
Abstract
Introduction
Platysmal bands are an unappealing feature of the aging face. Incomplete understanding of anatomy and physiology of platysmal bands has led to a long period of flawed or incomplete treatment. This review aims to elucidate the correct study of platysmal bands along with the most recent surgical treatments.
Materials and Methods
To identify all articles related to the topic of surgical management of platysmal bands, an extensive search was performed on PubMed and Medline databases for all articles related to platysmal bands from 1990 to 2023. The articles were then reviewed by 2 independent reviewers, and all relevant articles were selected. The search was narrowed down to clinical trials and cohort studies.
Results
6130 articles were identified, of which 21 articles matched the inclusion criteria and were selected for the study totaling 2331 patients. Different surgical procedures were mentioned. Assessment of results was mostly subjective and done by the surgeon.
Conclusion
Composite platysma-skin flap repositioning as opposed to wide skin undermining with or without submental incisions is being gradually accepted as a valid approach, with closed platysma myotomy and platysma denervation emerging as effective less invasive surgical modalities. Nevertheless, merits of more extensive procedures involving wide skin undermining and anterior platysma plication must not be lightly forgotten.
Level of Evidence III
This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The attributes of a youthful neck as defined by Ellenbogen et al. [1] include distinct inferior mandibular border, subhyoid depression, visible thyroid cartilage bulge, visible anterior sternocleidomastoid border and a cervico-mental angle of 105-120 degrees. In addition to skin sagging and excess of submental fat deposits, one of the most frustrating stigmata and first signs of neck aging are platysma muscle bands. One or two bands along the anterior segment of the neck are the most frequent [2]. They appear approximately at the age of 55 and increase exponentially thereafter [3, 4].
Several classifications of neck aging combinations based on degree of skin laxity and neck adiposity in addition to platysma banding, retrognathia, and low hyoid position have been proposed together with algorithms for their management [5,6,7,8]. The best strategy to approach changes associated with cervico-facial aging and in particular platysma bands is nevertheless still the subject of much debate [9]. It largely depends on patient preference and goals, budget, general health, and underlying anatomy [10].
Isolated platysmal contractions were demonstrated by Duchenne in 1865 [11]. Platysma bands were first described by Julien Bourguet in 1926 then by Padgett and Stevenson who pinpointed prominent platysma bands as an indicator of a failed rejuvenation procedure [12,13,14]. In view of anatomically demonstrated firm attachment of the platysma to the deep cervical fascia in the region of the hyoid bone, it was traditionally believed that these bands develop because of skin sagging followed by loss of muscle tone. It was subsequently described that anterior platysma bands are rather lateral pleats caused by muscle laxity and not formed by the medial edge proper of the muscle [5, 13].
Though successful in some aspects, most described rejuvenation methods with partial and complete transections and excisions of the platysma have their shortcomings except in very fatty necks. Persistent or recurrent paramedian bands are seen in addition to various contour irregularities with skeletonization or masculinization of the thyroid cartilage. Furthermore, visible submandibular gland bulges are a major drawback that may be accentuated by full width muscle transection [15, 16]. Moreover, McKinney et al have noted that midline muscle plication may result in accentuation of the deformity due to a “bow-stringing effect” in addition to pulling the skin in the wrong direction. Midline muscle dissection and suturing results also in increased morbidity and a “leather neck” that requires 6-8 weeks to resolve [5, 14].
Despite numerous modifications and refinements, and despite some reported decent results, treating platysma bands remains a frustrating and perplexing problem in esthetic neck surgery [17, 18]. Even the most invasive complete neck undermining combined with full-width platysma section which involves a long surgical time with definite risks and entails a long postoperative recovery does not achieve the desired correction of platysma bands and anterior skin laxity in certain patients [19]. Traditional complex techniques involving undermining skin and muscle, midline muscle plication, directed traction, and removal of excess tissue have mostly failed. Even with the most aggressive platysmaplasty maneuvers, frustrating recurrence of bands within 1 year or even less postoperatively is frequent; it can be as high as 40–45% [2, 16, 18, 20,21,22,23,24,25,26,27,28]. Pelle-Ceravolo et al. expressed real concerns about significant failure to maintain long-term correction despite full neck undermining with complete platysma transection and midline approximation [29]. The authors have confirmed that “after 25 years' experience with these deficiencies, a reconsideration of the most appropriate procedure for correction of the anterior neck is warranted.” Experience has since shown that platysma tightening will not universally correct cervical platysma bands. Our traditional view that these bands are simply due to age-related horizontal platysmal laxity is conceptually flawed and is responsible for many decades of failed treatments [20].
Though several described techniques have proved to be effective with some satisfactory long-term outcome, platysma tightening will not always correct cervical bands [30]. Long-lasting, dependable, and least aggressive surgical techniques are still mostly lacking [30, 31]. However, better insight regarding platysma and superficial aponeurotic system anatomy and pathophysiology of platysma banding have been accompanied by introduction of several innovative techniques for neck rejuvenation. The current review is aimed at exploring improved understanding of anatomical and physiological basis of platysma bands development and at analyzing how this improved knowledge has resulted in a major surgical paradigm change for better management and possibly long-lasting outcome.
