
Abstract
Background
Capsular contracture is a severe complication to breast surgery with implants. Previous studies suggest multiple risk factors are associated with capsular contracture, but the etiology is still unknown. We performed a literature review to investigate existing studies on histological analyses of breast implant capsules and how clinical risk factors impact the capsule morphology.
Methods
The literature search was conducted in PubMed. Studies that performed histological analyses of breast implant capsules were included. Animal studies or studies with a study population of less than five patients were excluded.
Results
Fifty-two studies were included. The histological analyses showed that the breast implant capsules were organized in multiple layers with an inner layer of synovial-like metaplasia which was reported to diminish in capsules with capsular contracture. The remaining layers of the capsule mostly consisted of collagen. The alignment of the collagen fibers differed between contracted and non-contracted capsules, and capsules with higher Baker grade were generally thickest and contained more tissue inflammation. Studies investigating capsules affected by radiotherapy found a more pronounced inflammatory response and the capsules were generally thicker and fibrotic compared with nonirradiated capsules.
Conclusions
The included studies offer valuable insights into the histological changes caused by capsular contracture and their relation to clinical risk factors. Further studies with larger sample sizes and more strict inclusion criteria are needed to further investigate implant capsules and the role of the synovial-like metaplasia for the development of capsular contracture.
Level of Evidence III
This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors https://www.springer.com/00266.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
When a breast implant is inserted in the human body, the immune system reacts by forming a thin fibrous capsule. In some women, the capsule undergoes a progressive thickening and starts contracting around the implant in a process called capsular contracture. Capsular contracture affects between 2.8% and 20.4% of women with implants [1,2,3,4,5,6] and can cause chronic pain and deformation of the breast. The Baker classification system [7] is commonly used to determine the severity of capsular contracture during a clinical examination of the breast. The treatment of severe capsular contracture is surgical removal of the capsule and exchange of the implant which is agonizing for the patient. The etiology of capsular contracture is undetermined, but multiple clinical risk factors including infection, radiotherapy, implant surface texture and silicone leakage have been suggested to cause capsular contracture. In order to develop preventive strategies, it is important to understand the histological changes of the implant capsule during the ongoing immune reaction, and how these are associated with clinical risk factors. In this study, we review histological studies of capsular contracture to evaluate the current knowledge about the histological morphology, the relation to the clinical symptoms of capsular contracture and its association with known risk factors for the development of contracture.
Methods
This review was conducted according to the PRISMA guidelines when applicable [8]. The literature search was performed in the PubMed database in March 2020 using the following search terms “Breast AND (implant OR prosthesis OR prostheses OR expander OR capsule OR capsular OR periprosthetic) AND (histology OR immunohistochemistry OR histological)”. Articles were selected based on a priori defined inclusion and exclusion criteria. Studies were included if they reported histological analyses of breast implant capsules. Histological parameters of interest included capsule layers, cellularity, inflammation and capsule thickness. Criteria for exclusion were animal studies or a small study population (less than five patients). Commentaries, discussions, letters, reviews and studies in languages other than English were also excluded. The following study characteristics were extracted: author, year of publication, country of origin, sample size, Baker grading, whether the samples came from patients who had received the implant in cosmetic or reconstructive surgery and time from implantation to collection of samples.
Results
The search identified 4870 articles of which 52 were included in our study. A flowchart of the screening process is shown in Fig. 1. Eleven studies included samples from a median of 19 patients (IQR 10–25 patients) who had undergone cosmetic breast augmentation with implants. Eighteen studies included samples from a median of 16 patients (IQR 10–20 patients) who had undergone implant-based breast reconstruction. Eighteen studies included samples from both cosmetic and reconstructive patients with a median of 33 patients (IQR 15–51 patients) and four studies did not report the patient category. The time from implantation to collection of the samples was reported in 42 studies with a median time of two years (IQR 0.5–7.8 years). In 26 studies, the clinical severity of capsular contracture was assessed with the Baker classification system [7]. Data from the included studies are summarized in Table 1.

Flowchart of the screening process
The Histological Layers of the Capsule
Most studies described the implant capsules as being organized in multiple layers [9,10,11,12,13,14,15,16,17]. Several studies found that the innermost layer at the tissue–implant interface consisted of synovial-like metaplasia. Beyond this layer, several studies found organized layers of loose and dense connective tissue containing the vascular supply of the capsules [9,10,11, 15, 16, 18, 19]. Although several authors describe the multilayered structure of the capsule, there was no consensus on the number of layers or on how the connective tissue was arranged. Most of the included studies described three [15, 19,20,21] or four layers [9,10,11] and one study described five layers [16].
