
Abstract
Background
Periprosthetic capsules are a common reaction of the body to silicone or polyurethane breast implants. The aim of this study was to evaluate similarities and differences in the histological features of periprosthetic capsules surrounding silicone implants and polyurethane foam-coated implants and to correlate those features with the age of the implants.
Methods
Tissues were studied from 41 periprosthetic capsules surrounding textured prostheses and from 20 capsules surrounding polyurethane foam-coated implants. For each sample we evaluated synovial metaplasia, density of collagen fibers or fibrosis, orientation of collagen fibers, and foreign body reaction (granulomatous reaction).
Results
Synovial metaplasia was seen in the capsular tissue from both types of implant, but more so from capsules surrounding polyurethane implants more than 5 years old. The density and orientation of the collagen fibers and the foreign body reaction were very similar for the two types of implant.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
In the last 50 years many authors have studied periprosthetic capsule formation around implants used in aesthetic and/or cancer-related breast surgery, with a view to ascertaining the biocompatibility of different types of breast prosthesis and whether their chemical and physical features, and the age of the implants, might influence the physiological reaction to the prostheses. Some studies [1–9] demonstrated a strong relationship between the age of the implant and the histological features of the capsule, e.g., synovial metaplasia, foreign body reaction (the presence of granulomatous tissue), and the orientation of the connective fibers.
Using histological methods, we analyzed the anatomical substrate of the breast capsule to establish whether there is any relationship between the features of the capsule and the surface of the prosthesis (textured or polyurethane foam) or the age of the implant.
Materials and Methods
We studied 41 samples of periprosthetic capsule tissue surrounding textured breast implants (McGhan-open pore) and 20 samples of such tissue surrounding polyurethane foam-coated implants. The age of the implants ranged from 3 months to 16 years (mean = 97.5 months). In the majority of cases, the patients (aged 30–60 years) had surgery because of breast cancer.
Each sample was fixed in 10% buffered formalin and embedded in paraffin. Five-micron sections were stained with hematoxylin and eosin. The sections were analyzed by light microscopy to assess features such as synovial metaplasia, density of collagen fibers or fibrosis, and orientation of connective bands.
Synovial Metaplasia
In accordance with Raso et al. [10, 11] (Fig. 1), we defined synovial metaplasia as a proliferation of synovia-like cells arranged in a palisade manner in the interface between capsule and implant. The cells had round to oval nuclei and an abundant eosinophilic cytoplasm. Multinucleated forms were also found. This membrane may be everted on the capsular surface, giving rise to villous hyperplasia. We adopted a semiquantitative method or categorization, i.e., (−): no synovial metaplasia; (+): synovial metaplasia in one third of the capsular surface; (++): synovial metaplasia in more than one third but not all of the capsular surface; and (+++): synovial metaplasia covering the entire capsular surface and/or evidence of villous hyperplasia.

Synovial metaplasia
Fibrosis
We assessed the density of the collagen fibers and whether their orientation was parallel or perpendicular to the implant surface (Fig. 2). We adopted a semiquantitative method of categorization: (−/+): no or sparse collagen fibers; (++): a moderate presence of collagen fibers; and (+++): a continuous, thick layer of collagen fibers.

Capsular fibrosis: parallel connective fiber orientation
Foreign Body Reaction (Granulomatous Reaction)
This was described as absent or present. We classified this reaction as (1) silicone-type granulomata (Fig. 3) if there were optically empty vacuoles due to loss of material after sample preparation, or (2) foreign body granulomata (Fig. 4).

Silicone-type granuloma and histiocytes

Foreign body granuloma showing giant multinucleated cells (white arrow) and crystalline amorphous material (yellow arrow)
Results
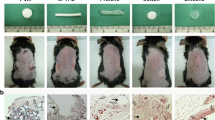
Synovial metaplasia was identified in the capsules surrounding both types of implant, and its presence was greater in polyurethane capsules that were more than 5 years old (Fig. 5). With respect to fibrosis, there were no apparent differences between the capsules surrounding the two types of prosthesis. In both types of sample, fibrosis tended to be greater for prostheses that were more than 5 years old (Fig. 6). There were no apparent differences in orientation of collagen bands. Their orientation was parallel for both silicone textured prostheses and polyurethane foam-coated prostheses (Fig. 7). Foreign body reaction (granulomatous tissue) was evident in both samples; foreign body reaction is a constant finding in polyurethane foam-coated implants (Fig. 8).

