
Abstract
Background
Single-incision laparoscopy (SIL) and natural orifice translumenal endoscopic surgery (NOTES) aim at reducing surgical access trauma. To monitor the introduction of emerging technologies, the Swiss Association for Laparo- and Thoracoscopic Surgeons launched a database in 2010. The current status of SIL and NOTES in Switzerland is reported, and the techniques are compared.
Methods
The number and type of procedures, surgeon experience, their impressions of performance, conversion, and complications between 2010 and 2015 are described. A survey was used to acquire additional data not included in the registry.
Results
Nine centers included 650 procedures. Cholecystectomy (55 %) and sigmoidectomy (26 %) were most prevalent in both techniques. The number of active centers declined from 9 to 2 during the study period. The frequencies of taught procedures were 4 and 43 % for SIL and NOTES (p < 0.001), and surgeon self-estimated impression of performance was perfect in 50 and 89 %, respectively (p < 0.0001). Conversions in total were 3.6 and 5.7 %, respectively, and 1.1 % to open for both techniques. Morbidity was 5 % in SIL and 2.7 % in NOTES, with 0.8 % access-related complications in NOTES and none in SIL (p = 0.29). Of laparoscopic cholecystectomy, sigmoidectomy, and right hemicolectomy, 11.4 and 15.6 % of cases were operated using SIL or NOTES, respectively (p < 0.0001).
Conclusions
Although in selected specialized centers, a considerable proportion of patients were treated using novel techniques, a fading interest of the surgical community in SIL and NOTES was observed. The proportion of SIL and NOTES procedures taught is insufficient and calls for improvement.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In the last decades, two new techniques have emerged that aimed at reducing surgical access trauma in laparoscopy. Single-incision laparoscopy (SIL) reduces the number of abdominal trocars to only one, with the incision usually hidden in the navel. In natural orifice translumenal endoscopic surgery (NOTES), the abdominal cavity is reached through a body orifice, such as the vagina, anus, or mouth, thus avoiding trauma to the abdominal wall. However, in clinical practice, NOTES is almost always used in a hybrid technique combining natural orifice access with small abdominal trocars. The purpose of both SIL and hybrid NOTES is to reduce postoperative pain [1–3], enhance recovery, and avoid visible scars [4, 5].
NOTES was first reported for transgastric peritoneoscopy in 2000 [6] but has gained broader attention only with reports of transvaginal cholecystectomy in 2007 [7, 8]. Also in 2007, after initial attempts in the 1990s, SIL became accepted with the availability of commercial platforms [9]. Scientific reports on both techniques are rapidly increasing [10]. However, little is known about the current dissemination of SIL and NOTES in routine clinical practice.
One of the most striking evolutions in abdominal surgery in the last century was the introduction of laparoscopy, which rapidly replaced open surgery for many routine procedures. After the widespread introduction of laparoscopic cholecystectomy, the biliary duct injury rate increased. Biliary complications are particularly frequent in the first 10 laparoscopic cases each surgeon performs [11]. For more advanced procedures, the learning curve is even more challenging, and the need for intensive laparoscopic training interferes with the widespread adoption of laparoscopic surgery. In a recent survey in Austria, the proportion of laparoscopy in colorectal surgery was as low as 26 % [12]. In addition, SIL and hybrid NOTES further increase the requirement of high-level laparoscopic skills. Mastering SIL cholecystectomy safely requires at least 20 procedures under supervision [13, 14]. A significant learning curve, especially for advanced colorectal procedures [15, 16], must be considered. In the course of implementation of new surgical techniques, complications inevitably may occur during the learning curve [17]. Therefore, pioneers of scarless surgery joined together to form working groups such as the Natural Orifice Surgery Consortium for Assessment and Research (NOSCAR) [18], the Euro-NOTES Group [19], and the D-NOTES in Germany [20]. These groups aim to ensure adequate surgical training and standards for a safe transfer of SIL and hybrid NOTES from the bench to the operating room [18].
In Switzerland, the Swiss Association for Laparo- and Thoracoscopic Surgeons (called SALTS) designed the D-SENT database on emerging surgical technologies in 2010. The aim of the current study is to describe the use of SIL and hybrid NOTES in Switzerland. Because D-SENT includes both techniques, the database also offers the unique opportunity to compare the two.