The Layer of Synovial-like Metaplasia
Synovial-like metaplasia was described in more than half of the included studies. The layer of synovial-like metaplasia was reported to consist predominantly of macrophages and fibroblasts and varied from one to several layers of cells [10, 11, 15,16,17, 19,20,21,22,23,24]. Several authors reported that the presence of synovial-like metaplasia decreased over time [9, 25,26,27]. One study by de Bakker et al. [10] suggested an inverse relation between the presence of the layer and the clinical severity of capsular contracture based on samples from 10 patients who had undergone cosmetic augmentation. Two studies found that the layer of synovial-like metaplasia lacked a basement membrane indicating that the layer is of mesenchymal origin [11, 28]. Additionally, several of the included studies suggested that the development of synovial-like metaplasia may be triggered by mechanical stress and silicone leakage [9, 10, 15, 17, 19, 25, 29, 30]. Two of these studies reported that the layer produced lubricating proteoglycans as an adaptive response to friction between the surface of the breast pocket and the implant [9, 28].
The Fibrous Layers
Several studies described that the layers beyond the synovial-like metaplasia predominantly consisted of collagen and fibroblasts [11, 25, 31] and that these layers constituted the majority of the capsule although varying in density and number of collagen layers [32, 33]. Multiple studies found that the collagen fibers in contracted capsules (Baker III/IV) ran parallel to the implant surface with a more uniform alignment compared with uncontracted capsules (Baker I/II) which were described as having more multidirectional and loosely arranged fibers [11, 14, 16, 30, 34,35,36,37,38,39]. A study by Moyer et al. [35] on 14 samples from patients who had undergone breast reconstruction with breast tissue expanders and acellular dermal matrix described the fibers of the implant capsule to be arranged as fine collagen bundles that developed around thicker collagen cables in a coil-like manner. In contracted capsules, they found these fine collagen fibers to condense around the collagen cables. It has been suggested that the alignment and condensation of collagen increase the tensile strength within the capsule tissue [34, 35].
Two studies described an increased cell density at the tissue–implant interface compared with the other layers of the capsule [29, 34]. De Bakker et al. [10] found a higher cell density in Baker IV capsules compared with Baker I capsules based on 20 capsules with a mean time from implantation to sample collection of 13.4 years (SD 5.9). Similarly, Brazin et al. [31] found a greater number of fibroblasts in Baker IV capsules compared with Baker I capsules. However, these results were based on an analyses of 31 capsule samples from patients who had undergone both cosmetic breast augmentation and breast reconstruction with a relatively short time of implantation (range 5–19 months) and the study only included two Baker IV capsules and 12 Baker I capsules.
Thickness and Contractility
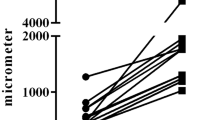
The severity of capsular contracture is thought to be influenced by the capsule thickness and the extent of contracture. The thickness of the implant capsule has been found to vary from 21 µm to 10 mm [24, 29]. Five studies investigating the correlation between capsule thickness and baker grade found that Baker III and IV capsules were significantly thicker than Baker I and II capsules [10, 26, 29, 36, 37]. Furthermore, two studies found that the thickness of the capsule increased over time [26, 29].
The capsule contractility is assumed to be mediated by the contractile properties of myofibroblasts and their attachment to the extracellular collagen. Two of the included studies investigated the relation between the number of myofibroblasts and the severity of capsular contracture [29, 38]. They found more myofibroblasts in contracted capsules than non-contracted capsules based on 59 patients who had primarily undergone cosmetic breast augmentation. Furthermore, Hwang et al. found that the capsule’s tensile strength had a positive correlation with the degree of capsular contracture [38].
Inflammation
Inflammation in the capsule tissue surrounding the breast implants has been described across 12 of the included studies [14, 19, 22,23,24,25,26, 30, 39,40,41,42]. The capsule samples have been found to exhibit both acute, chronic and granulomatous inflammation [19, 22,23,24,25,26, 30, 39, 41, 42]. The type of immune cells described within the capsule tissue include macrophages, histiocytes, mast cells, lymphocytes as well as multinucleated foreign body giant cells [15, 18,19,20, 23, 25, 29, 34, 39, 41, 43,44,45]. A study by Kamel et al. [45] investigated the lymphoid phenotypes of Baker I–IV capsules in 63 patients who had undergone both cosmetic breast augmentation and breast reconstruction. They found an inverse relation between the number of CD3 positive T-cells and CD68 positive macrophages and the progression of collagen deposition [45]. The authors suggested that, with time, the deposition of collagen progressed to fibrosis of the capsular tissue.
