
Abstract
Purpose
Transjugular intrahepatic portosystemic shunt (TIPS) creation is considered as being one of the most complex procedures in abdominal interventional radiology. Our aim was twofold: quantification of TIPS-related patient radiation exposure in our center and identification of factors leading to reduced radiation exposure.
Materials and methods
Three hundred and forty seven consecutive patients underwent TIPS in our center between 2007 and 2014. Three main procedure categories were identified: Group I (n = 88)—fluoroscopic-guided portal vein targeting, procedure done in an image intensifier-based angiographic system (IIDS); Group II (n = 48)—ultrasound-guided portal vein puncture, procedure done in an IIDS; and Group III (n = 211)—ultrasound-guided portal vein puncture, procedure done in a flat panel detector-based system (FPDS). Radiation exposure (dose-area product [DAP], in Gy cm2 and fluoroscopy time [FT] in minutes) was retrospectively analyzed.
Results
DAP was significantly higher in Group I (mean ± SD 360 ± 298; median 287; 75th percentile 389 Gy cm2) as compared to Group II (217 ± 130; 178; 276 Gy cm2; p = 0.002) and Group III (129 ± 117; 70; 150 Gy cm2 p < 0.001). The difference in DAP between Groups II and III was also significant (p < 0.001). Group I had significantly longer FT (25.78 ± 13.52 min) as compared to Group II (20.45 ± 10.87 min; p = 0.02) and Group III (19.76 ± 13.34; p < 0.001). FT was not significantly different between Groups II and III (p = 0.73).
Conclusions
Real-time ultrasound-guided targeting of the portal venous system during TIPS creation results in a significantly lower radiation exposure and reduced FT. Further reduction in radiation exposure can be achieved through the use of modern angiographic units with FPDS.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Transjugular intrahepatic portosystemic shunt (TIPS) creation is considered as being one of the most complex and radiation intensive procedures in abdominal interventional radiology [1]. Since its introduction in the 1980s, TIPS continues to play an important role in managing the complications of portal hypertension by creating the equivalent of a surgical side-to-side portocaval shunt. The most technically challenging step of the procedure, and frequently the longest, is the so-called ‘blind puncture’ of the portal vein following hepatic venous access. This step is considered as being high risk, since it may result in puncture of the liver capsule, gallbladder, biliary tree, or vascular structures such as the hepatic artery and vena cava. In general, the fewer passes required to achieve portal access, the safer the procedure. Several approaches have been proposed to minimize the number of needle passes required to catheterize the intrahepatic portal venous system. These include the use of bony landmarks, direct transhepatic catheterization of the portal vein, transarterial mesenteric indirect portography, indirect portography through a wedged catheter in the hepatic venous system (using iodinated contrast or carbon dioxide), placement of a metallic marker, and real-time sonographic guidance [2–8]. Few studies have investigated the radiation dose associated with TIPS and how its magnitude is affected by technical parameters [1, 9–13]. Our aim was to quantify TIPS-related patient radiation exposure in our center, and also to identify any factors leading to reduced radiation exposure.
Materials and Methods
Institutional review board approval was obtained for this retrospective study, even though no specific informed consent was required. An informed consent specific to TIPS was obtained in all cases. No financial support has been provided for this study.
All procedures performed in studies were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Patient Population
From July 1999 to January 2015, 594 TIPS creations were performed in patients with complications of portal hypertension in the Interventional Radiology Department of a single transplant center. Dosimetric data for every TIPS procedure was systematically archived into our radiology information system (RIS) and picture archiving and communication system (PACS) (Centricity RIS 4.2i, General Electric Medical Systems, USA) as from January 2007.
Three hundred and forty seven consecutive TIPS creations were performed between January 2007 and January 2015, these constitute our study group. Patient characteristics are reported in Table 1.
Three main procedure categories were identified based on different generations of angiographic systems and radiological technique used: Group I—fluoroscopic-guided portal vein targeting with the use of bony landmarks, procedure done in an image intensifier-based angiographic system (IIDS); Group II—ultrasound-guided portal vein puncture, procedure done in an IIDS; and Group III—ultrasound-guided portal vein puncture, procedure done in a flat panel detector-based system (FPDS).