Materials and methods
Entries in the prospective, voluntary database D-SENT between August 17, 2010, and August 24, 2015, were analyzed. The number of recruiting centers and their number of included patients are described. The study period was divided into five equal time portions. The type and frequency of procedures are described. It was analyzed whether consultants, fellows that were board certified in general surgery, or residents performed the procedures. Surgery performed by fellows or residents and supervised by senior laparoscopic surgeons was considered as a teaching procedure. The level of experience in SIL, NOTES, and corresponding conventional laparoscopic technique was assessed, and surgeon impression of the procedures was compared for SIL and hybrid NOTES.
Characteristics of procedures and patients including age, body mass index, duration of surgery, and length of hospital stay for the three most common SIL and hybrid NOTES procedures were compared. The type of NOTES routes applied for which procedures also was assessed.
The rates and reasons for conversions to either conventional laparoscopy or open surgery for SIL and hybrid NOTES were determined. Access-related and overall intra- and postoperative complications were analyzed in both groups and compared, with postoperative complications graded according to the Clavien–Dindo classification [21].
In addition, an Internet-based survey (SurveyMonkey., California) was administered to the responsible persons at each center. To depict the proportion of procedures performed in novel technique, the responsible persons were asked to provide statistics for the different time periods with the total number of patients undergoing SIL, hybrid NOTES, or conventional laparoscopy for the three most common procedures, as determined in the analysis of the registry.
Data collection and statistics
Patient characteristics, indication, and procedure details were prospectively collected in a database (Excel, Microsoft, Washington). Descriptive statistics and analysis of significant differences were performed using GraphPad® Prism version 5.00 (GraphPad Software, California). Continuous data were expressed as mean ± standard deviation or median and range, as indicated. Proportions between groups were compared using a two-tailed Mann–Whitney test assuming a nonparametric distribution. Categorical variables were compared using a two-sided Chi-square test. Linear trend was tested by multiple comparisons between means and column order in one-way ANOVA. The level of significance was set at 0.05.
Results
Registry data
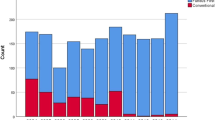
The registry included 676 entries in the study period, 650 of which were valid and eligible for analysis. Nine surgical departments in Switzerland included a median 9 (1–429) patients in the registry. Five centers included exclusively SIL, one center only hybrid NOTES, and three centers both techniques. More specifically, eight centers entered a median of 6 (1–73) patients for SIL and 4 centers a median of 38 (7–428) patients for the hybrid NOTES technique. The number of centers including SIL in the registry declined from eight at the beginning to only one at the end of the study period. After 2012, there was a statistical insignificant decline in the number of included SIL patients (p = 0.223; Fig. 1). The number of centers including NOTES procedures in the registry declined from initially four to only one at the end of the study period. After 2012, there was a statistically insignificant decline in the number of included hybrid NOTES procedures (p = 0.628; Fig. 2).

Single-incision laparoscopy (SIL) procedures per time period

Natural orifice translumenal endoscopic surgery (NOTES) procedures per time period
Cholecystectomy and sigmoidectomy were the most frequent procedures, accounting for 77 % of SIL and 83 % of NOTES. In SIL and NOTES, 11 and 10 different procedures were performed, respectively (Table 1).
Consultants performed the vast majority (89 %) and fellows only 11 % of SIL procedures. Residents performed none. The proportions of patients treated by consultants, fellows, or residents with hybrid NOTES were 42, 50, and 8 %. The frequencies of teaching procedures in SIL and hybrid NOTES were 4 and 43 % (p < 0.0001). Figure 3 shows the level of experience of SIL and hybrid NOTES surgeons with the novel technique and with the corresponding procedure in conventional laparoscopy. Although the experience with the novel technique was statistically not different (p = 0.06), surgeons with experience with more than 50 procedures in the corresponding laparoscopic technique were predominant in the SIL group (p = 0.0092). Surgeon impressions were that performance of the procedure was perfect in 50 % of SIL and 89 % of hybrid NOTES procedures, good in 9 and 44 %, and sufficient in 6 and 2 %, respectively (p < 0.0001).

Level of experience of single-incision surgeons with single-incision procedures (a) and the corresponding conventional laparoscopic technique (b) and of natural orifice translumenal endoscopic surgery (NOTES) surgeons with NOTES (c) and the corresponding conventional laparoscopic technique (d)
The three procedures being offered in most centers for both techniques were cholecystectomy, sigmoidectomy, and right hemicolectomy. Characteristics for these indicator procedures are depicted in Table 2.