Material and Methods
A preliminary PubMed and Medline search of published manuscripts in English from 1990 to 2023 was performed using the following search with MESH terms: (((((platysma band) OR (platysma bands)) OR (neck bands)) OR (neck band)) OR (neck ridge)) OR (neck ridges). Abstracts of all relevant manuscripts were independently reviewed by 2 authors. Inclusion criteria were clinical trials and cohort studies about the surgical management of platysma bands. Manuscripts about medical and non-surgical management of platysma bands were excluded along with reviews, discussions, comments, and case reports. Full texts of all identified studies were reviewed along PRISMA guidelines for size of study groups, study design, and outcome measurements; level of evidence was classified according to the rating scale of Ackley et al. for experimental studies and ASPS Evidence Rating Scales for Therapeutic Studies for clinical case series [32, 33].
Results
The search resulted in 6130 articles. 21 studies were found to match inclusion criteria and selected for the study (Table 1). A total of 2331 patients were included in the studies. Different articles used different approaches to surgically correct platysmal bands. The study selection flowchart is included (Fig. 1). Outcome was evaluated subjectively by the surgeons in most studies. Many were based on pre-and post-operative photographs. Though it is possible to evaluate efficacy of neck rejuvenation along Ellenbogen criteria with such type of outcome measure, it is, however, not possible to provide any reliable evidence about long-lasting correction of dynamic cervical bands [1].

Flowchart of Study Selection
Discussion
The platysma muscle is a mimic muscle. It develops similar to the facial mimic muscles together with the supplying facial nerve from sheet like laminae of premyoblast and myoblast. It covers the cervical area and has many anatomical variations [43]. Detailed dissections have revealed that it is a cutaneous muscle composed of horizontal facial and vertical cervical parts. The medial and lateral borders of the platysma are strongly attached to the deep cervical fascia near the hyoid bone and to the same fascia caudal to the mandibular angle [12, 44].
Numerous surgical neck rejuvenation techniques involving various platysma muscle flaps, muscle Z-plasty, and muscle plication to form a deep-layer supportive neck sling have been described. Even suturing of the digastric retaining ligaments to the mylohyoid muscles like a corset has been reported. Techniques with various vectors SMAS advancement with or without midline muscle plication have been reported as well [5, 12, 15, 17, 18, 20, 35, 36, 45,46,47,48,49,50]. Webster et al. have stressed that posterosuperior pulls on intact SMAS and muscle provide the safest, most physiologic correction with very little risk to sub-platysma structures with no permanent abnormal lumps, gaps, or adherences [16]. Total direct band excision to correct what has been originally described as “tone loss” of the platysma has been also described. Nevertheless, medial plication of the platysma has predominantly been emphasized as the most logical and natural way for neck rejuvenation to deal with neck bands to the extreme of presenting skin contraction and redraping, associated with medial platysmaplasty and submental lipectomy through a single limited anterior submental incision without skin excision, as an effective neck rejuvenating modality for patients with good skin elasticity [21, 51, 52].
McKinney described in 1996 a classification of platysma neck bands together with a treatment algorithm [5]. Barely visible Type I bands are easily handled with lateral SMAS tightening alone; moderate Bands II require midline muscle suturing only; more visible Bands III require resection of redundant muscle edges and midline suturing, while severe Bands IV necessitate lateral SMAS pull as well as midline muscle suturing. Feldman described the corset platysmaplasty indicated for all patients with visible paramedian muscle bands and even for patients without preoperative visible bands but would benefit from removal of subplatysmal fat [15]. He reported that recurrence of platysma muscle bands is the result of leaving un-joined muscle edges either below the level of upper midline plication or at new cut muscle edges after vertical excision, horizontal transection or wedge resection. The corset platysmoplasty technique consists in midline suturing of the two medial edges of the platysma with a continuous suture that runs down, and up, and down almost the full-height of the neck to create a smooth, flat, multilayered seam after adequate subcutaneous and subplatysmal lipectomy. Additional submandibular platysma suturing is also done to create strong, flat, vertical muscle pleats that correct submandibular gland bulging and refine the jawline and anterolateral neck contours as well. Le Louarn, for his part, reported anterior subplatysmal dissection with fixation of the anterior platysma to the deep cervical fascia and suspension of the lateral platysma flap to the mastoid [40]. He claimed that his hyo-neck technique definitely improves the cervico-mandibular angle and lateral submandibular area, in addition to simultaneously treating platysma bands.
Understanding Platysma Bands Etiology
Skin sagging followed by loss of platysma muscle tonicity has been the dominant theory for several decades to describe age-related changes of the neck including development of cervical bands. It is traditionally mentioned that the anterior platysma border migrates forward, with the constitution of platysmal bands more or less visible depending on the bloating of the cervicomental angle [12, 44]. On the other hand, the posterior border undergoes only slight modifications if any. However, the most striking changes are observed with sliding downward and forward of the platysma fibers at the junction of the horizontal and vertical platysma parts [12, 44].
