
Abstract
Background
Laparoscopic gastrectomy (LG) is now practiced widely, but it is unclear whether LG is the appropriate approach for elderly patients with resectable advanced gastric cancer. The aim of this study was to examine whether LG is more or less advantageous for elderly patients than for young patients.
Methods
We collected data on 571 consecutive patients who underwent gastrectomy for pT2–4 gastric cancer between January 2001 and December 2015. After adjustment with one-to-one propensity score matching, short-term and long-term outcomes were compared between the LG and open gastrectomy (OG) groups among young (age < 70 years) and elderly (age ≥ 70 years) patients.
Results
The LG group had a significantly longer operative time (P < 0.001) and less blood loss (P < 0.001) than the OG group among young and elderly patients. There were no significant differences regarding complications. Although disease-specific survival was similar between the LG and OG groups among young and elderly patients, LG was associated with more favorable overall survival than OG only among elderly patients (hazard ratio 0.67; 95% confidence interval 0.35–1.26). Death from respiratory diseases occurred more frequently in the OG group (10.9%) than in the LG group (0%) for elderly patients (P = 0.012).
Conclusion
LG for resectable advanced gastric cancer was not inferior to OG in terms of both short-term and long-term outcomes regardless of patient age. In elderly patients, LG may improve overall survival by reducing mortality from respiratory diseases.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gastric cancer is the fifth most common malignancy in the world and the second leading cause of death among all malignancies worldwide [1]. Radical open gastrectomy (OG) is the curative treatment for gastric cancer [2]. Gastrectomy without complications leads to good long-term prognosis [3]. Over the last few decades, the aging population has affected healthcare provision, including surgical treatments [4, 5]. Aging has progressed most prominently in developed countries; in Japan, 21.4% of the population is aged 70 years or older [6]. Several studies have reported that aggressive surgical treatment has led to longer survival in elderly patients with gastric cancer [7,8,9]. As society ages, the number of surgical treatments for gastric cancer in elderly patients will increase.
Laparoscopic gastrectomy (LG) has been widely used in Japan since 1991 to treat gastric cancer [10]. The usefulness of LG has already been demonstrated for early gastric cancer with sufficient evidence [11,12,13,14,15,16,17,18]. Several randomized controlled trials (RCTs) comparing LG with OG for advanced gastric cancer are in progress, and its safety and feasibility have almost been established [19,20,21]. However, these trials excluded elderly patients from the eligibility criteria. Thus, the usefulness of LG for elderly patients remains unclear.
In our institution, we have been actively performing LG for gastric cancer since 2001. We have reported many surgical techniques and innovations [22,23,24,25,26,27,28]. Furthermore, we have also expanded the indications of LG for advanced gastric cancer without age limitations. Considering the recent rapidly aging community, it is necessary to evaluate the safety and efficacy of LG in elderly patients. We hypothesized that LG is more suitable than OG for elderly patients because it is less invasive. Thus, we conducted a propensity score matching (PSM) analysis to examine whether LG is more or less advantageous for elderly patients than for young patients with resectable advanced gastric cancer.
Patients and methods
Patients
We collected data on 571 consecutive patients who underwent gastrectomy for pT2–4 gastric cancer between January 2001 and December 2015 at Osaka University Hospital. Patients who underwent partial, R1, or R2 resection and patients who had remnant gastric cancer or atypical histology were ineligible. Patients who cannot tolerate general anesthesia due to severe comorbidities were excluded from the study. All patients were histologically diagnosed as having gastric adenocarcinoma. In general, patients underwent LG or OG with lymph node dissection according to the Japanese Gastric Cancer Treatment Guidelines [29]. LG was performed or supervised by surgeons who were certified by the Japan Society for Endoscopic Surgery according to the Endoscopic Surgical Skill Qualification System. Postoperative complications were evaluated based on the Clavien–Dindo classification [30]; we considered complications of grade II or higher to be postoperative complications in this study. TNM staging was determined on the basis of the 14th edition of the Japanese Classification of Gastric Carcinoma [31]. This study was approved by the Institutional Review Board of Osaka University Hospital (Approval number: 19201).