Synovial metaplasia and age of implant

Density of collagen fibers and age of implant

Orientation of collagen bands and age of implant

Foreign body reaction and age of implant
Discussion
Synovial Metaplasia
In the last 30 years, synovial metaplasia has come to be seen as a typical feature of prosthetic breast capsules, and in young capsules in particular. Authors like Chase et al. [3], Copeland et al. [12], Raso et al. [10, 11], Del Rosario et al. [4], and Wyatt et al. [8] noted that this histological feature was more evident in textured and polyurethane prostheses. In 1994, Chase et al. [3] correlated synovial metaplasia with the age of the implant, reporting that it decreased as the age of the implant increased. Ko et al. [7] and Wyatt et al. [8] confirmed this correlation. At the time, synovial metaplasia was seen as having a protective effect against capsular contracture thanks to a biofilm produced by the capsular synovial cell layer at the interface with the implant and consisting of chondroitin 4 sulfate and keratin sulfate.
Using logistic regression, Ko et al. [7] found no correlation between the synovial metaplasia and the chemical and physical features of the implant’s surface, hypothesizing that a mechanical stress exerted by the implant on the surrounding tissues could be responsible for the synovial metaplasia. In 2007, Poeppl et al. [13] confirmed this theory when they compared the capsules surrounding smooth silicone implants with those surrounding textured silicone implants.
In our study, we found synovial metaplasia in the capsules surrounding both silicone and polyurethane implants. The greater expression of synovial metaplasia with polyurethane prostheses that were more than 5 years old could be explained by the fact that polyurethane implants are in fact silicone implants covered with polyurethane foam. This extra surface coating could give rise to metaplasia induced first by the polyurethane outer layer, which takes almost 2 years to disappear [14], and later by the inner silicone shell. The greater expression of synovial metaplasia with polyurethane prostheses supports the idea that polyurethane has a protective role against capsular contracture after long periods of time, giving the breast a more natural shape and tenderness. As Handel noted in 1995 [6], silicone-textured prostheses could only reduce capsular contracture in the short term.
Fibrosis
As Giachero described in 1992 [15], so too in our study, changes in the density of the collagen fibers, or fibrosis, is a common feature of both silicone and polyurethane implants that increases with the age of the prostheses, replacing the inflammatory reaction.
Orientation of Collagen Bands
Most studies [1, 2, 5] have described a random or multidirectional orientation of the collagen bands associated with textured and polyurethane prostheses. In 1998, Wyatt et al. [8] noted that the orientation was parallel in 75% of young capsules from textured implants. We confirmed this feature in almost all of our samples, hypothesizing that the mammary massage common in some patients after surgery for breast cancer could cause a separation between the capsules and the textured surface of the implant, with a consequent straightening of the connective fibers.
Foreign Body Reaction
Chase et al. [3], Raso et al. [10, 11], and Wyatt et al. [8] all described foreign body reaction as increasing with the age of the implant. In our study, however, foreign body reaction was commonly seen with both types of implant but its presence remained stable or increased only in the polyurethane implant-induced capsules. We hypothesized a breakdown of the double coating on the implants, i.e., first of the superficial sheet of polyurethane foam and subsequently of the underlying sheet of silicone, as the reason for this finding.
Conclusions
This histological study identified much the same situation for the two types of implants, the most important difference being that synovial metaplasia was more evident in polyurethane foam-coated implants. This feature might be of considerable importance because synovial metaplasia is the most important protective factor against capsular contracture.
References
Brand KG (1984) Polyurethane-coated silicone implants and the question of capsular contracture. Plast Reconstr Surg 73(3):498
Bucky LP, Ehrlich HP, Sohoni S, May JW Jr (1994) The capsule quality of saline-filled smooth silicone, textured silicone, and polyurethane implants in rabbits: a long-term study. Plast Reconstr Surg 93(6):1123–1131 discussion 1132-1133
Chase DR, Oberg KC, Chase RL, Malott RL, Weeks DA (1994) Pseudoepithelialization of breast implant capsules. Int J Surg Pathol 1(3):151–154
Del Rosario AD, Bui HX, Petrocine S, Sheehan C, Pastore J, Singh J, Ross JS (1995) True synovial metaplasia of breast implant capsules: a light and electron microscopic study. Ultrastruct Pathol 19(2):83–93
Batra M, Bernard S, Picha G (1995) Histologic comparison of breast implant shells with smooth, foam, and pillar microstructuring in a rat model from 1 day to 6 months. Plast Reconstr Surg 95(2):354–363
Handel N, Jensen JA, Black Q, Waisman JR, Silverstein MJ (1995) The fate of breast implants: a critical analysis of complications and outcomes. Plast Reconstr Surg 96(7):1521–1533
Ko CY, Ahn CY, Ko J, Chopra W, Shaw WW (1996) Capsular synovial metaplasia as a common response to both textured and smooth implants. Plast Reconstr Surg 97(7):1427–1433 discussion 1434-1435
Wyatt LE, Sinow JD, Wollman JS, Sami DA, Miller TA (1998) The influence of time on human breast capsule histology: smooth and textured silicone surfaced implants. Plast Reconstr Surg 102(6):1922–1931
Siggelkow W, Faridi A, Spiritus K, Klinge U, Rath W, Klosterhalfen B (2003) Histological analysis of silicone breast implant capsule and correlation with capsular contracture. Biomaterials 24(6):1101–1109
Raso DS, Greene WB, Metcalf JS (1994) Synovial metaplasia of a periprosthetic breast capsule. Arch Pathol Lab Med 118(3):249–251
Raso DS, Greene WB (1995) Synovial metaplasia of a periprosthetic breast capsule surrounding a polyurethane foam breast prosthesis. Ann Plast Surg 35(2):201–203
Copeland M, Choi M, Bleiweiss IJ (1994) Silicone breakdown and capsular synovial metaplasia in textured-wall saline breast prostheses. Plast Reconstr Surg 94(5):628–633 discussion 634-636
Poeppl N, Schreml S, Lichtenegger F, Lenich A, Eisenmann-Klein M, Prantl L (2007) Does the surface structure of implants have an impact on the formation of a capsular contracture? Aesthetic Plast Surg 31(2):133–139
Hester T Jr, Ford NF, Gale PJ, Hammett JL, Raymond R, Turnbull D, Frankos VH, Cohen MB (1997) Measurement of 2,4-toluenediamine in urine and serum samples from women with Même or Replicon breast implants. Plast Reconstr Surg 100:1291–1298
Giachero E (1992) Materiali sintetici in chirurgia plastica, Ed. Cortina
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bassetto, F., Scarpa, C., Caccialanza, E. et al. Histological Features of Periprosthetic Mammary Capsules: Silicone vs. Polyurethane. Aesth Plast Surg 34, 481–485 (2010). https://doi.org/10.1007/s00266-010-9483-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-010-9483-0