Age-related weakening of the cervical fascia has also been presented as a likely pathogenesis of platysma bands [4]. However, the absence of platysmal bands in patients with unilateral facial nerve palsy has drawn the attention to the possibility that formation of bands and platysma muscle contractions could be closely related [43]. It soon became widely accepted that prominent platysma bands reflect hyperkinetic platysma activity and are not related to relaxation of the platysma and skin laxity; skin laxity follows secondarily the anterior part of the platysma and not the other way around [3, 20]. With paradoxically two opposing theories about platysmal bands etiological mechanisms one of which involves platysmal contractions and increased tonicity while the other involves skin sagging and loss of platysma muscle tonicity, different therapeutic concepts with different outcomes have been proposed [43].
The two distinct forms of bands, hard dynamic and soft adynamic in the cervicosubmental region of aging individuals have been well described [53]. Soft, adynamic bands change little during platysma activation and are predominantly a problem of loose skin or horizontal platysmal laxity. In contradistinction, the more frequent hard dynamic bands that are phenotypically different from facial folds become tight or exaggerated upon platysmal activation and indicate a problem of longitudinal platysmal hyperfunction [43]. These bands are not due to fibrosis or rigidity of the tissues or muscle as previously described. Bands caused by longitudinal platysmal hyperfunction are refractory to horizontal pulling suggesting the need for a new approach for management [3, 20].
Reflex muscular contraction of the platysma secondary to cervical hyperlordosis development with aging has been also presented as a likely cause of increased platysma contraction [54]. Hodgkinson claimed that accumulation of submental fat results in hypertonic reflex and banding as the muscle contraction responds to the greater load on the platysma [11]. On the other hand, Olmedo et al. postulated that the physiologic involutive process of the muscle with aging results in loss of its elasticity with shortening even when relaxed; this creates vertical bands that may become pendulous in extreme cases [18]. Regardless of the exact pathophysiology, recent studies support the muscular hyperfunction hypothesis for platysmal banding [2, 20, 53]. However, this hypothesis does not provide sufficient explanation for the clinical presentation of bands in aged individuals particularly in those with thin, less fatty necks in whom skin folds are loose, without tension, and are constantly present, with or without muscular contraction [53]. Regardless of the exact etiology mechanism, Pelle-Ceravolo rightfully stated that “the conundrum to overcome is the dichotomy between hypertonic and hypotonic muscles, because both can create visible bands through hypothetically different mechanisms” [55].
Functional Anatomy and Platysma Bands
The fundamental flaw of the traditional platysma tightening techniques is that they have failed to recognize or address the underlying anatomical differences and differing functional origins of platysma bands [20]. They have underestimated regional architectural differences as well as different fibrous septa arrangements and platysma-skin interactions that were demonstrated to be critical in determining folds and crease formation [43]. Although with early studies the facial SMAS has been considered to be an evolutionary platysmal metamorphosis and that the cervical SMAS and platysma are closely connected forming a single layer, a recent study has demonstrated a fibro-adipose layer with direct fibrous connections between platysma and skin; the underlying platysma functions as a mimetic muscle similar to other facial mimetic muscles. It demonstrated also that facial muscles and platysma have no embracing fascia as also confirmed by Trévidic et al. [3, 43].
Morphologically, platysmal contractions are transferred by fibrous septa to the skin, similar to what occurs in the facial region [43]. Nevertheless, striking differences exist between facial SMAS and that of the neck. Facial fibrous arrangements of SMAS types I, II, and III comprise vertical septa connecting mimetic muscle bundles to the skin. On the other hand, types IV and V cervical SMAS consist of horizontally aligned fibrous septa that are connected by short, vertical, fibrous septa. With this cervical morphological dynamic pattern, a singular platysmal muscle bundle contraction is transferred to the skin level in a multiplanar manner. This is thought to induce platysmal bands [43].
Contrary to earlier reports, more recent computed tomographic analysis correlated with histologic investigation provided evidence that the platysma muscle is in fact enveloped in the superficial cervical fascia with midline and lateral zones of adherence [3, 43, 53]. Upon neural activation, a location-specific isometric muscle contraction has been described to occur in the paramedian plane at the adhesion zone created by fusion of the superficial cervical fascia with the investing layer of the deep cervical fascia next to the midline adhesion zone. Due to the subplatysmal gliding plane, isotonic platysma contraction occurs more laterally. The muscle can thus move and its fibers can shorten and become elevated, observed on the skin surface as paramedian platysmal bands. A similar elevation pattern occurs at the lateral platysma margin [53]. Pattern of platysmal banding is nevertheless subject to anatomical variation likely related to de Castro platysmal fusion types in addition to extent of adhesion zones [56]. Whether release of the fascial adhesion zone between the superficial and deep cervical fascia as recommended recently is necessary for cervical bands correction still awaits to be demonstrated [53].
