
Abstract
Purpose
Pavlik harness treatment is the most common treatment in newborns diagnosed with developmental dysplasia of the hip (DDH). The success rates and predictors for failure have been debated over the last decade. In this study, we explored our treatment failure rate and potential prognostic factors that could predict the failure of Pavlik harness (PH) treatment in patients with DDH.
Methods
Two hundred and sixty-five patients were treated with PH based on the Graf hip types of classification. Age, gender, first born status, family history, foot deformity, plagiocephaly, breech presentation, hip abduction, hip stability, Graf hip type, Galeazzi sign, bilateralism, and femoral nerve palsy were tested as predictors for failure in multivariate logistic regression mode. Success and failure were determined by the normalization of the hip based on the Graf hip classification.
Results
The failure rate of patients treated with Pavlik harness was 16.6% which is within the reported range of failure rate. The mean age of patients who were successfully treated was 6.73 weeks in comparison to 8.84 weeks for those who failed. Age, plagiocephaly, hip instability, Graf classification, and the development of femoral nerve palsy were found to be predictors for failure of PH treatment upon univariate analysis only. However, only the presence of Galeazzi sign, hip instability, high grades of Graf hip classification, and the development of femoral nerve palsy proved to be independent predictors for failed PH treatment upon multivariate logistic regression analysis.
Conclusions
Pavlik harness treatment is a successful treatment with an average success of 83.4%. Several independent predictors for failure of PH treatment have been identified. These include a positive Galeazzi sign, a frankly dislocated hip, Graf types III and IV, and the development of femoral nerve palsy.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Developmental dysplasia of the hip (DDH) involves a range of disorders that represent an abnormal relationship between the head of the femur and the acetabulum leading to abnormal development of the hip joint [1,2,3]. Current and previous data allude to an estimate of DDH that ranges from one to eight cases per 1000 live births revealed by physical examination which escalates up to one to three in 100 live births revealed by sonographic screening [3,4,5].
Several risk factors have been implicated with the cause of the DDH including first born status, female gender, family history, fetal malposition (particularly extended breech presentation), fetal packaging disorders (congenital torticollis and metatarsus adductus), and some geographical and racial factors (more common in native American and European than Asian and African). Two meta-analyses of over a million babies showed that the main independent risk factors are breech presentation, female gender, and family history [6, 7].
Screening practices include a detailed history and clinical examination by assessing infants for limb discrepancy and thigh fold symmetry, as well as any limitations in hip abduction [4]. Diagnosis is confirmed by ultrasound examination using either Graf, Harcke, Terjesen, or Suzuki methods [8, 9]. The quantitative classification of Graf is the most commonly utilized method (Table1) [10].
Pavlik harness (PH) treatment is one of the most used treatment methods for DDH in infants younger than six months yielding a 70–90% success rate [1, 11,12,13,14]. PH aims to relocate the hip to the normal anatomical position in a non-invasive fashion [15,16,17] [10] (Fig. 1).

Child treated with a Pavlik harness
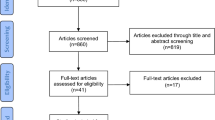
We conducted a systematic review of the studies that used PH treatment, and we identified 15 studies that investigated the Pavlik harness treatment in DDH [16, 18,19,20,21,22,23,24,25,26,27,28,29,30,31]. Seven studies investigated studies that reported a failure rate that ranged from 3.3 to 40% (crude mean is 11.6%) [11] (Table 2). Graf type IV hips, treatment initiation age, and male sex are reported as risk factors for treatment failure [4, 11]. Most case series are either small, did not follow a standard protocol, or were based on clinical rather than sonographic grading which is less specific and sensitive. In addition, not all the potential causes of treatment failure were studied.
The purpose of the study is to identify independent prognostic factors that could predict PH treatment failure in patients with DDH.
Methods
This is a retrospective study of infants, who were less than six months of age, that were treated with a Pavlik harness. The study was conducted and reported in accordance with Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies [32].
Demographic, sonographic, and clinical data were registered in a purpose-designed Microsoft Access Database. Referred patients were assessed according to the baby hip clinic initial assessment proforma. Based on the clinical and radiological findings, patients were either discharged, monitored, or treated with PH. A few patients who were close to six months of age were treated with surgery as first-line treatment. These patients were excluded from the study. Patients with Graf type I hips are considered normal and consequently were discharged. Patients with Graf IIa were monitored on a monthly basis. Graf IIb and onwards were treated with the PH.
