
Abstract
The anatomy of hepatic arteries is one of the most variable. Accurate awareness of all the possible anatomic variations is crucial in the upper GI surgery and especially in liver and pancreas transplantation. The most frequent anatomical variants are: a replaced or accessory right hepatic artery (RHA) from the superior mesenteric artery (6.3–21 %), a replaced or accessory left hepatic artery (LHA) from the left gastric artery (LGA) (3–18 %) or a combination of these two variants (up to 7.4 %). Herein, we describe the case of a 67-year-old cadaveric organ donor who presented a RHA originating from the splenic artery (SA) associated with both a CHA originating from the celiac trunk (CT) and a LHA originating from the LGA.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The anatomy of hepatic arteries is one of the most variable. Accurate awareness of all the possible anatomic variations is crucial in the upper GI surgery and especially in liver and pancreas transplantation. Liver is usually vascularized by the common hepatic artery (CHA) that originates from the celiac trunk (CT) and is divided into a right and a left branch (51–85.1 %) [1, 3–28].
The most frequent anatomical variants are: a replaced or accessory right hepatic artery (RHA) from the superior mesenteric artery (SMA) (6.3–21 %), a replaced or accessory left hepatic artery (LHA) from the left gastric artery (LGA) (3–18 %) or a combination of these two variants (up to 7.4 %) (Table 1).
Herein, we describe the case of a 67 years old cadaveric organ donor who presented a RHA originating from the splenic artery (SA), associated with both a CHA originating from the celiac trunk (CT) and a LHA from the LGA. A detailed review of the literature on vascularization of the liver was carried out.
Materials and methods
We performed a review of the literature on Pubmed, Embase and Web of Knowledge using the following keywords: “hepatic artery variant”, “hepatic artery”, “right hepatic artery”, “hepatic vascularization”. Italian, English and French language articles were selected without temporal limits. We found 1245 articles matching the above keywords. The objectives of the review were to describe the frequency of hepatic artery variants and to evaluate the presence of previous reports describing RHA off SA. We used the accuracy of anatomical description of celiac axis and hepatic arteries as the principal criteria to select articles. By analysing the abstracts of the articles, we selected 41 retrospective papers. 27 articles detailed satisfactorily the anatomical variants, with clear numbers and percentages according to the most common classifications. In addition, we searched for case reports describing the celiac and hepatic anatomy. We found 156 case reports/little case series which treated the above matter.
Case report
In May 2014, an en-bloc abdominal procurement (liver, pancreas in toto, spleen, aorta patch with CT and SMA origin) was sent from an external surgery team to the Liver transplant Unit of Ospedale Maggiore Policlinico di Milano. The procurement was performed on a 67 year old cadaveric organ donor. During the dissection manoeuvres at back table, we found a RHA originating from the splenic artery, associated with a CHA originating from the celiac trunk and a LHA from the LGA (Fig. 1).

Pictures of the liver on back table. CT Celiac trunk, SA splenic artery, RHA right hepatic artery, CHA common hepatic artery, GDA gastroduodenal artery, LHA left hepatic artery, LGA left gastric artery, PV portal vein
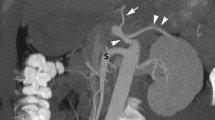
In the case being analysed the CT was divided in SA, CHA and LGA without the presence of hepatic vessels from SMA. The distance between CT and SMA was 1.1 cm. The diameter of the right hepatic artery was 3–4 mm; it originated from the splenic artery, 4 mm after the CT division. The right hepatic artery’s course was downward and parallel in respect of the common hepatic artery, at the top of the pancreas. It then moved behind the gastroduodenal artery and the bile duct. Finally it goes up at the right side of the portal vein, which is the standard anatomical position of the RHA off the superior mesenteric artery (Fig. 2). The course of the LHA from the LGA was standard. No arterial reconstructions on back table were needed. During liver transplantation the arterial anastomosis was performed between the donor CT and the recipient CHA. Our patient was discharged on XV postoperative day after a regular course.