At any rate, understanding the layered neck cervical fascial and muscular anatomy is essential to implement more effective treatment modalities [43, 53]. It is fundamental to realize that the connection between the skin and the platysma muscle is very tight. They maintain their close relationship without any notable sliding between the two tissues when aging [44]. However, cervical soft-tissue volume loss of both the superficial and deep fatty layers that occurs with progressive aging or weight loss causes the platysma muscle to lose its structured support. Due to the presence of a subplatysmal gliding plane, skin and platysma follow the effects of gravity and neck movements. Additional skin laxity can also exert a pull on the platysma that can glide except in regions of fascial adhesion [53].
Similar to whether a submental incision on a regular basis is indicated, the approximation and direct suturing of paramedian platysma bands on a regular basis is questionable [5, 11, 45]. Furthermore, contrary to previous long-time widespread practice of complete subcutaneous undermining of cervical skin, disruption of the tight relationship between the skin and the platysma does not seem to be morphologically justified. Greater and more dramatic anterior skin remodeling has been demonstrated when traction on the platysma to which the skin remains attached is exerted. As it is becoming apparent, full neck undermining technique could nowadays be considered anachronistic due to necessary extended downtime and the required withdrawal from normal life, a condition that is either unacceptable or impossible for many patients [19].
Pelle-Ceravolo et al. reported good outcomes with lateral skin-platysma displacement technique [19, 57]. Lateral traction applied on the midbody of the platysma after subplatysmal undermining to release cervical retaining ligaments has been reported to allow good mobilization with satisfactory neck remodeling. It is important to note in that regard that lateral platysmal approach plication or undermining does not lead to a widening of the gap between the medial platysmal bands [9]. This finding is in line with the recently described medial zone of adhesion [53]. It does, however, shed some doubts about efficacy of lateral skin-platysma displacement in case of exaggerated midline anterior skin laxity and redundancy.
Relocation of the platysma to its youthful position while maintaining its intimate cutaneous attachment appears nowadays to be the most logical approach to correct adynamic cervical bands. With vertical elevation, subplatysmal undermining is probably not necessary since the platysma has considerable upward sliding excursion [11, 58]. Vertical elevation can be made more dependable with high-tension suturing to the fixed strong anchor point prelobar fibrous tissue of Lore’s fascia without the need for further subplatysmal dissection [58].
Myotomy and Neurotomy for Management of Dynamic Platysma Bands
Management of dynamic cervical bands of McKinney grades III or IV, on the other hand, requires more than simple superolateral platysma tightening and relocation. Horizontal pulling of longitudinal platysmal hyperfunction bands is largely ineffective; it may provide only a short-time correction [3, 20]. Selective myotomy, myectomy, or neurotomy are more effective in regulating mimetic hyperkinesia [59]. To disrupt longitudinal hyperfunction, horizontal platysma transection has been recommended [2, 20]. Closed platysma myotomy technique using mini-incisions was introduced by Julien Bourguet [12]. The technique was revived by Saylan who recommended serial notching of the platysmal bands [41]. The procedure can also be used as an isolated procedure in patients with minor skin laxity as reported by Gonzalez, Daher, Clarós et al. and Hegazy [2, 12, 30, 38, 60]. The myotomy is usually performed at 3-6 sites 3-5 cm apart along each band depending on its length.
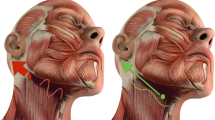
Alternatively, intentional cervical branch neurotomy has been proposed as being potentially a permanent treatment for platysmal banding. It must be mentioned in this context that with almost all the classical techniques described in the literature for platysma manipulation, even with the more aggressive techniques in terms of undermining and muscle division, innervation to the platysma appears to remain intact both cranial and caudal to any transection maneuvers [22, 53]. Minelli et al. have detailed in a very recent anatomical study platysma segmental innervation as well as its bony, fascial, and dermal attachments [61]. The authors have described the innervation of the cervical segment of the platysma by terminal branches of the cervical branch of the facial nerve (CBFN). These branches come off the main cervical trunk of the CBFN which runs deep within the deep fascia along the anterior border of the sternocleidomastoid muscle. The authors have confirmed also that there were no nerves innervating the platysma in the posterior triangle of the neck. Sinno et al. reported that muscle innervation is quite far medial at approximately the point where the cervical branch of the facial nerve crosses the facial vessels and is unlikely to be injured unless undermining of the muscle extends to this point [22].
Denervation of the entire platysma can be achieved with lateral neurotomy [22]. The cervical branch of the facial nerve can be reliably identified within 1 cm below a perpendicular line from the angle of the mandible to a line drawn from the mentum to the mastoid process [62]. Trévidic et al. described transection of the cervical branches of the facial nerve after careful dissection and elevation of the margin of the SMAS in the subplatysmal plane starting from the inferior part of the muscular border where it covers the sternocleidomastoid muscle and precise identification of the nerves using intra-operative electrical stimulation [23]. In contradistinction, medial neurotomy has been reported to result in more selective denervation of the medial platysma [22]. Appreciation of the dynamic nature of some forms of platysma banding as well as the value of selective denervation has opened the way to minimally invasive treatments rapidly gaining in popularity and provided the scientific basis for their efficacy. Non-surgical selective chemical denervation of the hyperkinetic muscle with botulinum A exotoxin is nowadays a well-accepted alternative approach for temporary improvement [4, 63, 64].