Radiotherapy
Previous studies suggest that radiotherapy can increase the risk of capsular contracture [46, 47]. Borrelli et al. [46] found an increased number of fibroblasts in irradiated capsules compared with nonirradiated capsules in 10 patients who underwent unilateral radiotherapy and bilateral breast reconstruction with expander implants. They found that the capsules in the irradiated breasts were significantly thicker than those of the nonirradiated breasts. The organization of collagen was found to be less uniform in the capsules surrounding implants of irradiated breasts compared with nonirradiated capsules. A study by Moyer et al. [48] found more macrophages in irradiated capsules compared with nonirradiated capsules based on six patients who underwent bilateral tissue expander reconstruction with acellular dermal matrix. This suggests that radiotherapy causes inflammation which may be why irradiated breasts are more prone to capsular contracture. See Table 2 for an overview of histological findings associated with clinical risk factors for capsular contracture.
Implant Surface Texture
The surface pores on textured implant shells are thought to induce a multidirectional orientation of the collagenous fibers, restrict the contractive potential of the fibrous capsule and thereby minimize the risk of capsular contracture [16, 49, 50]. Three studies investigated the capsule thickness in smooth and textured implants and found no difference in a total of 80 patients [29, 38, 51]. Kuriyama et al. [52] found a significant increase in the presence of myofibroblasts in the capsule surrounding smooth implants compared with textured implants in capsule samples from 10 patients who had undergone breast reconstruction.
Silicone Leakage
Silicone leakage has been investigated by numerous studies as a possible trigger of capsular contracture. Several of the included studies found silicone both intracellularly in macrophages and as free droplets in the tissue [11, 14, 17, 19,20,21, 24,25,26, 39, 44, 45, 53]. Most of these studies reported localized inflammatory response around the silicone droplets with infiltrates of giant cells and macrophages [11, 17,18,19, 21, 22, 24, 44, 53]. A study by Siggelkow et al. [26] found an association between the amount of silicone droplets and the thickness of the capsule tissue based on 13 patients who had undergone both cosmetic breast augmentation and breast reconstruction, but they did not find an association between amount of silicone droplets and severity of capsular contracture graded with the Baker score.
Acellular Dermal Matrix
Acellular dermal matrix (ADM) has been proposed to have a protective effect on the development of capsular contracture [39, 43, 45]. Several of the included studies collected biopsies from the ADM as well as biopsies from the native capsule. The ADM biopsies exhibited both synovial-like metaplasia and layers of connective tissue similar to the native capsule [54,55,56] but showed a significant decrease in blood vessel proliferation, fibroblast activity, collagen deposition as well as less capsular fibrosis compared with the native capsules from the same patients [46, 48, 56,57,58,59]. Some of the studies reported that the use of ADM significantly decreased the inflammatory response and suggested that ADM may have a role in slowing the process of capsule formation [48, 54, 56, 57, 60, 61].
Discussion
In this systematic review, we evaluated the histological characteristics of capsular contracture to investigate clinical risk factors associated with capsular contracture. Based on previous studies, it is evident that radiotherapy induces tissue damage with an increase in inflammation, fibrosis and collagen deposition which leads to a thicker capsule. However, it is still unknown whether the capsule contraction induced by radiotherapy is similar to the capsular contracture that develops in a nonirradiated breast or if the cellular mechanisms involved are different from one another.
The use of textured implants is thought to decrease the risk of capsular contracture. The studies included in this review did not find a distinct histological difference when comparing capsules surrounding textured implants and smooth implants. Recently, textured implants and macrotextured implants in particular have been associated with an increased incidence of breast implant-associated anaplastic large cell lymphoma (BIA-ALCL) [62]. Due to the rarity of BIA-ALCL, the evidence is inconclusive, and there is an ongoing debate about the use of textured implants and their role in the pathogenesis of BIA-ALCL [63].