Schematic description of the hepatic artery variant. CT Celiac trunk, SA splenic artery, RHA right hepatic artery, CHA common hepatic artery, GDA gastroduodenal artery, LHA left hepatic artery, LGA left gastric artery, CBD common bile duct, PV portal vein
Discussion
The definition of anatomical variant is used to define the morphology of a particular structure which deviates from the anatomical configuration observed in the majority of individuals. Therefore, the anatomical variant is a change from the normal or modal configuration. Although not pathological, anatomical variants may make diagnostic or operative procedures more complex. Changes in hepatic vascularization were first defined by Michels’ classification [19] who in 1962 described ten types of arterial variants. Rarer cases include a CHA from SMA and a CHA which arises from LGA. A more simple and recent classification was proposed by Hiatt et al. [13] in 1994.
The prevalence of hepatic artery variants outside these two classifications was reported between 0 and 19 % (Table 1).
We analysed 27 works with a total of 11.193 hepatic artery anatomy descriptions [1, 3–28].
The analysis of the literature highlighted a high variability in hepatic vascularization (14.9–49 %) which may arise in different combinations: from celiac trunk or one of its branches, from the SMA and/or directly from the aorta. The splenic artery is the arterial branch of the celiac trunk which is the less interested in liver vascularization.
From the analysis performed we found three cases of left hepatic artery arising from the splenic artery. None of the 27 papers we analysed (Table 1) reported a right hepatic artery originating from the splenic artery. Even among the 156 case reports and little case series no evidence of this variant was found. Moreover, we became aware of a recent Russian analysis of 4315 angiographic evaluations, not reported in Table 1 because it was presented at the GEST 2014 congress (Balakhnin PV et al. Classification of hepatic artery anatomic variants for intra-arterial therapy: analysis of 4315 angiographic studies. GEST 2014, poster session). Even in this large series of cases the origin of a RHA from SA was absent.
Conclusions
The presence of a RHA from the SA is very rare: whilst we are aware that it is not possible to say with certainty that all scientific contributions in every language from every country have been taken into account, as far as we know, this case report appears to be the first describing this kind of variant. We analysed more than 11,000 cases reporting hepatic artery anatomy before finding a RHA off the SA. It has been estimated that there are approximately 11,000 three-leaf clovers for every four-leaf clover [2]. What an interesting similarity.
Abbreviations
- CHA:
-
Common hepatic artery
- RHA:
-
Right hepatic artery
- LHA:
-
Left hepatic artery
- SA:
-
Splenic artery
- LGA:
-
Left gastric artery
- CT:
-
Celiac trunk
- SMA:
-
Superior mesenteric artery
- PV:
-
Portal vein
References
Allen PJ, Stojadinovic A, Ben-Porat L et al (2002) The management of variant arterial anatomy during hepatic arterial infusion pump placement. Ann Surg Oncol 9:875–880
Bradley D (2008) “Five-leaf clovers”. http://www.sciencebase.com/science-blog/five-leaf-clovers.html
Burke D, Earlam S, Fordi C, Allen-Mersh TG (1995) Effect of aberrant hepatic arterial anatomy on tumor response to hepatic artery infusion of floxuridine for colorectal liver metastases. Br J Surg 82:1098–1100
Coşkun M, Kayahan EM, Ozbek O et al (2005) Imaging of hepatic arterial anatomy for depicting vascular variations in living related liver transplant donor candidates with multidetector computed tomography: comparison with conventional angiography. Transpl Proc 37:1070–1073
Covey AM, Brody LA, Maluccio MA et al (2002) Variant hepatic arterial anatomy revisited: digital subtraction angiography performed in 600 patients. Radiology 224:542–547
Curley SA, Chase JL, Roh MS et al (1993) Technical consideration and complications associated with the placement of 180 implantable hepatic arterial infusion devices. Surgery 114:928–935