Statistical analysis
One-to-one PSM was used to reduce sampling bias and potential confounding factors by matching patients in the LG and OG groups. PSM analysis was conducted using a logistic regression model with the following covariates: age, sex, body mass index (BMI), American Society of Anesthesiologists physical status classification (ASA-PS), surgical procedure, histology, main tumor location, macroscopic type, tumor size, presence or absence of neoadjuvant chemotherapy, and pathological TNM stage. We used a caliper width of 0.2 for the pooled standard deviation of the logit for calculating the propensity score. After PSM, we divided the patients into two populations: elderly patients, consisting of patients aged 70 years or more, and young patients under 70 years.
Overall survival (OS) was defined as the period from the date of surgery to the date of death from any cause. Disease-specific survival (DSS) was defined as the period from the date of surgery to the date of death due to primary disease. Survival was estimated using the Kaplan–Meier method and compared using the log-rank test. We compared the clinicopathological characteristics of the LG and OG groups using the Chi-squared test for categorical variables and the Mann–Whitney U test for continuous variables. P < 0.05 was considered to indicate a statistically significant difference. All statistical analyses were performed using JMP® PRO software (JMP version 14.1.0, SAS Institute, Cary, NC).
Results
Patient characteristics
The study flowchart is summarized in Fig. 1. After 188 patients in the LG group and 383 patients in the OG group underwent PSM, 137 pairs of patients were analyzed. Of 274 patients, 172 patients (62.8%) were young (age < 70 years) patients and 102 (37.2%) were elderly (age ≥ 70 years) patients. Total gastrectomy was performed for 44.2% of young patients and 30.4% of elderly patients. The proportions of pathological stage I, II, and III disease were 19.2%, 49.4%, and 31.4%, respectively, for young patients and 15.7%, 52.9%, and 31.4%, respectively, for elderly patients. Adjuvant chemotherapy was performed in 53.5% of young patients and 32.4% of elderly patients. The differences in clinicopathological characteristics between the LG and OG groups are summarized in Table 1. No significant differences were observed between the two groups in any factors between young and elderly patients.

Study flowchart
Short-term outcomes
Comparisons of short-term outcomes between the young and elderly patients are summarized in Table 2. The LG group had a significantly longer operative time (P < 0.001) and less blood loss (P < 0.001) than the OG group among both young and elderly patients. The number of retrieved lymph nodes did not differ significantly between the LG and OG groups among young (P = 0.19) and elderly patients (P = 0.43).
Regarding surgical complications, the overall incidence of Clavien–Dindo grade II–IV surgical complications did not differ significantly among young (LG, 16.1%; OG, 22.0%; P = 0.32) and elderly patients (LG, 19.6%; OG, 30.4%; P = 0.21). There was no significant difference for each complication between the LG and OG groups among young and elderly patients. No in-hospital mortality or 30-day mortality occurred in either group.
Long-term outcomes
At the median follow-up duration of 63.2 months for all censored patients, we estimated DSS and OS. In the DSS analysis (Fig. 2), the LG and OG groups had similar survival curves among young (hazard ratio [HR] 1.02; 95% confidence interval [CI] 0.52–2.02; log-rank P = 0.95) and elderly patients (HR 1.00; 95% CI 0.41–2.42; log-rank P = 1.00). In the OS analysis (Fig. 3), LG showed a nonsignificant difference, but a trend toward improved survival compared with OG (HR 0.67; 95% CI 0.35–1.26; log-rank P = 0.21) among elderly patients, although the LG and OG groups had similar survival curves among young patients (HR 0.88; 95% CI 0.47–1.67; log-rank P = 0.70).