Though apparently a logical and attractive modality, intentional surgical platysma denervation to correct platysma bands is not without stirring debate and raising serious controversies. Concerns about effect of muscle denervation on submandibular contour may be genuine. Complete platysma denervation may potentially lead to unmasking of sub-platysmal structures as the muscle that becomes flaccid [22]. Moreover, it is questionable whether a thin and atrophic muscle as a result of denervation would be able to maintain adequate neck contour over time. Moreover, possible marginal mandibular nerve “pseudo marginal mandibular palsy” as a result of lateral denervation of the upper branch of the cervical nerve is not to be taken lightly, though Sinno et al. believe that this condition is not due to cervical branch injury but is more likely due to temporary swelling of the marginal mandibular branch [22]. Nevertheless, in view of the recent anatomical study of Minelli et al., the recommendation of sparing the first CBFN considering its ending near the menton and potential function on the lower lip depressor labii muscle, and maintaining adequate tone of the platysma cranial segment, is well justified [61]. This may be achieved by total deep cervical fasciotomy below the level of the hyoid bone that transects all lower CBFN branches to the cervical platysma while sparing the upper CBFN branches to the submandibular platysma and lower lip depressor muscle [65]. Nevertheless, reinnervation is a complex issue with likely neurotization after simple CBFN transection, precluding permanent platysma denervation. Before confidently recommending routine caudal platysma denervation, further study of this innovative modality is needed. Preliminary experience is encouraging; it may turn out to be safe and highly effective [61, 66].
Alloplastic Neck Slings
Dissatisfied with most of the current approaches for neck rejuvenation that do not fit all cases and tend to focus on correction of specific aspects of the aging neck, neck artificial sling using alloplastic mesh to elevate all of the descending elements as a whole instead of manipulating the platysma has been described associated with resection of redundant skin as needed to create a natural and longstanding result [24, 39]. It is claimed that the quality of neck improvement using this technique seems to be superior to other approaches of neck rejuvenation. Results are also claimed to be uniform and smooth and seem to be long-lasting [24]. Infection of the mesh matrix is, however, a potential serious complication and unbiased confirmation of safety and efficacy of this approach is still pending [24, 67].
Innovative Techniques and Objective Analysis of Outcomes
In view of the wide variation of deformities encountered in aging necks and the necessity to individualize each patient’s needs, it is apparent from this review that there is no one-for-all rejuvenation technique applicable to all patients [58]. Soft adynamic bands may be corrected by superolateral platysma displacement, while hard dynamic bands require a more direct approach either by partial or total transection, band myotomy, myectomy, or even platysma denervation. Moreover, by favoring lateral skin-platysma displacement, midline platysma plication and wide cutaneous undermining would be counterproductive. On the other hand, applying the principle of skin-platysma displacement in patients with heavy necks necessitating direct fat excision or in patients with excessive anterior skin and platysma laxity may not be possible. Nevertheless, when the integrity of the intimate platysma cutaneous attachment becomes questionable in case of liposuction of submental fat, wide subcutaneous undermining may still be not necessary. Liposuction tunneling creates in most cases adequate cutaneous sliding making desirable neck contouring possible through differential lateral traction and displacement of platysma and skin because they remain anatomically connected.
Non-standard creative solutions for the management of challenging clinical conditions are unique characteristics of plastic surgery. Furthermore, no other branch of medicine and surgery can promote new techniques and procedures more than esthetic medicine and surgery with limited scientific objective proof of efficacy. Though neurotoxin injection below the zygomatic arch in the lower face is still not an FDA approved indication for rejuvenation, chemodenervation of the platysma muscle is currently performed and marketed as an effective minimally invasive modality for the treatment of platysma bands [68]. Furthermore, botulinum toxin injections are believed to block muscle regeneration whenever horizontal section of the platysma is performed though solid evidence of this effect is still lacking [69]. It will not be surprising that in a not so far future various anti-aging and tissue regeneration modalities to rejuvenate the neck and efface platysma bands may emerge as potential alternatives.
However, in an era of evidence-based medicine, and in view of the many limitations of conventional outcome evaluation tools of esthetic interventions, importance of objective assessment of outcome cannot be overstated before any of the interventions can be safely recommended. Instead of currently used patient reported ill-defined outcomes and subjective measures very often from the patients’ and/or providers’ perspective, the present hi-tech era is offering great opportunities to obtain objective and reproducible measurements. Versatile digital photography and measuring systems and tools could be applied in daily clinical practice to assess efficacy of any treatment modality [70]. Patient outcomes and neck deformity recurrence may be as well determined in a way similar to what has been reported with the LACE+ Index and objectively assess adverse outcomes in a plastic surgery population [71]. Furthermore, artificial intelligence machine learning, in particular facial emotion recognition systems, and eye-tracking visual gaze analysis are very promising. Both can objectively quantitate outcomes and define esthetic interventions’ success from both the patients’ and observers’ perspectives [72].