Patients were provided with individual follow-up plans. Each follow-up involved completing the baby hip clinic follow-up assessment and ultrasound examination to monitor progress. The Pavlik harness treatment was considered successful and stopped when the hip became normal (Graf type I). Treatment failure was considered when there is worsening, or no improvement, and the PH was abandoned, and surgical treatment was offered. When a hip is subluxed or not centered (B angle is above 77°), a maximum of two weeks of Pavlik harness treatment is allowed for the hip to reduce. If not, the harness will be abandoned. This is to prevent the Pavlik harness syndrome which is the damage to the posterior rim of the acetabulum. The latter can pose a difficulty not only to future treatment but also to the Pavlik harness treatment itself. In contrast to a well-centered but dysplastic hip (A-angle is < 60°), treatment is continued until the hip is normalized.
The main objective of this research was to identify the success and failure rates and prognostic factors for failure and establish the strength of association with failure (or success). Our null hypothesis is that there are no prognostic factors that could predict the failure of PH treatment in DDH. Data was collected using the baby hip clinic database. Most data were collected retrospectively but some data were collected prospectively using the initial assessment form and follow-up assessment form of the baby hip clinic (see Appendices 1 and 2). Variables obtained from the data are quantitative and qualitative. Quantitative data includes continuous variables such as age and duration of treatment. Qualitative data includes nominal variables such gender, first born status, family history, foot deformity, plagiocephaly, breech presentation, Galeazzi sign, hip abduction, and femoral nerve palsy. Ordinal variables include hip ultrasound Graf classification and hip stability.
The latter was classified into five grades: stable, dislocatable, dislocated but reducible, dislocated but irreducible, and unable to assess. However, for the purpose of this study analysis, hip stability was recoded as not dislocatable and dislocatable to maximize the power of the statistical test while keeping a meaningful clinical message [33].
Hip abduction was coded as full or limited as used clinically. Graf hip types are classified as listed in Table 1. This variable was not condensed to a binary outcome because it is a radiological finding. However, if a child has bilateral hip dysplasia, we used the worse side as a predictor for treatment failure. In our experience, this is almost always correct.
Data were formally checked for normality using Kolmogorov-Smirnov test (KST) and visually. The methods used for descriptive statistics of continuous variables are measures of tendency and dispersion, while categorical variables are described by calculating proportion and frequency. The categorical dichotomous independent variables were cross tabulated with the outcomes tested using chi-square or Fisher exact test based on sample size. Categorical independent variables with more than two independent variables were compared visually through a bar chart in adherence to chi-square conditions. Continuous independent variables were all nonparametric and thus were analyzed using the Mann-Whitney test for significance. Independent variables that proved significance in the univariate analysis were then entered in the multivariate analysis to identify prognostic factors for failure. Multiple logistic regression was used to identify the interplay between the significant variables. The P value of ≤ 0.05 was chosen to determine statistical significance. Missing data were excluded from the analysis.
Results
Success rate of Pavlik harness
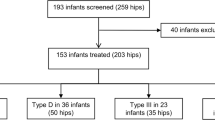
Two hundred and sixty-five patients out of 3885 patients, who were referred to the baby hip clinic, were treated with PH in the five year period of analysis. All patients completed their treatment and there was no loss to follow-up during the treatment phase; however, two patients lost to follow-up after treatment was finished and were excluded from the study. Two hundred and twenty-one patients (83.4%) were successfully treated, while 44 (16.6%) failed the treatment.
Prognostic factors for failure of Pavlik harness univariate analysis
Thirteen factors of interest were assessed to identify the ones that could predict failure of PH treatment (Table 3). Age, plagiocephaly, positive Galeazzi sign, hip instability, higher grades on Graf hip classification, and the development of femoral nerve palsy were shown to be significant on univariate analysis (P ≤ 0.05). The mean age of successful treatment was 6.73 weeks in comparison to 8.84 weeks for failure of treatment.
The influence of the grades of the Graf classification on failure rates is illustrated in Table 4. The radiological type of hip as per Graf classification was a significant factor in predicting failure PH treatment. The higher the grade, the more likely it was that PH treatment failed (FET = 0.027).
Multivariate analysis
The significant variables were entered into a multiple logistic regression analysis in order to identify the confounder adjusted odds ratios of the prognostic factors. Table 5 illustrates our findings. This yielded significantly independent predictors of failed PH treatment by 4.43 folds due to a positive Galeazzi, 5.27 folds due to hip instability, 1.3 folds due to a higher Graf grade, and 4.724 folds due to the development of femoral nerve palsy.