It bears mentioning that in all included NOTES procedures rigid instruments were used and small sized abdominal trocars were added. The procedures are therefore considered hybrid NOTES. The preferred NOTES route was transvaginal in 89 %, followed by transrectal in 11 %, and transgastric in 0.2 %. Through the transvaginal route, cholecystectomy, colectomy, adnexectomy, hysterectomy, and left pancreatectomy were performed. In none of the surgical cases was a gynecologist involved to help with the access. The transrectal route was used for sigmoidectomy and anterior resection, and the transgastric route for intragastric resection of GIST.
In SIL, conversion rates were 2.1 % (3) to laparoscopy and 1.4 % (2) to open surgery. The reason for conversion was insufficient exposure in all cases. With NOTES, 4.7 % (24) involved conversions to conventional laparoscopy and 1 % (5) to open surgery. However, it was not noted in the register whether the conversion was decided on before or after attempted NOTES access. The reasons for conversion to laparoscopy were insufficient exposure (11), adhesions in the pelvis disabling NOTES access (4), specimen too large to remove over transrectal access (7), polyp in the cervix uteri (1), and one intraoperative injury to the Riolan arcade in transvaginal sigmoidectomy. The five conversions to open surgery were due to the need for additional adnexectomy for tubo-ovarian abscess, very large uterine myomas in transvaginal laparoscopic hysterectomy, malrotation in a sigmoidectomy patient, interenteric fistula in a case of sigmoid diverticulitis, and severe adhesions in one case.
Access-related intraoperative complications occurred in 0.6 % (3) of transvaginal NOTES: one perforation of the uterus by means of the uterus manipulator; one injury to the bladder, necessitating an overstitch; and the aforementioned injury to the Riolan arcade. There was no intraoperative complication in SIL.
The overall postoperative complication rate was 3.2 %: 5 % (7) in SIL and 2.7 % (14) in hybrid NOTES (p = 0.19). The complications are listed in Table 3. The reoperation rate of 1.4 % was equal in both groups. Among the complications in the hybrid NOTES group, there was one bleeding at the colpotomy site with a need to overstitch by colposcopy, clearly related to the transvaginal access. Including the intraoperative complications, there were 0.8 % access-related complications in NOTES, whereas there were no obvious access-related complications in SIL (p = 0.29).
Survey data
On the survey, five centers, of which two performed SIL, one hybrid NOTES and two both techniques, provided their total number of SIL, hybrid NOTES, or conventional laparoscopic cholecystectomy, sigmoidectomy, and right hemicolectomy.
For trend analysis, four centers performing a total of 951 SIL out of 8360 laparoscopic procedures, and three centers performing 898 hybrid NOTES out of 5747 laparoscopic procedures were included. Per 12-month period, a median of 278 (106–285) underwent SIL and 195 (178–214) hybrid NOTES. The study term was divided into two periods to compare the proportion of procedures performed with a novel technique among all corresponding laparoscopic procedures. In the centers that responded to the survey, the proportion of SIL increased from 11 % in the first time period (09/2010–08/2013) to 13 % in the second period (09/2013–08/2015) (p = 0.0035). On the other hand, the proportion of hybrid NOTES decreased from 17 to 14 % (p = 0.0366). However, in total, the proportion of patients being operated with a novel technique in centers performing hybrid NOTES was higher than for SIL (p < 0.0001). In Table 4, the proportions of SIL or hybrid NOTES compared to the respective laparoscopic procedure are shown.
Discussion
Although as many as 16 different procedures were included in the registry, the vast majority of the 140 SIL and 510 hybrid NOTES records concern cholecystectomy and colorectal surgery. Cholecystectomy, representing 55 % of all procedures, was less predominant than in the German NOTES registry where this intervention accounted for 88 % of all entries. Hence, colorectal surgery was much more represented in D-SENT compared to the German registry with 35 and 31 % for SIL and hybrid NOTES, respectively, compared to 5.2 %. A few centers included a high number of patients for novel technologies. In one center, up to 67 % of cholecystectomies were performed with the SIL technique. In a few specialized centers, SIL and hybrid NOTES seemed to be not only a cutting-edge method for highly selected patients but also an important new approach for routine clinical use.