Conclusion
Perhaps, obtaining predictable results in cervical contouring is one of the most challenging aspects of face and neck rejuvenating procedures. With improved understanding of platysma muscle biophysical changes related to aging, cervical bands treatment techniques and neck rejuvenation modalities have dramatically evolved. Composite platysma-skin flap repositioning as opposed to wide skin undermining with or without submental incisions is being gradually accepted as a valid approach. Furthermore, closed platysma myotomy and platysma denervation are emerging as effective less invasive surgical modalities. Nevertheless, merits of more extensive procedures involving wide skin undermining and anterior platysma plication must not be lightly forgotten. It must also be realized that the outcome of any given procedure for neck rejuvenation is largely dependent on several factors including pre-operative neck morphology and degree of skin redundancy as well as skin quality and age of the patient.
References
Ellenbogen R, Karlin JV (1980) Visual criteria for success in restoring the youthful neck. Plast Reconstr Surg 66(6):826–837
Daher JC (2011) Closed platysmotomy: a new procedure for the treatment of platysma bands without skin dissection. Aesthetic Plast Surg 35(5):866–877
Trévidic P, Criollo-Lamilla G (2017) Platysma bands: Is a change needed in the surgical paradigm? Plast Reconstr Surg 139(1):41–47
Rohrich RJ, Savetsky IL, Cohen JM, Avashia YJ (2020) Effective treatment of platysma bands with neurotoxin. Plast Reconstr Surg Glob Open 8(6):e2812. https://doi.org/10.1097/GOX.0000000000002812
McKinney P (1996) The management of platysma bands. Plast Reconstr Surg 98(6):999–1006
Rohrich RJ, Rios JL, Smith PD, Gutowski KA (2006) Neck rejuvenation revisited. Plast Reconstr Surg 118(5):1251–1263. https://doi.org/10.1097/01.prs.0000209406.80690.9f
Friedman O, Shamban A, Fabi S, Duncan DI, Artzi O (2021) The aging neck-A case base treatment algorithm. J Cosmet Dermatol 20(2):569–576. https://doi.org/10.1111/jocd.13877
Dedo DD (1980) “How I do it–plastic”--surgery. Practical suggestions on facial plastic surgery. A preoperative classification of the neck for cervicofacial rhytidectomy. Laryngoscope 90(11):1894–1896
Charles-de-Sá L, Gontijo-de-Amorim NF, Loureiro Claro V, Vieira DML, de Andrade GM, Dantas-Rocha L, da Silva CGR, Abboudib JH, de Castro CC (2020) Does the approach of the lateral platysmal bands widen the gap between the medial bands? Plast Reconstr Surg Glob Open 8(6):e2853. https://doi.org/10.1097/GOX.0000000000002853
Pérez P, Hohman MH (2022) Neck rejuvenation. StatPearls Publishing, Treasure Island (FL)
Hodgkinson DJ (2012) Five-year experience with modified Fogli (Loré’s fascia fixation) platysmaplasty. Aesthetic Plast Surg 36(1):28–40
Gonzalez R (2009) Composite platysmaplasty and closed percutaneous platysma myotomy: a simple way to treat deformities of the neck caused by aging. Aesthet Surg J 29(5):344–354
Padgett EC, Stephenson KL (1948) Plastic and Reconstructive Surgery. Thomas CC, Springfield, IL, p 638
McKinney P, Tresley GE (1984) The “maxi-SMAS”: management of the platysma bands in rhytidectomy. Ann Plast Surg 12(3):260–267
Feldman JJ (1990) Corset platysmaplasty. Plast Reconstr Surg 85(3):333–343
Webster RC, Hamdan US, Fuleihan NS, Haddad NM, Smith RC (1987) Cosmetic platysmal surgery. Facial Plast Surg 4(2):97–126
Guyuron B, Sadek EY, Ahmadian R (2010) A 26-year experience with vest-over-pants technique platysmarrhaphy. Plast Reconstr Surg 126(3):1027–1034
Olmedo A, Longato F (2002) The case for full-width platysma transection and rotation. Aesthetic Plast Surg 26(4):239–250
Pelle-Ceravolo M, Angelini M, Silvi E (2017) Treatment of anterior neck aging without a submental approach: lateral skin-platysma displacement, a new and proven technique for platysma bands and skin laxity. Plast Reconstr Surg 139(2):308–321
Marten T, Elyassnia D (2018) Management of the platysma in neck lift. Clin Plast Surg 45(4):555–570
Knize DM (1998) Limited incision submental lipectomy and platysmaplasty. Plast Reconstr Surg 101(2):473–481
Sinno S, Thorne CH (2019) Cervical branch of facial nerve: an explanation for recurrent platysma bands following necklift and platysmaplasty. Aesthet Surg J 39(1):1–7