For every procedure the dose-area product (DAP) given in Gy cm2, fluoroscopy time (FT) given in minutes, and iodinate contrast material (ICM) volume given in milliliters (ml) were retrospectively documented. DAP (or Kerma-area-product) was considered as a surrogate measurement of the entire amount of energy delivered to the patient by the radiation beam during the procedure and is the quantity recommended by the International Commission on Radiation Units to measure patient doses in interventional radiology [14]. FT and volume of ICM were considered as surrogate marker of procedural complexity. The Society of Interventional Radiology–Cardiovascular and Interventional Radiology Society of Europe (SIR–CIRSE) international guideline on patient radiation management states that fluoroscopy time should not be used to monitor patient irradiation during interventional procedures; however, fluoroscopy time might provide an indication of procedure complexity, but it does not always correlate with other dose metrics [15, 16].
Angiographic Equipment
Procedures were performed in an angiographic suite with an image intensifier-based digital system (IIDS) (Advantax, General Electric Medical Systems, USA) during the period spanning January 2007 to July 2010. Procedures performed after July 2010 were performed in a flat-panel-based detector angiographic suite (FPDS) (Innova 4100, General Electric Medical Systems, USA). In both angiographic systems DAP and FT were measured with a dual channel DIAMENTOR M4-KDK DAP/Dose meter transmission ion chamber (PTW, Freiburg, Germany) fixed to the collimator with a valid calibration and quality control certificate revalidated every 6 months. DAP and FT values were archived into our RIS/PACS system at the end of every procedure. Standard dose reduction measures were routinely employed. These included tight collimation limited only to the region of interest, and a low object-to-detector and source-to-image distance. Low-frame rate pulsed fluoroscopy (7.5 frames/sec in FFDS, 12.5 frames/sec in IIDS) without magnification was routinely employed in procedures performed using both IIDS and FFDS. High frame rates (up to 15–30 frames/sec) and/or magnification was only used when absolutely necessary in technically challenging cases, during the most critical steps such as the stent deployment in obese patients. Fluoroscopy protocols were optimized in each system. The automatic exposure control system, designed to automatically determine the optimal technique parameters such as kV, mAs, focal spot size, and spectral filtration, was used in both systems. The ‘last image hold feature’, which displays the last active fluoroscopic image, was always used since this enables image-capture without additional fluoroscopic exposure.
Interventional Procedure
All procedures were carried out by three faculty-level radiologists with 24, 14, and 11 years of experience in abdominal interventional radiology, respectively, at the time of writing of this manuscript.
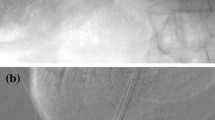
All procedures were performed under general anesthesia, using the Ring Transjugular Intrahepatic Access Set (CooK, Bloomington, USA). Ultrasound guidance was used to puncture the right internal jugular vein, and a left sided jugular approach was undertaken whenever this was not possible. A Cobra-2 catheter and a hydrophilic wire were used to catheterize the right hepatic vein, with the alternative being the middle hepatic vein. In the procedures performed between January 2007 and July 2009 access to a portal vein branch was achieved by aiming and advancing the Colapinto needle from the right/middle hepatic vein toward the projection of the 11th rib, approximately 0.5–1.5 vertebral body widths from the lateral border of the spine. These bony landmarks usually correspond to the location of the right portal vein. In procedures performed after August 2009, the Colapinto needle was advanced into the portal venous system under real-time ultrasound guidance (Fig. 1) using the 3.5 MHz curvilinear transducer of a GE Logiq E9 ultrasound machine (GE Healthcare, Milwaukee, WI). In all procedures, steady negative pressure was applied using a syringe secured to the Colapinto needle, while the latter was being withdrawn at a slow pace. Contrast was injected when blood was aspirated to confirm cannulation of the portal venous system. A hydrophilic guidewire was then used to gain access to the main portal vein, following which direct portography and portosystemic pressure gradient measurement were performed. Dilatation of the intrahepatic tract was performed with an 8 mm BlueMax balloon catheter (Boston Scientific, Natick, MA). Subsequently an e-PTFE covered stent (Viatorr®; W.L.GORE & Associates, Inc. Flagstaff, Az) was deployed and ballooned. Direct portography was then performed again following measurement of the post-TIPS portosystemic pressure gradient. In few cases, TIPS creation was combined with gastro-esophageal variceal coil embolization.