Very similar to the German registry, patients for cholecystectomy and sigmoidectomy were relatively young and non-obese, indicating a selection of low-risk patients. Patients who underwent SIL sigmoidectomy were significantly younger than for hybrid NOTES, with an average age of 54.2 years. Here, surgeons were reluctant to offer SIL sigmoidectomy to either elderly patients or, possibly, younger patients particularly requested SIL.
The access-related complication rate in SIL and hybrid NOTES was not different; however, 0.8 % of transvaginal NOTES involved access-related complications, which is similar to the German registry with 0.7 % of such access-related complications reported, including bladder, uterus, and bowel injuries and vaginal bleeding. In SIL, no access-related complications were reported, but wound infections occurred in 2.1 %, which corresponds to the wound complication rate reported before for SIL [22]. It has been proposed that the wound complication rate decreases after a SIL learning curve of 500 procedures. The rate of overall complications was nevertheless not different for SIL and NOTES (5 and 3.3 %).
The overall conversion rate in SIL with 3.6 % and hybrid NOTES with 5.7 % was low and comparable to the German data [23]. Furthermore, the conversion rates to open surgery were only 1.4 % and 1 % for SIL and hybrid NOTES, respectively. The registry does not distinguish between conversion before or after attempted NOTES access, so most of the conversions to laparoscopy in the NOTES group are assumed to have been performed before a natural orifice access was established due to the findings of the prior diagnostic laparoscopy. There was only one conversion due to intraoperative access-related complication in transvaginal sigmoidectomy.
Surgeon experience differed considerably between SIL and hybrid NOTES. SIL surgeons were more proficient in laparoscopy, and most were consultants. The proportion of teaching procedures in SIL was very low, however, at 4 %, whereas with hybrid NOTES, 43 % of procedures were taught mostly to fellows. Residents performed none of SIL and only 8 % of hybrid NOTES procedures. The higher proportion of teaching procedures in hybrid NOTES may be explained by the fact that using a rigid hybrid approach the surgical technique is largely similar to conventional laparoscopy except for trocar placement, organ retrieval and in some cases bowel anastomosis. For hybrid NOTES, the principle of laparoscopic procedures remains unchanged, the triangulation of instruments is preserved, and the same instruments are used as for standard laparoscopy. By contrast, in SIL, the possibility of triangulating the instruments is limited, articulating or curved instruments are used in some cases, and it is partly difficult to handle the camera. Furthermore, the case volume of participating centers was lower for SIL than for hybrid NOTES. The supervising surgeon must overcome a personal learning curve before teaching the procedure. It could also be argued that surgeons felt more safe and confident with their performance in hybrid NOTES than in SIL and were therefore keener to share their skills. The shift of typical teaching procedures to a higher level of difficulty by SIL and NOTES is worrisome. Common procedures such as cholecystectomy and sigmoidectomy should generally be taught to fellows and resident. Therefore, in surgical departments performing SIL and NOTES at a high volume every effort should be taken to support younger colleagues in adopting the novel techniques. Even though the supervising surgeon may not feel comfortable teaching SIL and NOTES specific steps of the procedure, the steps of the operation that are similar to conventional laparoscopy should be taught. It has been shown that teaching in novel technologies is possible in a high proportion of patients. In a recent Japan report, residents performed 77 % of 202 single port appendectomies [24] and 49 % of 301 single port totally extraperitoneal inguinal hernia repair [25].
In a 5-year period, 650 patients were included in the D-SENT registry, corresponding to the inclusion of 130 patients per year. The largest registry on novel access in abdominal surgery is the German registry [23]. Yet, in the Swiss D-SENT registry, the yearly inclusion of patients was higher than in the German D-NOTES, including 16.3 and 6.6 patients per million inhabitants, respectively. Similar to the German registry, the number of participating hospitals in the registry was low. After an initial peak, the number of centers and, although not statistical significant, the number of included SIL and hybrid NOTES procedures decreased over the study period. With a higher sample size and a longer observation time, this trend might well become significant. Even though it is not evident from the registry if this decline is real or if surgeons gradually ceased to include cases, it must be assumed that the interest in SIL and NOTES is fading away. Meta-analyses on SIL versus conventional laparoscopy failed to show significant advantages for SIL. So, no differences in pain level were found for appendectomy and for cholecystectomy [26, 27]. A slightly faster bowel recovery in SIL colectomy is probably of minor clinical importance [28]. Concerning hybrid NOTES, meta-analyses demonstrated lower pain level and analgesics consumption for transvaginal hybrid NOTES cholecystectomy compared to multiport cholecystectomy [3]. Furthermore, a meta-analysis on laparoscopic colectomy with and without natural orifice specimen extraction showed reduced pain, shorter hospital stay, and better cosmetic result for hybrid NOTES [2]. However, the advantages to conventional laparoscopy are of questionable clinical importance. Based on the rather vague evidence supporting SIL and hybrid NOTES, the initial enthusiasm for these techniques faded and only a few, and specialized surgeons continue to offer SIL and NOTES.