Trévidic P, Criollo-Lamilla G (2019) Surgical denervation of platysma bands: a novel technique in rhytidectomy. Plast Reconstr Surg 144(5):798e–802e
Gronovich Y (2018) Innovative surgical approach using a mesh sling for the aging neck. Plast Reconstr Surg 141(6):1386–1391
Geister TL, Bleßmann-Gurk B, Rzany B, Harrington L, Görtelmeyer R, Pooth R (2013) Validated assessment scale for platysmal bands. Dermatol Surg 39(8):1217–1225. https://doi.org/10.1111/dsu.12240
Stuzin JM (2017) Discussion: treatment of anterior neck aging without a submental approach: lateral skin-platysma displacement, a new and proven technique for platysma bands and skin laxity. Plast Reconstr Surg 139(2):322–323
Biggs TM, Koplin L (1983) Concepts of neck lift. Clin Plast Surg 10(3):367–378
Tonnard PL, Verpaele A, Gaia S (2005) Optimising results from minimal access cranial suspension lifting (MACS-lift). Aesthetic Plast Surg 29(4):213–220
Pelle-Ceravolo M, Angelini M, Silvi E (2016) Complete platysma transection in neck rejuvenation: a critical appraisal. Plast Reconstr Surg 138(4):781–791
Clarós P, Aleksandra S, Clarós A (2020) Simple management of the neck platysma bands: a technique. Int J Otorhinolaryngol Head Neck Surg 6(10):1927–1931
Fedok FG (2020) Another look at platysmaplasty in facelifting. Facial Plast Surg 36(4):395–403
Ackley BJ, Ladwig GB, Swan BA, Tucker SJ (2007) Evidence-based nursing care guidelines. Elsevier Health Sciences
Atiyeh BS, Chahine F (2022) Objective outcome measure of beauty and attractiveness in esthetic surgery: making the impossible possible. J Craniofac Surg 33(8):2323–2324
Feldman JJ (2014) Neck lift my way: an update. Plast Reconstr Surg 134(6):1173–1183
Newman J, Dolsky RL (1983) Innovations in platysma rhytidectomy. Arch Otolaryngol 109(10):637–641
van der Lei B, Cromheecke M, Hofer SO (2009) The purse-string reinforced SMASectomy short scar facelift. Aesthet Surg J 29(3):180–188
Gonzalez R (2013) Closed platysmotomy: a new procedure to treat platysma bands. Aesthetic Plast Surg 37(3):636–637
Feldman JJ (2017) Discussion: Platysma bands: Is a change needed in the surgical paradigm? Plast Reconstr Surg 139(1):48–49
Ramirez OM (1997) Cervicoplasty: nonexcisional anterior approach. Plast Reconstr Surg 99(6):1576–1585
Mühlbauer W, Fairley J, van Wingerden J (1995) Mimetic modulation for problem creases of the face. Aesthetic Plast Surg 19(2):183–191
Yousif NJ, Matloub HS, Sanger JR (2016) Hyoid suspension neck lift. Plast Reconstr Surg 138(6):1181–1190
American Society of Plastic Surgeons (2011) ASPS Evidence Rating Scales. www.plasticsurgery.org/documents/medical-professionals/health-policy/evidence-practice/ASPS-Rating-Scale-March-2011.pdf
Sandulescu T, Stoltenberg F, Buechner H, Schmidt-Park H, Linnerz F, Jast J, Franzmann M, Blaurock-Sandulescu T, Naumova EA, Arnold WH (2020) Platysma and the cervical superficial musculoaponeurotic system - Comparative analysis of facial crease and platysmal band development. Ann Anat 227:151414. https://doi.org/10.1016/j.aanat.2019.151414
Fogli AL (2008) Skin and platysma muscle anchoring. Aesthetic Plast Surg 32(3):531–541
Citarella ER, Condé-Green A, Sinder R (2010) Triple suture for neck contouring: 14 years of experience. Aesthet Surg J 30(3):311–319
Guerrerosantos J (2008) Managing platysma bands in the aging neck. Aesthet Surg J 28(2):211–216
Labbé D, Giot JP, Kaluzinski E (2013) Submental area rejuvenation by digastric corset: anatomical study and clinical application in 20 cases. Aesthetic Plast Surg 37(2):222–231
Connell BF (1976) Cervical lift: Surgical correction of fat contour problems combined with full-width platysma muscle flaps. Aesthetic Plast Surg 1(1):355–362
Abramo AC, Oliveira VR (2000) The “lazy S-shaped” plication of the SMAS-platysma musculoaponeurotic system: a 10-year review. Aesthetic Plast Surg 24(6):433–439
Connell BF (1978) Cervical lifts: the value of platysma muscle flaps. Ann Plast Surg 1(1):32–43
Mottura AA (1999) Cervical rhytidectomy. Aesthetic Plast Surg 23(3):179–188
Le Louarn C (2018) Hyo-neck lift evolution: neck lift with fixation of the platysma to the deep cervical fascia. Ann Chir Plast Esthet 63(2):164–174