The presence of synovial-like metaplasia was another interesting finding of this review. The included studies suggested that the layer acts as a protective barrier against the frictional forces within the breast pocket, thereby reducing the risk of capsular contracture. The presence of the layer was found to decrease as the time of implantation prolonged as well as with higher Baker grading. De Bakker et al. hypothesized that the layer is lost due to the increasing thickness of the capsule and consequently loss of nutrition to the synovial-like metaplasia [10]. We hypothesize that the inconsistency of the layer could be due to a strong adhesion between the implant surface and the capsule. This adhesion has been described as a “Velcro-effect” [64, 65], and it might result in the synovial-like metaplasia being torn off during implant removal. Future studies on synovial-like metaplasia are encouraged to further investigate the correlation between the layer and capsular contracture.
ADM was also suggested to have a protective effect against capsular contracture in implant-based breast reconstruction. Several of the included studies reported of a decrease in both inflammation and vascularization in the ADM samples compared with samples from the native capsule. Similarly, reduced inflammation and vascularization are thought to reduce scar formation why these findings indicate that ADM may have a role in slowing the process of capsule formation.
Investigating the pathogenesis of capsular contracture is challenging for several reasons. Capsular contracture is a continuous process that can develop in a wide timespan from a few months up to several years after insertion of the implant [66]. In order to characterize the morphological changes of the implant capsule over time, it is necessary to include biopsies with great variation in the time from implantation to sample collection. The studies included in this review have a median time of implantation of 1.4 years (IQR 0.5–7.1 years) which limits the ability of the studies to draw conclusions on the time of implantation as a contributing factor to capsular contracture. Furthermore, the included samples represent a single moment in time of a continues process. It is therefore unknown whether an uncontracted capsule represents a healthy control sample or an early stage in the development toward capsular contracture. Most of the included studies are unable to conclude on a causal relationship between the histologic morphology and capsular contracture due to their study design (e.g., case–control studies).
Another challenge when investigating the pathogenesis of capsular contracture is the lack of a validated clinical grading system. A grading of the severity of capsular contraction is necessary in order to investigate the differences between a contracted capsule and a non-contracted capsule. The Baker classification system is often used to determine the severity of capsular but only 26 (50%) of the included studies reported on Baker grades. It is generally recognized that the Baker grading system is limited by the subjective assessment when determining the grade resulting in a user-dependent score [67,68,69]. Currently, no validated objective measurement of the degree of contracture exists.
Most of the included studies have a descriptive approach to their investigation and a relatively small samples size with a median sample size of 19 included patients. While the studies provide a detailed description of capsule histology, larger sample sizes are required to perform quantitative analyses to identify the differences between contracted and non-contracted capsules. The lack of quantitative analyses impairs synthetization of data across studies in a meta-analysis. Additionally, the included studies are generally composed of a heterogenous patient population with samples from patients who had undergone cosmetic augmentation as well as breast reconstruction after breast cancer including both expander implants and permanent implants. Furthermore, the location from where the biopsy was obtained is often not standardized or mentioned in the studies. Further studies are needed that account for these limitations to investigate the pathogenesis of capsular contracture.