The hospitals that are scientifically active in novel techniques have mostly participated in the registry, and it is assumed that those centers are also most clinically active. However, a quite large number of unknown cases were probably performed by surgeons using SIL and NOTES infrequently and are not included in the registry. Those cases are most prone to complications because procedures are performed within the individual learning curve. Unfortunately, the voluntary registry misses such cases for monitoring, and the societies eventually fail to meet their goals for quality assurance.
In conclusion, although a few specialized centers perform a quite high proportion of standard procedures in SIL or hybrid NOTES technique, there is a fading interest of the surgical community in SIL and NOTES. The number of hospitals performing SIL and hybrid NOTES as well as the number of performed procedures is declining. The proportion of SIL and hybrid NOTES procedures taught to residents is currently insufficient and must be improved.
References
Li L, Tian J, Tian H, Sun R, Wang Q, Yang K (2014) The efficacy and safety of different kinds of laparoscopic cholecystectomy: a network meta analysis of 43 randomized controlled trials. PLoS One 9(2):e90313
Ma B, Huang XZ, Gao P, Zhao JH, Song YX, Sun JX et al (2015) Laparoscopic resection with natural orifice specimen extraction versus conventional laparoscopy for colorectal disease: a meta-analysis. Int J Colorectal Dis 30(11):1479–1488
Xu B, Xu B, Zheng WY, Ge HY, Wang LW, Song ZS et al (2015) Transvaginal cholecystectomy vs conventional laparoscopic cholecystectomy for gallbladder disease: a meta-analysis. World J Gastroenterol 21(17):5393–5406
Lurje G, Raptis DA, Steinemann DC, Amygdalos I, Kambakamba P, Petrowsky H et al (2015) Cosmesis and body image in patients undergoing single-port versus conventional laparoscopic cholecystectomy: a Multicenter Double-blinded Randomized Controlled Trial (SPOCC-trial). Ann Surg 262(5):728–735
Zhou H, Jin K, Zhang J, Wang W, Sun Y, Ruan C et al (2014) Single incision versus conventional multiport laparoscopic appendectomy: a systematic review and meta-analysis of randomized controlled trials. Dig Surg 31(4–5):384–391
Khashab MA, Kalloo AN (2012) NOTES: current status and new horizons. Gastroenterology 142(4):704-10 e1
Zornig C, Emmermann A, von Waldenfels HA, Mofid H (2007) Laparoscopic cholecystectomy without visible scar: combined transvaginal and transumbilical approach. Endoscopy 39(10):913–915
Marescaux J, Dallemagne B, Perretta S, Wattiez A, Mutter D, Coumaros D (2007) Surgery without scars: report of transluminal cholecystectomy in a human being. Arch Surg 142(9):823–826; discussion 6–7
Ross S, Rosemurgy A, Albrink M, Choung E, Dapri G, Gallagher S et al (2012) Consensus statement of the consortium for LESS cholecystectomy. Surg Endosc 26(10):2711–2716
Autorino R, Yakoubi R, White WM, Gettman M, De Sio M, Quattrone C et al (2013) Natural orifice transluminal endoscopic surgery (NOTES): where are we going? A bibliometric assessment. BJU Int 111(1):11–16
McMahon AJ, Fischbacher CM, Frame SH, MacLeod MC (2000) Impact of laparoscopic cholecystectomy: a population-based study. Lancet 356(9242):1632–1637
Klugsberger B, Haas D, Oppelt P, Neuner L, Shamiyeh A (2015) Current state of laparoscopic colonic Surgery in Austria: a national survey. J Laparoendosc Adv Surg Tech Part A 25(12):976–981
Pan MX, Liang ZW, Cheng Y, Jiang ZS, Xu XP, Wang KH et al (2013) Learning curve of transumbilical suture-suspension single-incision laparoscopic cholecystectomy. World J Gastroenterol 19(29):4786–4790