Two sterile fields are prepared, one over the right jugular area, the other over the right anterolateral abdominal wall (A), with two corresponding windows (B). The abdominal sterile area will be used during real-time sonographic visualization of the Colapinto needle, and in guiding transit of the needle from the hepatic vein to the intrahepatic portal vein radicle. The ultrasound probe is covered with a sterile probe-cover and maneuvered by the operator who remains at the head of the patient (C)
Non-ionic ICM was used during all procedures (Visipaque 320 mgI/ml, Amersham Health, Italy). A power injector (Mark V ProVis® Angiographic Injection System, MEDRAD, Pittsburgh, Penn.) was always used for both direct portograms. The majority of the procedures were performed with the detector in the anteroposterior projection and with no cranio-caudal or oblique tilting.
Statistical Analysis
The dosimetric and contrast-related data for all three groups was inputted in an Excel 2007 spreadsheet (Microsoft, Richmond, WA). DAP-, FT-, and ICM-related data were analyzed for each group, and expressed as the mean value ± standard deviation and median. The differences in DAP, FT, and ICM within each group was analyzed using two-tailed T tests. All statistical results were considered significant when a p value of less than 0.05 was reached.
Results
The overall mean DAP across all three groups was 235 ± 198 Gy cm2, with a mean FT of 21.99 ± 12.57 min. The overall mean volume of ICM corresponded to 120 ± 39 ml.
Group I consisted of eighty-eight procedures, with a mean DAP of 360 ± 298 Gy cm2, mean FT of 25.78 ± 13.52 min, and a mean ICM volume of 166 ± 91 ml. Forty-eight procedures were performed in Group II, with a mean DAP of 217 ± 130 Gy cm2, mean FT of 20.45 ± 10.87 min, and mean ICM volume of 107 ± 58 ml. Group III encompassed two hundred and eleven procedures with a mean DAP of 129 ± 117 Gy cm2, mean FT of 19.76 ± 13.34 min, and a mean ICM volume of 88 ± 30 ml (Table 2).
As expected, there was a wide variation in radiation exposure and the collected data exhibited asymmetric and typically non-Gaussian distributions (Fig. 2). DAP (360 ± 298 Gy cm2) was significantly higher in Group I as compared to Group II (217 ± 130 Gy cm2; p = 0.002) and Group III (129 ± 117 Gy cm2 p < 0.001). The difference in DAP between Group II and III was also significant (p < 0.001).

DAP distribution in TIPS creation for Groups I–III
Group I had significantly longer FT (25.78 ± 13.52 min) as compared to Group II (20.45 ± 10.87 min; p = 0.02) and Group III (19.76 ± 13.34; p < 0.001). FT was not significantly different between Groups II and III (p = 0.73).
The volume of ICM used was significantly higher in Group I (166 ± 91 ml) as compared to Group II (107 ± 58 ml, p = 0.0002) and also Group III (88 ± 30 ml, p < 0.001). A statistically significant difference was also seen on comparing Groups II and III (p = 0.002) (Fig. 3).

Histograms showing differences in DAP (A), FT (B), and ICM (C) among Groups I–III
Technical success was achieved in all procedures. One procedure in Group III, requiring a combined transhepatic/transjugular approach, was complicated by a large hemothorax few hours after the end of the TIPS creation, requiring surgical drainage. This patient had a previous liver transplant, with the indication for TIPS being refractory ascites for cirrhosis recurrence. This approach was used due to an unusually acute angle between the hepatic vein and the portal venous branch. No other major procedure-related bleeding complication was recorded in the study group.
No deterministic or stochastic complications were observed in our study group with a mean follow-up of 4 years (range 3 months to 8 years).
Discussion
As expected, radiation exposure in our cohort of patients varied according to the complexity of the procedure, with a wide range in DAP, FT and ICM volume used. The mean radiation exposure in TIPS creation was reduced by 65 % when performing TIPS using our commercially available FPDS with the use of real-time sonographic portal vein targeting, as compared to TIPS performed in an IIDS and portal vein targeting through the use of bony landmarks.
The data available regarding patient radiation exposure during TIPS is sparse. The largest series available is the RAD-IR study authored by Miller et al. [1], which reported a mean DAP of 335 Gy cm2 and a mean FT 38.7 min in 134 TIPS. Based on this, in a secondary analysis, Miller et al. [9] proposed a DAP reference level of 525 Gy cm2 and a FT reference level of 60 min for TIPS creation.