References
Spear SL, Murphy DK (2014) Allergan silicone breast implant U.S. Core clinical study group. Natrelle round silicone breast implants: Core study results at 10 years. Plast Reconstr Surg 133. https://doi.org/10.1097/PRS.0000000000000021
Blount AL, Martin MD, Lineberry KD, Kettaneh N, Alfonso DR (2013) Capsular contracture rate in a low-risk population after primary augmentation mammaplasty. Aesthetic Surg J 33(4):516–521. https://doi.org/10.1177/1090820X13484465
Stutman RL, Codner M, Mahoney A, Amei A (2012) Comparison of breast augmentation incisions and common complications. Aesthetic Plast Surg 36(5):1096–1104. https://doi.org/10.1007/s00266-012-9918-x
Codner MA, Mejia JD, Locke MB et al (2011) A 15-year experience with primary breast augmentation. Plast Reconstr Surg 127(3):1300–1310. https://doi.org/10.1097/PRS.0b013e318205f41b
Sevin A, Sevin K, Senen D, Deren O, Adanali G, Erdogan B (2006) Augmentation mammaplasty: retrospective analysis of 210 cases. Aesthetic Plast Surg 30(6):651–654. https://doi.org/10.1007/s00266-006-0076-x
Gutowski KA, Mesna GT, Cunningham BL (1997) Saline-filled breast implants: a plastic surgery educational foundation multicenter outcomes study. Plastic Reconstr Surg 100(4):1019–1027
Spear SL, Baker JL, Coffee HH (1995) Classification of capsular contracture after prosthetic breast reconstruction. Plast Reconstr Surg 96(5):1124. https://doi.org/10.1097/00006534-199510000-00019
Liberati A, Altman DG, Tetzlaff J et al (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ital J Public Health. 6(4):354–391. https://doi.org/10.1371/journal.pmed.1000100.t004
Cheriyan T, Guo L, Orgill DP, Padera RF, Schmid TM, Spector M (2012) Lubricin in human breast tissue expander capsules. J Biomed Mater Res B Appl Biomater 100B(7):1961–1969. https://doi.org/10.1002/jbm.b.32763
de Bakker E, van den Broek LJ, Ritt MJPF, Gibbs S, Niessen FB (2018) The histological composition of capsular contracture focussed on the inner layer of the capsule: an intra-donor Baker-I versus Baker-IV comparison. Aesthetic Plast Surg 42(6):1485–1491. https://doi.org/10.1007/s00266-018-1211-1
del Rosario AD, Bui HX, Petrocine S et al (1995) True synovial metaplasia of breast implant capsules: a light and electron microscopic study. Ultrastruct Pathol 19(2):83–93. https://doi.org/10.3109/01913129509014607
Hansen TC, Woeller CF, Lacy SH, Koltz PF, Langstein HN, Phipps RP (2017) Thy1 (CD90) expression is elevated in radiation-induced periprosthetic capsular contracture: implication for novel therapeutics. Plast Reconstr Surg 140(2):316–326. https://doi.org/10.1097/PRS.0000000000003542
Hunter LW, Lieske JC, Tran NV, Miller VM (2011) The association of matrix Gla protein isomers with calcification in capsules surrounding silicone breast implants. Biomaterials 32(33):8364–8373. https://doi.org/10.1016/j.biomaterials.2011.07.073
Šmahel J (1979) Foreign material in the capsules around breast prostheses and the cellular reaction to it. Br J Plast Surg 32(1):35–42. https://doi.org/10.1016/0007-1226(79)90058-4
Wolfram D, Rainer C, Niederegger H, Piza H, Wick G (2004) Cellular and molecular composition of fibrous capsules formed around silicone breast implants with special focus on local immune reactions. J Autoimmun 23(1):81–91
Rubino C, Mazzarello V, Farace F et al (2001) Ultrastructural anatomy of contracted capsules around textured implants in augmented breasts. Ann Plast Surg 46(2):95–102. https://doi.org/10.1097/00000637-200102000-00001
Emery JA, Spanier SS, Kasnic G, Hardt NS (1994) The synovial structure of breast-implant-associated bursae. Mod Pathol 7(7):728–733
Kasper CS (1994) Histologic features of breast capsules reflect surface configuration and composition of silicone bag implants. Am J Clin Pathol 102(5):655–659. https://doi.org/10.1093/ajcp/102.5.655
Yeoh G, Russell P, Jenkins E (1996) Spectrum of histological changes reactive to prosthetic breast implants: a clinopathological study of 84 patients. Pathology 28(3):232–235. https://doi.org/10.1080/00313029600169044