Davidovic K, Frank K, Schenck TL, Cohen SR, Dayan S, Gotkin RH, Sykes JM, Liew S, Gavril D, Cotofana S (2021) Anatomy behind the paramedian platysmal band: a combined cadaveric and computed tomographic study. Plast Reconstr Surg 148(5):979–988. https://doi.org/10.1097/PRS.0000000000008414
Knipper P, Mitz V (2017) Platysma bands: Is a change needed in the surgical paradigm? Plast Reconstr Surg 140(5):755e
Pelle-Ceravolo M (2021) Discussion: anatomy behind the paramedian platysmal band: a combined cadaveric and computed tomographic study. Plast Reconstr Surg 148(5):989–991
de Castro CC (1980) The anatomy of the platysma muscle. Plast Reconstr Surg 66(5):680–683
Pelle-Ceravolo M, Angelini M (2019) Lateral skin-platysma displacement: a new approach to neck rejuvenation through a lateral approach. Clin Plast Surg 46(4):587–602
Athanasiou A, Rempelos G (2014) Lore’s fascia a strong fixation point for neck rejuvenation procedures. Clin Plast Surg 41(1):43–49
Saylan Z (2001) Serial notching of the platysma bands. Aesthet Surg J 21(5):412–417
Hegazy AM, Farouk M (2017) A simplified method for management of platysmal bands: platysmotomy as an office procedure. Aesthetic Plast Surg 41(6):1351–1359
Minelli L, Wilson JL, Bravo FG, Hodgkinson DJ, O'Daniel TG, van der Lei B, Mendelson BC (2023) The functional anatomy and innervation of the platysma is segmental: implications for lower lip dysfunction, recurrent platysmal bands, and surgical rejuvenation. Aesthet Surg J sjad148. https://doi.org/10.1093/asj/sjad148
Chowdhry S, Yoder EM, Cooperman RD, Yoder VR, Wilhelmi BJ (2010) Locating the cervical motor branch of the facial nerve: anatomy and clinical application. Plast Reconstr Surg 126(3):875–879. https://doi.org/10.1097/PRS.0b013e3181e3b374
Matarasso A, Matarasso SL, Brandt FS, Bellman B (1999) Botulinum A exotoxin for the management of platysma bands. Plast Reconstr Surg 103(2):645–652; discussion 653–655. https://doi.org/10.1097/00006534-199902000-00043
Engerer N, Frank K, Moellhoff N, Alfertshofer M, Giunta RE, Green JB, Lorenc PZ, Chaney GK, Ehrl D, Cotofana S (2022) Aging of the neck decoded: new insights for minimally invasive treatments. Aesthetic Plast Surg 46(4):1698–1705. https://doi.org/10.1007/s00266-022-02961-0
Bravo FG (2022) Neck contouring and rejuvenation in male patients through dual-plane reduction neck lift. Clin Plast Surg 49(2):257–273
Gennai A (2018) Minimally invasive neck rejuvenation of moderate cervicomental laxity with polytetrafuoroethylene (PTFE) bands. Eur J Plast Surg 41(6):625–636
Prabhat A, Dyer WK 2nd (2003) Improving surgery on the aging neck with an adjustable expanded polytetrafluoroethylene cervical sling. Arch Facial Plast Surg 5(6):491–501
Matarasso SL, Matarasso A (2019) Commentary on: botulinum toxin treatment for mild to moderate platysma bands: a systematic review of efficacy, safety, and injection technique. Aesthet Surg J 39(2):207–208
Le Louarn C (2021) Face lift with U threads. Ann Chir Plast Esthet 66(1):62–68
Guarro G, Cozzani F, Rossini M, Bonati E, Del Rio P (2021) Wounds morphologic assessment: application and reproducibility of a virtual measuring system, pilot study. Acta Biomed 92(5):e2021227. https://doi.org/10.23750/abm.v92i5.11179
Winter E, Glauser G, Caplan IF, Goodrich S, McClintock SD, Kovach SJ 3rd, Fosnot J, Serletti JM, Malhotra NR (2020) The LACE+ index as a predictor of 30-day patient outcomes in a plastic surgery population: a coarsened exact match study. Plast Reconstr Surg 146(3):296e–305e. https://doi.org/10.1097/PRS.0000000000007064
Choi J, Hwang K (2020) Modified medial and lateral platysmaplasty. J Craniofac Surg 31(7):1958–1961
Acknowledgements
This article does not contain any studies with human participants or animals performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Consent for Publication
For this type of study, formal consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Atiyeh, B., Emsieh, S., Oneisi, A. et al. Surgical Management of Platysma Bands: A Narrative Review of Evolving Concepts and Changing Techniques for Neck Rejuvenation. Aesth Plast Surg 47, 1824–1834 (2023). https://doi.org/10.1007/s00266-023-03604-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-023-03604-8