Disease-specific survival curves of the laparoscopic gastrectomy (LG) and open gastrectomy (OG) groups for young patients (< 70 years) (a) and elderly patients (≥ 70 years) (b)

Overall survival curves of the laparoscopic gastrectomy (LG) and open gastrectomy (OG) groups for young patients (< 70 years) (a) and elderly patients (≥ 70 years) (b)
Regarding the cause of death, the proportions of death from primary cancer were very similar between the LG and OG groups among young (LG 19.8%; OG18.6%; P = 0.86) and elderly patients (LG 19.6%; OG 19.6%; P = 0.99) (Table 3). On the other hand, elderly patients in the OG group had a nonsignificant difference but a trend toward a higher proportion of death from other diseases (LG 10.7%; OG 28.3%; P = 0.14). In particular, death from respiratory diseases occurred more frequently in the OG group than in the LG group among elderly patients (LG 0%; OG 10.9%; P = 0.012), although no young patients died due to respiratory diseases in either group. A total of nine patients died of secondary cancers diagnosed during the postoperative follow-up period.
Discussion
In this PSM study, we confirmed LG required significantly longer operative time, but there was less blood loss than OG among both young and elderly patients. In addition, there were no statistically significant differences regarding complications. Among long-term outcomes, DSS was quite similar between the LG and OG groups among both young and elderly patients. However, LG was associated with more favorable OS than OG among elderly patients only. This is probably because elderly patients who underwent LG were less likely to die from other diseases, such as respiratory diseases, than elderly patients who underwent OG.
Many studies have demonstrated the benefits of LG, which include improved cosmetic effect, less pain, quicker recovery, shorter hospital stay, and better quality of life [13, 32,33,34,35]. Recent retrospective studies have also suggested the non-inferiority of LG compared with OG in terms of long-term outcomes [36,37,38]. Three large-scale RCTs comparing LG and OG have been conducted for advanced gastric cancer; short-term outcomes have already been reported to be satisfactory in these studies [19,20,21]. For long-term prognosis, one of the three studies recently showed the non-inferiority of LG [39], although two of the three studies are still ongoing. Of these three RCTs, inclusion criteria included age up to 80 years for two studies and up to 75 years for one study. Thus, many elderly patients with gastric cancer were excluded from these studies. There have been few studies comparing LG and OG in patients with advanced gastric cancer after stratification for age. In this study, we examined how LG and OG affect prognosis after stratification into young and elderly patients with advanced gastric cancer.
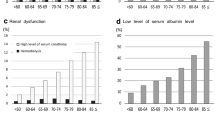
Elderly patients often have more comorbidities such as hypertension and diabetes than young patients [40]. We reported that elderly patients have significantly lower preoperative serum albumin levels and higher ASA-PS scores than young patients [41]. These high-risk conditions are probably responsible for some nonsurgical complications after gastrectomy in elderly patients. Gastrectomy for the elderly is associated with a higher incidence of postoperative pneumonia, which is directly linked to mortality [42, 43]. We also reported that a low preoperative prognostic nutrition index and multiple comorbidities are significant risk factors for death from other diseases within 5 years in elderly patients [44]. Kiuchi et al. [45] reported that postoperative pneumonia is less common after LG (0.9%) versus OG (2.6%). Indeed, there was the possibility that patients with severe respiratory or cardiac comorbidities tended to receive OG. However, as laparoscopic surgery has the advantage of causing less abdominal wall injury, LG may lead to fewer postoperative respiratory complications in elderly patients. This advantage of LG could lead to lower mortality from respiratory diseases during long-term follow-up as well.