Lam MC, Walgenbach-Brünagel G, Pryalukhin A et al (2019) Management of capsular contracture in cases of silicone gel breast implant rupture with use of pulse lavage and open capsulotomy. Aesthetic Plast Surg 43(5):1173–1185. https://doi.org/10.1007/s00266-019-01463-w
Legrand AP, Marinov G, Pavlov S et al (2005) Degenerative mineralization in the fibrous capsule of silicone breast implants. J Mater Sci Mater Med 16(5):477–485. https://doi.org/10.1007/s10856-005-6989-0
Luke JL, Kalasinsky VF, Turnicky RP, Centeno JA, Johnson FB, Mullick FG (1997) Pathological and biophysical findings associated with silicone breast implants: a study of capsular tissues from 86 cases. Plast Reconstr Surg 100(6):1558–1565. https://doi.org/10.1097/00006534-199711000-00029
Hameed MR, Erlandson R, Rosen PP (1995) Capsular synovial-like hyperplasia around mammary implants similar to detritic synovitis: a morphologic and immunohistochemical study of 15 cases. Am J Surg Pathol 19(4):433–438. https://doi.org/10.1097/00000478-199504000-00004
Prantl L, Schreml S, Fichtner-Feigl S et al (2007) Clinical and morphological conditions in capsular contracture formed around silicone breast implants. Plast Reconstr Surg 120(1):275–284. https://doi.org/10.1097/01.prs.0000264398.85652.9a
Ko CY, Ahn CY, Ko J, Chopra W, Shaw WW (1996) Capsular synovial metaplasia as a common response to both textured and smooth implants. Plast Reconstr Surg 97(7):1427–1433. https://doi.org/10.1097/00006534-199606000-00017
Siggelkow W, Faridi A, Spiritus K, Klinge U, Rath W, Klosterhalfen B (2003) Histological analysis of silicone breast implant capsules and correlation with capsular contracture. Biomaterials 24(6):1101–1109. https://doi.org/10.1016/S0142-9612(02)00429-5
Wyatt LE, Sinow JD, Wollman JS, Sami DA, Miller TA (1998) The influence of time on human breast capsule histology: smooth and textured silicone-surfaced implants. Plast Reconstr Surg 102(6):1922–1931. https://doi.org/10.1097/00006534-199811000-00017
Raso DS, Schulte BA (1996) Immunolocalization of keratan sulfate, chondroitin-4-sulfate, and chondroitin-6-sulfate in periprosthetic breast capsules exhibiting synovial metaplasia. Plast Reconstr Surg 98(1):78–82. https://doi.org/10.1097/00006534-199607000-00012
Bui JM, Perry TA, Ren CD, Nofrey B, Teitelbaum S, Van Epps DE (2015) Histological characterization of human breast implant capsules. Aesthetic Plast Surg 39(3):306–315. https://doi.org/10.1007/s00266-014-0439-7
Bassetto F, Scarpa C, Caccialanza E, Montesco MC, Magnani P (2010) Histological features of periprosthetic mammary capsules: silicone vs. polyurethane. Aesthetic Plast Surg 34(4):481–485. https://doi.org/10.1007/s00266-010-9483-0
Brazin J, Malliaris S, Groh B et al (2014) Mast cells in the periprosthetic breast capsule. Aesthetic Plast Surg 38(3):592–601. https://doi.org/10.1007/s00266-014-0318-2
Coleman DJ, Sharpe DT, Naylor IL, Chander CL, Cross SE (1993) The role of the contractile fibroblast in the capsules around tissue expanders and implants. Br J Plast Surg 46(7):547–556. https://doi.org/10.1016/0007-1226(93)90104-J
Poh PSP, Schmauss V, McGovern JA et al (2018) Non-linear optical microscopy and histological analysis of collagen, elastin and lysyl oxidase expression in breast capsular contracture. Eur J Med Res 23(1). https://doi.org/10.1186/s40001-018-0322-0
Bosetti M, Navone R, Rizzo E, Cannas M (1998) Histochemical and morphometric observations on the new tissue formed around mammary expanders coated with pyrolytic carbon. J Biomed Mater Res 40(2):307–313. https://doi.org/10.1002/(SICI)1097-4636(199805)40:2%3c307::AID-JBM16%3e3.0.CO;2-I
Moyer KE, Ehrlich HP (2013) Capsular contracture after breast reconstruction: collagen fiber orientation and organization. Plast Reconstr Surg 131(4):680–685. https://doi.org/10.1097/PRS.0b013e31828189d0
Ersek RA, Burroughs JR, Ersek CL, Navarro A (1991) Interrelationship of capsule thickness and breast hardness confirmed by a new measurement method. Plast Reconstr Surg 87(6):1069–1073. https://doi.org/10.1097/00006534-199106000-00008
Prantl L, Pöppl N, Horvat N, Heine N, Eisenmann-Klein M (2005) Serologic and histologic findings in patients with capsular contracture after breast augmentation with smooth silicone gel implants: is serum hyaluronan a potential predictor? Aesthetic Plast Surg 29(6):510–518. https://doi.org/10.1007/s00266-005-5049-y
