein in humans: its variations, phylogenetic retention and clinical relevance. Surg Radiol Anat 25:36–41
Hamilton WJ, Boyd JD, Mossamn HW (1972) Human embryology: prenatal development of form and function, 4th edn. William & Wilkins, Baltimore
Moini M, Rasouli MR, Kenari MM, Mahmoodi HR (2009) Non-cuffed dual lumen catheters in the external jugular veins versus other central veins for hemodialysis patients. Saudi J Kidney Dis Transpl 20:44
Moore KL, Dalley AF, Agur AMR (2014) Clinically oriented anatomy, 7th edn. Lippincott Williams & Wilkins, Philadelphia
Murali P, Sundarapandian S (2016) Unusual variation of the veins of the head and neck: external jugular vein and facial vein. Res J Pharm Biol Chem Sci 7:2510–2513
Padget DH (1957) The development of the cranial venous system in man, from the viewpoint of comparative anatomy. Contrib Embryol Carnegie Instn Wash Publ 247:79–140
Pai M, Vadgaonkar R, Prabhu L, Shetty P (2008) The different termination patterns of the facial vein: a cadaveric study. Fırat Tıp Derg 13:32–34
Sabharwal P, Mukherjee D (1998) Autogenous common facial vein or external jugular vein patch for carotid endarterectomy. Cardiovasc Surg 6:594–597
Schummer W, Schummer C, Bredle D, Frober R (2004) The anterior jugular venous system: variability and clinical impact. Anesth Analg 99:1625–1629
Singla RK, Singla S, Sachdeva K (2011) Partial duplication of external jugular vein forming a venous ring around supraclavicular nerve: a case report. J Clin Diagn Res 5:859–861
Silva MRMA, Henriques JGB, Silva JH, Camargos VR, Moreira PR (2016) Venous arrangement of the head and neck in humans anatomic variability and its clinical inferences. J Morphol Sci 33:22–28
Snoj Z, Cvetko E (2013) A case of unilateral fenestration and duplication of the external jugular vein. Int J Morphol 31:107–109
Borley StrandingS. Gray NR.H (2016) Gray’s anatomy: the anatomical basis of clinical practice, 41st edn. Churchill Livingstone/Elsevier, Edinburgh
Yagi S, Suyama Y, Fukuoka K, Takeuchi H, Kitano H (2016) Recipient vessel selection in head and neck reconstruction based on the type of neck dissection. Yonago Acta Med 59:159–162
Author information
Authors and Affiliations
Contributions
PCV: data collection, manuscript writing. SSSNR manuscript writing & editing. VG manuscript writing & editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical standards
We state that the present report complies with the current laws of the country in which it was performed.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Vani, P.C., Rajasekhar, S.S.S.N. & Gladwin, V. Unusual and multiple variations of head and neck veins: a case report. Surg Radiol Anat 41, 535–538 (2019). https://doi.org/10.1007/s00276-019-02203-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-019-02203-0