There are several limitations in this study. First, this study is a retrospective study and includes several sources of selection bias. In order to reduce these biases, PSM was performed. Background factors were well balanced after PSM. In general, OG tends to be selected for more advanced cases, but our selection process usually depends on ongoing clinical trials rather than tumor status. Second, there is still no consensus on the age cutoff between young and elderly patients. Frailty is especially important in cancer treatment [46]. We used 70 years as the age cutoff in this study because it is usually recommended that all elderly patients aged over 70 years be routinely assessed for frailty [47]. It may be necessary to examine to use a higher age cutoff in the near future, considering the speed of aging in society. Third, due to the long study period, the historical background is somewhat different. For example, the ACTS-GC trial demonstrated the survival benefit of postoperative S-1 in 2007 [48]. Later, adjuvant S-1 chemotherapy was determined to be the standard treatment for pStage II–III gastric cancer. Thus, the change in standard treatment over time may have influenced differences in prognosis for LG versus OG.
In conclusion, LG for resectable advanced gastric cancer is not inferior to OG in terms of short-term and long-term outcomes. However, in elderly patients, LG may improve OS by reducing mortality from other diseases due to its lower invasiveness. Thus, the advantage of LG would be higher for elderly patients than for young patients with advanced gastric cancer. If the ongoing RCTs demonstrate the non-inferiority of LG versus OG for relatively young patients with advanced gastric cancer, the results can be generalized to elderly patients.
References
International Agency for Research on Cancer: Cancer Today: Population fact sheets. http://gco.iarc.fr/today/data/factsheets/populations/900-world-fact-sheets.pdf. Accessed 29 Mar 2020
Kurokawa Y, Doki Y, Mizusawa J et al (2018) Bursectomy versus omentectomy alone for resectable gastric cancer (JCOG1001): a phase 3, open-label, randomised controlled trial. Lancet Gastroenterol Hepatol 3:460–468
Saito T, Kurokawa Y, Miyazaki Y et al (2015) Which is a more reliable indicator of survival after gastric cancer surgery: Postoperative complication occurrence or C-reactive protein elevation? J Surg Oncol 112:894–899
Partridge JS, Harari D, Dhesi JK (2012) Frailty in the older surgical patient: a review. Age Ageing 41:142–147
Soreide K, Wijnhoven BP (2016) Surgery for an ageing population. Br J Surg 103:e7–9
Statistics Bureau, Ministry of Internal Affairs and Communications. Result of the population estimates: monthly report; March 1, 2019 (final estimates). https://www.stat.go.jp/english/data/jinsui/tsuki/index.html
Endo S, Shimizu Y, Ikenaga M et al (2017) Survival benefit of gastrectomy for gastric cancer in patients ≥ 85 years old: a retrospective propensity score-matched analysis. Surgery 161:984–994
Kusano C, Iwasaki M, Kaltenbach T et al (2011) Should elderly patients undergo additional surgery after non-curative endoscopic resection for early gastric cancer? Long-term comparative outcomes. Am J Gastroenterol 106:1064–1069
Lim JH, Lee DH, Shin CM et al (2014) Clinicopathological features and surgical safety of gastric cancer in elderly patients. J Korean Med Sci 29:1639–1645
Kitano S, Iso Y, Moriyama M et al (1994) Laparoscopy-assisted Billroth I gastrectomy. Surg Laparosc Endosc 4:146–148
Hiki N, Katai H, Mizusawa J et al (2018) Long-term outcomes of laparoscopy-assisted distal gastrectomy with suprapancreatic nodal dissection for clinical stage I gastric cancer: a multicenter phase II trial (JCOG0703). Gastric Cancer 21:155–161