Discussion
Pavlik harness is a commonly used treatment device for developmental dysplasia of the hip in patients younger than six months of age [1, 34]. Crude failure rate has been reported to be 11.6% (3.3–40%) [14]; however, there exists a lack of comprehensive assessment of possible prognostic factors that could lead to failure of treatment. Of the patients in the study, 83.4% (n = 221/265) were successfully treated, while 16.6% (n = 44/265) failed which is within the published range of successful treatment.
Our study identified several predictors for PH treatment failure. However, a positive Galeazzi sign, hip instability (on clinical examination), Graf classification, and the development of femoral nerve palsy were identified as independent prognostic factors for failed PH treatment.
The age at initiation of treatment was significant in the univariate analysis; however, upon running multivariate analysis, the adjusted OR, CI, and P value were no longer significant. This could be because most of the older patients had more severe findings in hip instability, limited hip abduction, and Graf type hip. Therefore, the regression model associated age as a confounding factor. The association between the two variables reported that failure increased with infants above three to six months of age [11, 35], whereas in our study, the mean age of patient population who failed treatment was 6.7 weeks. This is consistent with some published studies that reported a higher failure rate in children above seven weeks [36, 37].
Gender was not significantly associated with PH failure upon univariate analysis. Males constituted 18.3% of our study (n = 48/262) with a failure of 4.2% (n = 11/48), while females comprised of 81.7% of the study population (n = 214/262) with a failure of 12.6% (n = 33/214). Many studies show no association between gender and failure [11, 38,39,40]. One study, however, indicates that males whom are Graf type IV and Ortolani positive (dislocated reducible) are more likely to fail [41]. Another study claims that males past seven weeks in the PH will require alternative therapy [42]. The significance in these studies could be attributed to the severity of displacement as well as the prolonged duration of treatment rather than gender. A multivariate analysis would have been a better statistical analysis to uncover the play of confounding factors.
First born status, family history, and breech presentation had been hypothesized to be a predictor of treatment failure; however, our study shows no association between these three factors and PH failure. This is consistent with another published study by Omeroglu and colleagues [11]. There are studies that reported the presence of a foot deformity is a prognostic factor for failure [11, 43]; however, no significant association was established in our study. This could be a genuine finding; however, the small sample size regarding failed patients with foot deformities may preclude strong recommendation. In our series, patients with foot deformities compromise only 4.6% of the population (n = 12/257) and 4.5% of the total failure (n = 2/44).
Intra uterine packaging disorders such as plagiocephaly have been described as risk factors for developing DDH but not to treatment failure. In the univariate analysis that we conducted, there was a significant association between plagiocephaly and treatment of failure; however, upon adjusting for confounding factors, the significance and CI subsided. There is no literature on plagiocephaly and its prognostic value on PH failure; thus, more studies with larger sample sizes are required.
Galeazzi sign is a clinical finding that signifies the presence of a truly dislocated hip. Univariate and multivariate analyses indicated a strong association between Galeazzi sign and PH treatment failure. To the best of our knowledge, there are no studies that evaluated the presence of Galeazzi sign as a prognostic factor for PH treatment failure.
Like Galeazzi sign, clinical hip instability and Graf types III and IV are signs of actual dislocated hips and not a mere dysplasia. Both were significantly associated as independent prognostic factors with failure of PH treatment. Several studies reveal that 60% of the clinically dislocated and irreducible hips fail PH treatment, while the failure rate of dislocated but reducible hips is 40% [15, 37, 38, 44, 45]. The greatest proportion of patients that failed PH treatment in our study was found to be patients with hips that were assessed as dislocated irreducible 71% (n = 5/7) which is quite similar to the results of another study in which all cases with dislocated irreducible hips failed the Pavlik harness treatment (n = 6/6) [38]. Graf hip classification has been widely accepted as a radiological prognostic factor for PH treatment failure in which Graf hip 2a has the highest success rate, while Graf type hips III and IV have the highest failure rate [8, 38, 41, 44]. This is consistent with our findings. However, one intriguing finding is that nine patients (9.4%) with Graf type IIa failed PH treatment. This is more than expected if we compare it to treatment failure in type IIb. Therefore, we studied these nine patients individually. The median age was eight weeks (1, 2, 5, 8, 8, 9, 10, 10, 11) with six of them above the median. Seven were females. Seven were born by caesarian section and two developed femoral nerve palsy. We cautioned against any conclusion from these nine patients as the number is small and these may be a chance finding. Moreover, we do not recommend treating type IIa hips because most would resolve naturally.