Hwang K, Sim HB, Huan F, Kim DJ (2010) Myofibroblasts and capsular tissue tension in breast capsular contracture. Aesthetic Plast Surg 34(6):716–721. https://doi.org/10.1007/s00266-010-9532-8
Carpaneda CA (1997) Inflammatory reaction and capsular contracture around smooth silicone implants. Aesthetic Plast Surg 21(2):110–114. https://doi.org/10.1007/s002669900094
Smahel J (1978) Fibrous reactions in the tissues which surround silicone breast prostheses. Br J Plast Surg 31(3):250–253. https://doi.org/10.1016/0007-1226(78)90095-4
Šmahel J (1977) Histology of the capsules causing constrictive fibrosis around breast implants. Br J Plast Surg 30(4):324–329. https://doi.org/10.1016/0007-1226(77)90132-1
Prantl L, Angele P, Schreml S, Ulrich D, Pöppl N, Eisenmann-Klein M (2006) Determination of serum fibrosis indexes in patients with capsular contracture after augmentation with smooth silicone gel implants. Plast Reconstr Surg 118(1):224–229. https://doi.org/10.1097/01.prs.0000220462.28928.83
Wolfram D, Rabensteiner E, Grundtman C, Böck G, Mayerl C, Parson W et al (2012) T regulatory cells and TH17 cells in peri–silicone implant capsular fibrosis. Plastic Reconstr Surg 129(2):327e–337e. https://doi.org/10.1097/PRS.0b013e31823aeacf
Efanov JI, Giot JP, Fernandez J, Danino MA (2017) Breast-implant texturing associated with delamination of capsular layers: a histological analysis of the double capsule phenomenon. Ann Chir Plast Esthet 62(3):196–201. https://doi.org/10.1016/j.anplas.2017.02.001
Kamel M, Protzner K, Fornasier V, Peters W, Smith D, Ibanez D (2001) The peri-implant breast capsule: an immunophenotypic study of capsules taken at explantation surgery. J Biomed Mater Res 58(1):88–96. https://doi.org/10.1002/1097-4636(2001)58:1%3c88::AID-JBM130%3e3.0.CO;2-7
Borrelli MR, Irizzary D, Patel RA et al (2020) Pro-Fibrotic CD26-Positive fibroblasts are present in greater abundance in breast capsule tissue of irradiated bBreasts. Aesthetic Surg J 40(4):369–379. https://doi.org/10.1093/asj/sjz109
Lipa JE, Qiu W, Huang N, Alman BA, Pang CY (2010) Pathogenesis of radiation-induced capsular contracture in tissue expander and implant breast reconstruction. Plast Reconstr Surg 125(2):437–445. https://doi.org/10.1097/PRS.0b013e3181c82d05
Moyer HR, Pinell-White X, Losken A (2014) The effect of radiation on acellular dermal matrix and capsule formation in breast reconstruction: clinical outcomes and histologic analysis. Plast Reconstr Surg 133(2):214–221. https://doi.org/10.1097/01.prs.0000437255.01199.42
Abramo AC, De Oliveira VR, Ledo-Silva MC, De Oliveira EL (2010) How texture-inducing contraction vectors affect the fibrous capsule shrinkage around breasts implants? Aesthetic Plast Surg 34(5):555–560. https://doi.org/10.1007/s00266-010-9495-9
Wickman M, Johansson O, Olenitis M, Forslind B (1993) A comparison of the capsules around smooth and textured silicone prostheses used for breast reconstruction a light and electron microscopic study. Scand J Plast Reconstr Surg Hand Surg 27(1):15–22. https://doi.org/10.3109/02844319309080286
Thuesen B, Siim E, Christensen L, Schrøder M (1995) Capsular contracture after breast reconstruction with the tissue expansion technique: a comparison of smooth and textured silicone breast prostheses. Scand J Plast Reconstr Surg Hand Surg 29(1):9–13. https://doi.org/10.3109/02844319509048417
Kuriyama E, Ochiai H, Inoue Y et al (2017) Characterization of the capsule surrounding smooth and textured tissue expanders and correlation with contracture. Plast Reconstr Surg Glob Open 5(7). https://doi.org/10.1097/GOX.0000000000001403
Lesesne CB (1997) Textured surface silicone breast implants: histology in the human. Aesthetic Plast Surg 21(2):93–96. https://doi.org/10.1007/s002669900091
Boháč M, Danišovič Ľ, Koller J, Dragúňová J, Varga I (2018) What happens to an acellular dermal matrix after implantation in the human body? A histological and electron microscopic study. Eur J Histochem 62(1):1–11. https://doi.org/10.4081/ejh.2018.2873