A significant variability in DAP and FT was reported in other series, this can be explained by the small number of procedures analyzed. Pinto et al. [10] reported a mean DAP of 340 Gy cm2 in 12 procedures. Zweers et al. [11], reported data on procedures performed in two different hospitals with a mean DAP of 226 Gy cm2 and median FT of 32 min in one hospital (n = 14) and a mean DAP of 77 Gy cm2 and median FT of 59 min in the second hospital (n = 9). Hidajat et al. [12] reported a mean DAP of 446 Gy cm2 and a mean FT of 77 min in 18 patients. Livingstone et al. [13] reported a mean DAP of 63 Gy cm2 and a mean FT of 19.2 min in 19 patients with the use of sonographic guidance to target the portal venous system.
At the best of our knowledge, our study is the largest single-center survey on patient radiation exposure during TIPS creation. Overall, our DAP is (Reviewer 1, comment 9) below the results reported by Miller et al. [1] and below the proposed reference level [10]. In particular, our cohort of TIPS performed in an FFDS utilizing real-time sonographic guidance to target the portal venous system resulted in a mean DAP 75 % lower than the proposed reference levels. Mean FT was 66 % lower than the proposed reference levels. This data is particularly relevant since TIPS is being increasingly performed in young adults with Budd–Chiari syndrome, selected pediatric patients with complicated portal hypertension from varied etiologies, and young patients with portal hypertension who present with uncontrollable variceal bleeding during pregnancy [17–25]. Another TIPS-specific consideration is that related to occupational radiation dose reduction, given that the main operator often stands in close proximity to the patient and X-ray tube, with potential exposure to scattered radiation from the patient. The magnitude of radiation exposure to the operator is much smaller than that of the patient. However, the cumulative dose resulting in the span of a whole career might be substantial, and the consequences of this are yet to be known [26]. The use of FPDS and real-time sonographic guidance to target the portal venous system could have an important role in maintaining the eye lens organ dose of the operators below the threshold of 20 mSv/year as recently recommended [27].
Our results continue to stress the importance of targeting the portal venous system using real time ultrasound. Real-time sonographic guidance during TIPS creation has been described in four cases in 1992 by Longo et al. [2]. To date, this technique has not gained global acceptance despite it being relatively simple. This can be easily demonstrated by reviewing the methodology described in recent TIPS-related publications, with many centers still advocating the use of other techniques [3–8]. In our experience, a single operator positioned at the head of the patient can advance the Colapinto needle with the left hand while scanning the liver with the right hand (Fig. 1). In order to achieve this, the right anterolateral abdomen has to be adequately disinfected alongside with the right jugular region at the start of the procedure, and the sterile drape should include two windows. This approach is simple and inexpensive, and has been proven to further reduce radiation exposure to both patient and operator in this study.
Our results also confirm previous data reporting considerable reduction of radiation exposure in adult and pediatric populations following the introduction of FPDS [28–30]. Based on recent data, the radiation exposure originating from acquisition of angiographic runs in TIPS can be reduced by 75 % through the use of dedicated low-dose protocols in FFDS with no significant compromise on image quality and procedural outcome [31].
The data regarding the volume of ICM used during TIPS creation is also sparse. The largest study available is that published by Anderson et al. [32] reporting a mean ICM volume of 122 ± 97 ml in a total of 129 procedures. This study also concluded that the volume of ICM administered during TIPS creation was not related to the level of procedure-related renal dysfunction or to long-term renal dysfunction after TIPS creation. The overall amount of ICM in our study is in line with the results reported by Anderson et al. [32].
Based on our results and following discussion with our medical physicist, we decided to implement a local dose reference level for TIPS creation. This was set as the 75th percentile of the results obtained in Group III, that is a DAP of 150 Gy cm2 and a FT of 25 min.
The limitations of our study include the lack of accurate risk estimation for stochastic effects (including cancer and leukemia), since these should be quantified using the patient-specific Monte Carlo simulation. This was not feasible in our retrospective study, since inaccurate values would be derived (field size and possible field size variations during the procedure were not recorded). Prospective studies are therefore needed to explore this argument with more accuracy. Another limitation is that the number of punctures needed to successfully catheterize the portal system was not recorded. It was therefore not possible to conclude whether the use of real-time sonographic guidance was correlated with less punctures as compared with the use of bony landmarks.