Femoral nerve palsy is a complication of PH treatment and an early sign that can predict treatment failure [25]. The relationship between femoral nerve palsy is complicated as most clinicians abandon treatment when it occurs. This area will be the focus of ongoing research which we aim to publish separately.
There are some limitations of this study. The protocol of treatment for DDH was changed over time as more evidence had become available that most type IIa hips normalize naturally. Initially, type IIa was treated with PH; however, this was changed. Treatment was advocated for type IIb and worse. The lack of long-term follow-up precludes quantifying some of the long-term PH treatment complication such as avascular necrosis of the femoral head and residual dysplasia. However, there are several strengths of the study. It is one of the largest published series with 265 patients that were extracted from a larger population of 3800 patients who were referred to our baby hip clinics. A thorough analysis of various variables have been conducted including ones that have not been or rarely assessed before such as plagiocephaly, Galeazzi sign, foot deformities, and femoral nerve palsy.
Conclusions
Pavlik harness treatment is a successful treatment method with an average success of 85%. Several independent predictors for failure of PH treatment have been identified. These include a positive Galeazzi sign, a frankly dislocated hip, Graf types III and IV, and the development of femoral nerve palsy.
Data availability
Anonymous data is available on request.
Code availability
SPSS output data is available on request.
References
Alshryda S, Wright J (2013) A harness for treatment of congenital hip dislocation in infants. In: Classic papers in orthopaedics. Springer Science + Business Media. pp 555–557
Alshryda S, Jones S, Banaszkiewicz PA (2014) Postgraduate paediatric orthopaedics: the candidate’s guide to the FRCS (Tr and Orth) examination. Cambridge University Press, Cambridge
Thaler M, Biedermann R, Lair J, Krismer M, Landauer F (2011) Cost-effectiveness of universal ultrasound screening compared with clinical examination alone in the diagnosis and treatment of neonatal hip dysplasia in Austria. J Bone Joint Surg British 93-B:1126–1130. https://doi.org/10.1302/0301-620x.93b8.25935
Shorter D, Hong T, Osborn DA (2013) Cochrane review: screening programmes for developmental dysplasia of the hip in newborn infants. Evid Based Child Health 8:11–54. https://doi.org/10.1002/ebch.1891
Paton RW (2005) Screening for hip abnormality in the neonate. Early Hum Dev 81:803-806. S0378-3782(05)00184-2 [pii] https://doi.org/10.1016/j.earlhumdev.2005.09.001
de Hundt M, Vlemmix F, Bais JM, Hutton EK, de Groot CJ, Mol BW, Kok M (2012) Risk factors for developmental dysplasia of the hip: a meta-analysis. Eur J Obstet Gynecol Reprod Biol 165:8-17. S0301-2115(12)00297-7 [pii] https://doi.org/10.1016/j.ejogrb.2012.06.030
Ortiz-Neira CL, Paolucci EO, Donnon T (2011) A meta-analysis of common risk factors associated with the diagnosis of developmental dysplasia of the hip in newborns. Eur J Radiol 81:e344-351. S0720-048X(11)00771-6 [pii] https://doi.org/10.1016/j.ejrad.2011.11.003
Ömeroglu H (2018) Treatment of developmental dysplasia of the hip with the Pavlik harness in children under six months of age: indications, results and failures. J Children’s Orthop 12:308–316. https://doi.org/10.1302/1863-2548.12.180055
Õmeroğlu H (2014) Use of ultrasonography in developmental dysplasia of the hip. J Children’s Orthop 8:105–113. https://doi.org/10.1007/s11832-014-0561-8
Gardner ROE, Kelley SK, Alshryda S, Wedge J (2016) Chapter 4: evidence-base for the management of developmental dysplasia of the hip. In: Alshryda H, Banaszkiewicz (ed) Paediatric orthopaedics: an evidence-based approach to clinical questions. Springer. pp 51–75.