De Cecco CN, Ferrari R, Rengo M et al (2009) Anatomic variations of the hepatic arteries in 250 patients studied with 64-row CT angiography. Eur Radiol 19:2765–2770
De Santis M, Ariosi P, Calò GF et al (2000) Hepatic arterial vascular anatomy and its variants. Radiol Med 100:145–151
Egorov VI, Yashina NI, Fedorov AV et al (2010) Celiaco-mesenterial arterial aberrations in patients undergoing extended pancreatic resections: correlation of CT angiography with findings at surgery. JOP 11:348–357
Gruttadauria S, Foglieni CS, Doria C et al (2001) The hepatic artery in liver transplantation and surgery: vascular anomalies in 701 cases. Clin Transpl 15:359–363
Gümüs H, Bükte Y, Özdemir E et al (2013) Variations of the celiac trunk and hepatic arteries: a study with 64-detector computed tomographic angiography. Eur Rev Med Pharmacol Sci 17:1636–1641
Hardy KJ, Jones RM (1994) Hepatic artery anatomy in relation to reconstruction in liver transplantation: some unusual variations. Aust N Z J Surg 64:437–440
Hiatt JR, Gabbay J, Busuttil RW (1994) Surgical anatomy of the hepatic arteries in 1000 cases. Ann Surg 220:50–52
Kemeny MM, Hogan JM, Goldberg DA et al (1986) Continuous hepatic artery infusion with an implantable pump: problems with hepatic artery anomalies. Surgery 99:501–504
Koops A, Wojciechowski B, Broering DC et al (2004) Anatomic variations of the hepatic arteries in 604 selective celiac and superior mesenteric angiographies. Surg Radiol Anat 26:239–244
Lopez-Andujar R, Moya A, Montalva E et al (2007) Lessons learned from anatomic variants of the hepatic artery in 1081 transplanted livers. Liver Transpl 13:1401–1404
Löschner C, Nagel SN, Kausche S et al (2015) Hepatic arterial supply in 1297 CT-angiographies. Rofo 187:276–282
Mäkisalo H, Chaib E, Krokos N et al (1993) Hepatic arterial variations and liver-related diseases of 100 consecutive donors. Transpl Int 6:325–329
Michels NA (1962) Newer anatomy of the liver and its variant blood supply and collateral circulation. Am J Surg 112:337–347
Niederhuber JE, Ensminger WD (1983) Surgical consideration in the management of hepatic neoplasia. Semin Oncol 10:135–147
Rong GH, Sindelar WF (1987) Aberrant peripancreatic arterial anatomy: consideration in performing pancreatectomy for malignant neoplasms. Am Surg 53:726–729
Rygaard H, Forrest M, Mygind T et al (1986) Anatomic variants of the hepatic arteries. Acta Radiol Diagn (Stockh) 27:425–427
Saba L, Mallarini G (2011) Anatomic variations of arterial liver vascularization: an analysis by using MDCTA. Surg Radiol Anat 33:559–568
Soin AS, Friend PJ, Rasmussen A et al (1996) Donor arterial variations in liver transplantation: management and outcome of 527 consecutive grafts. Br J Surg 83:637–641
Stemmler BJ, Paulson EK, Thornton FJ et al (2004) Dual-phase 3D MDCT angiography for evaluation of the liver before hepatic resection. Am J Roentgenol 183:1551–1557
Suzuki T, Nakayasu A, Kawabe K et al (1971) Surgical significance of anatomic variations of the hepatic artery. Am J Surg 122:505–512
Varotti G, Gondolesi GE, Goldman J et al (2004) Anatomic variations in right liver living donors. J Am Coll Surg 198:577–582
Winston CB, Lee NA, Jarnagin WR et al (2007) CT angiography for delineation of celiac and superior mesenteric artery variants in patients undergoing hepatobiliary and pancreatic surgery. Am J Roentgenol 189:W13–W19
Acknowledgments
The authors thank Benedetta Furgiuele and Adam Bisoffi for their contributions.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that no conflict of interest exists.
Ethical standards
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Informed consent
Informed consent was obtained from all patients for being included in the study.
Additional informed consent was obtained from all patients for which identifying information is included in this article.
All institutional and national guidelines for the care and use of laboratory animals were followed.
Rights and permissions
About this article

Cite this article
Caruso, F., Dondossola, D., Fornoni, G. et al. Right hepatic artery from splenic artery: the four-leaf clover of hepatic surgery. Surg Radiol Anat 38, 867–871 (2016). https://doi.org/10.1007/s00276-016-1617-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-016-1617-x