In conclusion TIPS creation is technically challenging and radiation intensive, even when performed by experienced operators. Real-time sonographic guidance to target the portal venous system decreases radiation exposure and volume of ICM needed as compared to techniques relying on use of bony landmarks. Further reduction in radiation exposure can be achieved through the use of modern angiographic units with FPDS.
References
Miller DL, Balter S, Cole PE, et al. Radiation doses in interventional radiology procedures: the RAD-IR study: part I: overall measures of dose. J Vasc Interv Radiol. 2003;14(6):711–27.
Longo JM, Bilbao JI, Rousseau HP, et al. Color Doppler-US guidance in transjugular placement of intrahepatic portosystemic shunts. Radiology. 1992;184:281–4.
Harman JT, Reed JD, Kopecky KK, et al. Localization of the portal vein for transjugular catheterization: percutaneous placement of a metallic marker with real-time US guidance. J Vasc Interv Radiol. 1992;3:545–7.
Teitelbaum GP, Van Allan RJ, Reed RA, et al. Portal venous branch targeting with a platinum-tipped wire to facilitate transjugular intrahepatic portosystemic shunt (TIPS) procedures. Cardiovasc Intervent Radiol. 1993;16(3):198–200.
Maleux G, Nevens F, Heye S, et al. The use of carbon dioxide wedged hepatic venography to identify the portal vein: comparison with direct catheter portography with iodinated contrast medium and analysis of predictive factors influencing level of opacification. J Vasc Interv Radiol. 2006;17(11 Pt 1):1771–9.
Adamus R, Pfister M, Loose RWR. Enhancing transjugular intrahepatic portosystemic shunt puncture by using three-dimensional path planning based on the back projection of two two-dimensional portographs. Radiology. 2009;251(2):543–7.
Yamagami T, Tanaka O, Yoshimatsu R, et al. Hepatic artery guide wire targeting technique during transjugular intrahepatic portosystemic shunt. Br J Radiol. 2011;84(1000):315–8.
Chin MS, Stavas JM, Burke CT, et al. Direct puncture of the recanalized paraumbilical vein for portal vein targeting during transjugular intrahepatic portosystemic shunt procedures: assessment of technical success and safety. J Vasc Interv Radiol. 2010;21(5):671–6.
Miller DL, Kwon D, Bonavia GH. Reference levels for patient radiation doses in interventional radiology: proposed initial values for U.S. practice. Radiology. 2009;253(3):753–64.
Pinto NGV, Braz D, Vallim MA, et al. Radiation exposure in interventional radiology. Nucl Instrum Methods Phys Res A. 2007;580:586–90.
Zweers D, Geleijns J, Aarts NJM, Hardam LJ, Lameris JS, Scultz FW, Kool LJS. Patient and staff radiation dose in fluoroscopy-guided TIPS procedures and dose reduction, using dedicated fluoroscopy exposure settings. Br J Radiol. 1998;71:672–6.
Hidajat N, Wust P, Kreuschner M, et al. Radiation risks for the radiologist performing transjugular intrahepatic portosystemic shunt (TIPS). Br J Radiol. 2006;79(942):483–6.
Livingstone RS, Keshava SN. Technical note: reduction of radiation dose using ultrasound guidance during transjugular intrahepatic portosystemic shunt procedure. Indian J Radiol Imaging. 2011;21(1):13–4.
Wambersie A. International Commission on Radiological Units and Measurements. Patient dosimetry for X-rays used in medical imaging. ICRU report. J ICRU. 2005;5(2):iv–vi.
Stecker MS, Balter S, Towbin RB, et al. Guidelines for patient radiation dose management. J Vasc Interv Radiol. 2009;20(7 suppl):S263–73.
Miller DL, Balter S, Wagner LK, et al. Quality improvement guidelines for recording patient radiation dose in the medical record. J Vasc Interv Radiol. 2004;15:423–9.
Garcia-Pagan JC, Heydtmann M, Raffa S, et al. TIPS for Budd-Chiari syndrome: long-term results and prognostics factors in 124 patients. Gastroenterology. 2008;135(3):808–15.