Honda M, Hiki N, Kinoshita T et al (2016) Long-term outcomes of laparoscopic versus open surgery for clinical stage I gastric cancer: the LOC-1 study. Ann Surg 264:214–222
Katai H, Mizusawa J, Katayama H et al (2017) Short-term surgical outcomes from a phase III study of laparoscopy-assisted versus open distal gastrectomy with nodal dissection for clinical stage IA/IB gastric cancer: Japan Clinical Oncology Group Study JCOG0912. Gastric Cancer 20:699–708
Katai H, Sasako M, Fukuda H et al (2010) Safety and feasibility of laparoscopy-assisted distal gastrectomy with suprapancreatic nodal dissection for clinical stage I gastric cancer: a multicenter phase II trial (JCOG 0703). Gastric Cancer 13:238–244
Kim HH, Han SU, Kim MC et al (2014) Long-term results of laparoscopic gastrectomy for gastric cancer: a large-scale case-control and case-matched Korean multicenter study. J Clin Oncol 32:627–633
Kim W, Kim HH, Han SU et al (2016) Decreased morbidity of laparoscopic distal gastrectomy compared with open distal gastrectomy for stage I gastric cancer: short-term outcomes from a multicenter randomized controlled trial (KLASS-01). Ann Surg 263:28–35
Kurokawa Y, Katai H, Fukuda H et al (2008) Phase II study of laparoscopy-assisted distal gastrectomy with nodal dissection for clinical stage I gastric cancer: Japan Clinical Oncology Group Study JCOG0703. Jpn J Clin Oncol 38:501–503
Nakamura K, Katai H, Mizusawa J et al (2013) A phase III study of laparoscopy-assisted versus open distal gastrectomy with nodal dissection for clinical stage IA/IB gastric cancer (JCOG0912). Jpn J Clin Oncol 43:324–327
Hu Y, Huang C, Sun Y et al (2016) Morbidity and mortality of laparoscopic versus open D2 distal gastrectomy for advanced gastric cancer: a randomized controlled trial. J Clin Oncol 34:1350–1357
Lee HJ, Hyung WJ, Yang HK et al (2016) Morbidity of laparoscopic distal gastrectomy with D2 lymphadenectomy compared with open distal gastrectomy for locally advanced gastric cancer: short term outcomes from multicenter randomized controlled trial (KLASS-02). Proc Am Soc Clin Oncol 34(suppl):4062 (abstr)
Lee SW, Etoh T, Ohyama T et al (2017) Short-term outcomes from a multi-institutional, phase III study of laparoscopic versus open distal gastrectomy with D2 lymph node dissection for locally advanced gastric cancer (JLSSG0901). Proc Am Soc Clin Oncol 35(suppl):4029 (abstr)
Furukawa H, Kurokawa Y, Takiguchi S et al (2018) Short-term outcomes and nutritional status after laparoscopic subtotal gastrectomy with a very small remnant stomach for cStage I proximal gastric carcinoma. Gastric Cancer 21:500–507
Takiguchi S, Fujiwara Y, Yamasaki M et al (2015) Laparoscopic intraoperative navigation surgery for gastric cancer using real-time rendered 3D CT images. Surg Today 45:618–624
Takiguchi S, Fujiwara Y, Yamasaki M et al (2013) Laparoscopy-assisted distal gastrectomy versus open distal gastrectomy. A prospective randomized single-blind study. World J Surg 37:2379–2386. https://doi.org/10.1007/s00268-013-2121-7
Takiguchi S, Hiura Y, Takahashi T et al (2013) Preservation of the celiac branch of the vagus nerve during laparoscopy-assisted distal gastrectomy: impact on postprandial changes in ghrelin secretion. World J Surg 37:2172–2179. https://doi.org/10.1007/s00268-013-2078-6
Wada N, Kurokawa Y, Takiguchi S et al (2014) Feasibility of laparoscopy-assisted total gastrectomy in patients with clinical stage I gastric cancer. Gastric Cancer 17:137–140
Takiguchi S, Sekimoto M, Miyake Y et al (2003) Totally laparoscopic distal gastrectomy using the hand-sewn Billroth-I anastomotic technique: report of a case. Surg Today 33:371–374
Takiguchi S, Sekimoto M, Fujiwara Y et al (2004) Laparoscopic lymph node dissection for gastric cancer with intraoperative navigation using three-dimensional angio computed tomography images reconstructed as laparoscopic view. Surg Endosc 18:106–110