Hansson E, Burian P, Hallberg H (2020) Comparison of inflammatory response and synovial metaplasia in immediate breast reconstruction with a synthetic and a biological mesh: a randomized controlled clinical trial. J Plast Surg Hand Surg 54(3):131–136. https://doi.org/10.1080/2000656X.2019.1704766
Basu CB, Leong M, Hicks MJ (2010) Acellular cadaveric dermis decreases the inflammatory response in capsule formation in reconstructive breast surgery. Plast Reconstr Surg 126(6):1842–1847. https://doi.org/10.1097/PRS.0b013e3181f44674
Leong M, Basu CB, Hicks MJ (2015) Further evidence that human acellular dermal matrix decreases inflammatory markers of capsule formation in implant-based breast reconstruction. Aesthetic Surg J 35(1):40–47. https://doi.org/10.1093/asj/sju014
Tevlin R, Borrelli MR, Irizarry D, Nguyen D, Wan DC, Momeni A (2019) Acellular dermal matrix reduces myofibroblast presence in the breast capsule. Plast Reconstr Surg - Glob Open. 7(5):e2213. https://doi.org/10.1097/gox.0000000000002213
Bohac M, Varga I, Polak S, Dragunova J, Fedeles J, Koller J (2018) Delayed post mastectomy breast reconstructions with allogeneic acellular dermal matrix prepared by a new decellularizationmethod. Cell Tissue Bank 19(1):61–68. https://doi.org/10.1007/s10561-017-9655-0
Moyer HR, Hart AM, Yeager J, Losken A (2017) A histological comparison of two human acellular dermal matrix products in prosthetic-based breast reconstruction. Plast Reconstr Surg Glob Open 5(12). https://doi.org/10.1097/GOX.0000000000001576
Poppler L, Cohen J, Dolen UC et al (2015) Histologic, molecular, and clinical evaluation of explanted breast postheses, capsules, and acellular dermal matrices for bacteria. Aesthetic Surg J 35(6):653–668. https://doi.org/10.1093/asj/sjv017
Magnusson M, Beath K, Cooter R et al (2019) The epidemiology of breast implant-associated anaplastic large cell lymphoma in Australia and New Zealand confirms the highest risk for Grade 4 Surface breast implants. Plast Reconstr Surg 143(5):1285–1292. https://doi.org/10.1097/PRS.0000000000005500
U.S. Food and Drug Administration (2019) Medical device reports of breast implant-associated anaplastic large cell ymphoma. https://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/ImplantsandProsthetics/BreastImplants/ucm481899.htm. Accessed 7 Apr 2021
Danino AM, Basmacioglu P, Saito S et al (2001) Comparison of the capsular response to the biocell RTV and mentor 1600 siltex breast implant surface texturing: a scanning electron microscopic study. Plast Reconstr Surg 108(7):2047–2052. https://doi.org/10.1097/00006534-200112000-00032
Giot JP, Paek LS, Nizard N, El-Diwany M, Gaboury LA, Nelea M et al (2015) The double capsules in macro-textured breast implants. Biomaterials 67:65–72. https://doi.org/10.1016/j.biomaterials.2015.06.010
Zeplin PH, Corduff N (2015) Influence of patient age on capsular contracture after aesthetic breast augmentation. Can J Plast Surg 23(2):67–69. https://doi.org/10.1177/229255031502300209
de Bakker E, Rots M, Buncamper ME, Niessen FB, Smit JM, Winters HA et al (2020) The Baker classification for capsular contracture in breast implant surgery is unreliable as a diagnostic tool. Plastic Reconstr Surg 146(5):956–962. https://doi.org/10.1097/PRS.0000000000007238
Zahavi A, Sklair ML, Ad-El DD (2006) Capsular contracture of the breast: working towards a better classification using clinical and radiologic assessment. Ann Plast Surg 57(3):248–251. https://doi.org/10.1097/01.sap.0000221614.32176.9a
Embrey M, Adams EE, Cunningham B, Peters W, Young VL, Carlo GL (1999) A review of the literature on the etiology of capsular contracture and a pilot study to determine the outcome of capsular contracture interventions. Aesthetic Plast Surg 23(3):197–206. https://doi.org/10.1007/s002669900268
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest to disclose.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, informed consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Larsen, A., Rasmussen, L.E., Rasmussen, L.F. et al. Histological Analyses of Capsular Contracture and Associated Risk Factors: A Systematic Review. Aesth Plast Surg 45, 2714–2728 (2021). https://doi.org/10.1007/s00266-021-02473-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-021-02473-3