Tripathi D, Macnicholas R, Kothari C, et al. Good clinical outcomes following transjugular intrahepatic portosystemic stent-shunts in Budd-Chiari syndrome. Aliment Pharmacol Ther. 2014;39(8):864–72.
Seijo S, Plessier A, Hoekstra J, et al. Good long-term outcome of Budd-Chiari syndrome with a step-wise management. Hepatology. 2013;57(5):1962–8.
Di Giorgio A, Agazzi R, Alberti D, et al. Feasibility and efficacy of transjugular intrahepatic portosystemic shunt (TIPS) in children. J Pediatr Gastroenterol Nutr. 2012;54(5):594–600.
Mermuys K, Maleux G, Heye S, et al. Use of the Viatorr expanded polytetrafluoroethylene-covered stent-graft for transjugular intrahepatic portosystemic shunt creation in children: initial clinical experience. Cardiovasc Intervent Radiol. 2008;31(Suppl 2):S192–6.
Vo NJ, Shivaram G, Andrews RT, et al. Midterm follow-up of transjugular intrahepatic portosystemic shunts using polytetrafluoroethylene endografts in children. J Vasc Interv Radiol. 2012;23(7):919–24.
Pillai AK, Joseph AM, Reddick M, et al. Intravascular US-guided transjugular intrahepatic portosystemic shunt creation in a second-trimester pregnancy to prophylactically decompress abdominal wall varices before cesarean section. J Vasc Interv Radiol. 2014;25(3):481–3.
Savage C, Patel J, Lepe MR, et al. Transjugular intrahepatic portosystemic shunt creation for recurrent gastrointestinal bleeding during pregnancy. J Vasc Interv Radiol. 2007;18(7):902–4.
Ingraham CR, Padia SA, Johnson GE, et al. Transjugular intrahepatic portosystemic shunt placement during pregnancy: a case series of five patients. Cardiovasc Intervent Radiol. 2015. doi:10.1007/s00270-015-1053-z.
Kim KP, Miller DL, Berrington de Gonzalez A, et al. Occupational radiation doses to operators performing fluoroscopically-guided procedures. Health Phys. 2012;103(1):80–99.
International Commission on Radiological Protection. ICRP statement on tissue reactions and early and late effects of radiation in normal tissues and organs—threshold doses for tissue reactions in a radiation protection context. ICRP Publication 118. Oxford: Elsevier; 2012. Ann. ICRP 41(1–2).
Suzuki S, Furui S, Kobayashi I, et al. Radiation dose to patients and radiologists during transcatheter arterial embolization: comparison of a digital flat-panel system and conventional unit. Am J Roentgenol. 2005;185(4):855–9.
Miraglia R, Maruzzelli L, Tuzzolino F, et al. Radiation exposure in biliary procedures performed to manage anastomotic strictures in pediatric liver transplant recipients: comparison between radiation exposure levels using an image intensifier and a flat-panel detector-based system. Cardiovasc Intervent Radiol. 2013;36(6):1670–6.
Miraglia R, Maruzzelli L, Cortis K, et al. Comparison between radiation exposure levels using an image intensifier and a flat-panel detector-based system in image-guided central venous catheter placement in children weighing less than 10 kg. Pediatr Radiol. 2015;45(2):235–40.
Miraglia R, Maruzzelli L, Cortis K, et al. Digital subtraction angiography during transjugular intrahepatic portosystemic shunt creation or revision: data on radiation exposure and image quality obtained using a standard and a low-dose acquisition protocol in a flat-panel detector-based system. Abdom Imaging. 2014. doi:10.1007/s00261-014-0313-8.
Anderson CL, Saad WE, Kalagher SD, et al. Effect of transjugular intrahepatic portosystemic shunt placement on renal function: a 7-year, single-center experience. J Vasc Interv Radiol. 2010;21(9):1370–6.
Conflict of interest
Roberto Miraglia, Luigi Maruzzelli, Kelvin Cortis, Mario D’Amico, Gaetano Floridia, Giuseppe Gallo, Corrado Tafaro, and Angelo Luca declares that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Miraglia, R., Maruzzelli, L., Cortis, K. et al. Radiation Exposure in Transjugular Intrahepatic Portosystemic Shunt Creation. Cardiovasc Intervent Radiol 39, 210–217 (2016). https://doi.org/10.1007/s00270-015-1164-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-015-1164-6