Japanese Gastric Cancer Association (2014) Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer 20:1–19
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Japanese Gastric Cancer A (2011) Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer 14:101–112
Huscher CG, Mingoli A, Sgarzini G et al (2005) Laparoscopic versus open subtotal gastrectomy for distal gastric cancer: five-year results of a randomized prospective trial. Ann Surg 241:232–237
Kim MG, Yook JH, Kim KC et al (2011) Influence of obesity on early surgical outcomes of laparoscopic-assisted gastrectomy in gastric cancer. Surg Laparosc Endosc Percutan Tech 21:151–154
Lee SI, Choi YS, Park DJ et al (2006) Comparative study of laparoscopy-assisted distal gastrectomy and open distal gastrectomy. J Am College Surg 202:874–880
Ohtani H, Tamamori Y, Noguchi K et al (2010) A meta-analysis of randomized controlled trials that compared laparoscopy-assisted and open distal gastrectomy for early gastric cancer. J Gastrointest Surg 14:958–964
Kinoshita T, Uyama I, Terashima M et al (2019) Long-term outcomes of laparoscopic versus open surgery for clinical stage II/III gastric cancer: a multicenter cohort study in Japan (LOC-A Study). Ann Surg 269:887–894
Li Z, Li B, Bai B et al (2018) Long-term outcomes of laparoscopic versus open D2 gastrectomy for advanced gastric cancer. Surg Oncol 27:441–448
Xu Y, Hua J, Li J et al (2019) Long-term outcomes of laparoscopic versus open gastrectomy for advanced gastric cancer: a large cohort study. Am J Surg 217:750–756
Yu J, Huang C, Sun Y et al (2019) Effect of laparoscopic vs open distal gastrectomy on 3-year disease-free survival in patients with locally advanced gastric cancer: the CLASS-01 randomized clinical trial. JAMA 321:1983–1992
Centers for Disease Control and Prevention (2003) From the Centers for Disease Control and Prevention. Public health and aging: trends in aging–United States and worldwide. JAMA 289:1371–1373
Mikami J, Kurokawa Y, Miyazaki Y et al (2015) Postoperative gastrectomy outcomes in octogenarians with gastric cancer. Surg Today 45:1134–1138
Yamada H, Shinohara T, Takeshita M et al (2013) Postoperative complications in the oldest old gastric cancer patients. Int J Surg 11:467–471
Takeuchi D, Koide N, Suzuki A et al (2015) Postoperative complications in elderly patients with gastric cancer. J Surg Res 198:317–326
Hashimoto T, Kurokawa Y, Mikami J et al (2019) Postoperative long-term outcomes in elderly patients with gastric cancer and risk factors for death from other diseases. World J Surg. https://doi.org/10.1007/s00268-019-05109-5(in press)
Kiuchi J, Komatsu S, Ichikawa D et al (2016) Putative risk factors for postoperative pneumonia which affects poor prognosis in patients with gastric cancer. Int J Clin Oncol 21:920–926
Ethun CG, Bilen MA, Jani AB et al (2017) Frailty and cancer: Implications for oncology surgery, medical oncology, and radiation oncology. CA Cancer J Clin 67:362–377
Morley JE, Vellas B, van Kan GA et al (2013) Frailty consensus: a call to action. J Am Med Dir Assoc 14:392–397
Sakuramoto S, Sasako M, Yamaguchi T et al (2007) Adjuvant chemotherapy for gastric cancer with S-1, an oral fluoropyrimidine. N Engl J Med 357:1810–1820
Acknowledgements
The authors had no financial support for the research reported.
Funding
None
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There is no conflict of interest regarding the manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ushimaru, Y., Kurokawa, Y., Takahashi, T. et al. Is Laparoscopic Gastrectomy More Advantageous for Elderly Patients Than for Young Patients with Resectable Advanced Gastric Cancer?. World J Surg 44, 2332–2339 (2020). https://doi.org/10.1007/s00268-020-05486-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-020-05486-2