Tay CW, Shen L, Hartman M, Iyer SG, Madhavan K, Chang SK (2013) SILC for SILC: single institution learning curve for single-incision laparoscopic cholecystectomy. Minim Invasive Surg 2013:381628
Kim CW, Kim WR, Kim HY, Kang J, Hur H, Min BS et al (2015) Learning curve for single-incision laparoscopic anterior resection for sigmoid colon cancer. J Am Coll Surg 221(2):397–403
Park Y, Yong YG, Yun SH, Jung KU, Huh JW, Cho YB et al (2015) Learning curves for single incision and conventional laparoscopic right hemicolectomy: a multidimensional analysis. Ann Surg Treat Res 88(5):269–275
Wood SG, Panait L, Duffy AJ, Bell RL, Roberts KE (2014) Complications of transvaginal natural orifice transluminal endoscopic surgery: a series of 102 patients. Ann Surg 259(4):744–749
Al-Akash M, Boyle E, Tanner WA (2009) Training on N.O.T.E.S.: from history we learn. Surg Oncol 18(2):111–119
Meining A, Feussner H, Swain P, Yang GZ, Lehmann K, Zorron R et al (2011) Natural-orifice transluminal endoscopic surgery (NOTES) in Europe: summary of the working group reports of the Euro-NOTES meeting 2010. Endoscopy 43(2):140–143
Meining A, Kahler G, von Delius S, Buess G, Schneider A, Hochberger J et al (2009) Natural orifices transluminal endoscopic surgery (NOTES) in Germany: summary of the working group reports of the “D-NOTES meeting 2009”. Z Gastroenterol 47(11):1160–1167
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240(2):205–213
Weiss HG, Brunner W, Biebl MO, Schirnhofer J, Pimpl K, Mittermair C et al (2014) Wound complications in 1145 consecutive transumbilical single-incision laparoscopic procedures. Ann Surg 259(1):89–95
Lehmann KS, Ritz JP, Wibmer A, Gellert K, Zornig C, Burghardt J et al (2010) The German registry for natural orifice translumenal endoscopic surgery: report of the first 551 patients. Ann Surg 252(2):263–270
Wakasugi M, Tei M, Omori T, Anno K, Mikami T, Tsukada R et al (2016) Single-incision laparoscopic surgery as a teaching procedure: a single-center experience of more than 2100 procedures. Surg Today. doi:10.1007/s00595-016-1315-7
Wakasugi M, Tei M, Anno K, Mikami T, Tsukada R, Koh M et al (2016) Single-incision totally extraperitoneal inguinal hernia repair as a teaching procedure: one center’s experience of more than 300 procedures. Surg Today 46(9):1039–1044
Trastulli S, Cirocchi R, Desiderio J, Guarino S, Santoro A, Parisi A et al (2013) Systematic review and meta-analysis of randomized clinical trials comparing single-incision versus conventional laparoscopic cholecystectomy. Br J Surg 100(2):191–208
Xue C, Lin B, Huang Z, Chen Z (2015) Single-incision laparoscopic appendectomy versus conventional 3-port laparoscopic appendectomy for appendicitis: an updated meta-analysis of randomized controlled trials. Surg Today 45(9):1179–1186
Podda M, Saba A, Porru F, Pisanu A (2016) Systematic review with meta-analysis of studies comparing single-incision laparoscopic colectomy and multiport laparoscopic colectomy. Surg Endosc. doi:10.1007/s00464-016-4812-2
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Drs. Daniel C. Steinemann, Andreas Zerz, Michel Adamina, Walter Brunner, Andreas Keerl, Antonio Nocito, Andreas Scheiwiller, René Spalinger, Sebastian H. Lamm and Prof. Stephan A. Vorburger have no conflicts of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Steinemann, D.C., Zerz, A., Adamina, M. et al. Single-Incision and Natural Orifice Translumenal Endoscopic Surgery in Switzerland. World J Surg 41, 449–456 (2017). https://doi.org/10.1007/s00268-016-3723-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-016-3723-7