Omeroglu H, Kose N, Akceylan A (2015) Success of Pavlik harness treatment decreases in patients >/= 4 months and in ultrasonographically dislocated hips in developmental dysplasia of the hip. Clin Orthop Relat Res. https://doi.org/10.1007/s11999-015-4388-5
Al-Essa RS, Aljahdali FH, Alkhilaiwi RM, Philip W, Jawadi AH, Khoshhal KI (2017) Diagnosis and treatment of developmental dysplasia of the hip: a current practice of paediatric orthopaedic surgeons. J Orthop Surg 25:230949901771719. https://doi.org/10.1177/2309499017717197
Swarup I, Penny CL, Dodwell ER (2018) Developmental dysplasia of the hip. Curr Opin Pediatr 30:84–92. https://doi.org/10.1097/mop.0000000000000574
Ashoor M, Abdulla N, Elgabaly EA, Aldlyami E, Alshryda S (2020) Evidence based treatment for developmental dysplasia of the hip in children under 6 months of age. Syst Rev Exploratory Anal Surg. https://doi.org/10.1016/j.surge.2020.02.006
Gulati V (2013) Developmental dysplasia of the hip in the newborn: a systematic review. World J Orthop 4:32. https://doi.org/10.5312/wjo.v4.i2.32
Pavlik A (1953) A harness for treatment of congenital hip dislocation in infants. Acta Chir Orthop Traumatol Cech 20:93–100
Pavlik A (1992) The functional method of treatment using a harness with stirrups as the primary method of conservative therapy for infants with congenital dislocation of the hip. 1957. Clin Orthop Relat Res (281):4–10
van der Sluijs JA, De Gier L, Verbeke JI, Witbreuk MM, Pruys JE, van Royen BJ (2009) Prolonged treatment with the Pavlik harness in infants with developmental dysplasia of the hip. J Bone Joint Surg Br 91:1090–1093. 91-B/8/1090 [pii] https://doi.org/10.1302/0301-620X.91B8.21692
Nakamura J, Kamegaya M, Saisu T, Someya M, Koizumi W, Moriya H (2007) Treatment for developmental dysplasia of the hip using the Pavlik harness: long-term results. J Bone Joint Surg Br 89:230-235. 89-B/2/230 [pii] https://doi.org/10.1302/0301-620X.89B2.18057
Grill F, Bensahel H, Canadell J, Dungl P, Matasovic T, Vizkelety T (1988) The Pavlik harness in the treatment of congenital dislocating hip: report on a multicenter study of the European Paediatric Orthopaedic Society. J Pediatr Orthop 8:1–8
Wilkinson AG, Sherlock DA, Murray GD (2002) The efficacy of the Pavlik harness, the Craig splint and the von Rosen splint in the management of neonatal dysplasia of the hip. A comparative study. J Bone Joint Surg Br 84:716–719
Cashman JP, Round J, Taylor G, Clarke NM (2002) The natural history of developmental dysplasia of the hip after early supervised treatment in the Pavlik harness. A prospective, longitudinal follow-up. J Bone Joint Surg Br 84:418–425
Wada I, Sakuma E, Otsuka T, Wakabayashi K, Ito K, Horiuchi O, Asagai Y, Kamegaya M, Goto E, Satsuma S, Kobayashi D, Saito S, Taketa M, Takikawa K, Nakashima Y, Hattori T, Mitani S, Wada A (2013) The Pavlik harness in the treatment of developmentally dislocated hips: results of Japanese multicenter studies in 1994 and 2008. J Orthop Sci 18:749–753. https://doi.org/10.1007/s00776-013-0432-z
Westacott DJ, Mackay ND, Waton A, Webb MS, Henman P, Cooke SJ (2013) Staged weaning versus immediate cessation of Pavlik harness treatment for developmental dysplasia of the hip. J Pediatr Orthop B 23:103–106. https://doi.org/10.1097/BPB.0000000000000025
Murnaghan ML, Browne RH, Sucato DJ, Birch J (2011) Femoral nerve palsy in Pavlik harness treatment for developmental dysplasia of the hip. The Journal of bone and joint surgery American volume 93:493-499. 93/5/493 [pii] https://doi.org/10.2106/JBJS.J.01210
Mafalda Santos M, Filipe G (1997) [Treatment of congenital hip dislocation using Pavlik’s harness. Long term results].Rev Chir Orthop Reparatrice Appar Mot 83:41-50. MDOI-RCO-02-1997-83-1-0035-1040-101019-ART75 [pii]
Filipe G, Carlioz H (1982) Use of the Pavlik harness in treating congenital dislocation of the hip. J Pediatr Orthop 2:357–362
Atar D, Lehman WB, Tenenbaum Y, Grant AD (1993) Pavlik harness versus Frejka splint in treatment of developmental dysplasia of the hip: bicenter study. J Pediatr Orthop 13:311–313
Czubak J, Piontek T, Niciejewski K, Magnowski P, Majek M, Plonczak M (2004) Retrospective analysis of the non-surgical treatment of developmental dysplasia of the hip using Pavlik harness and Frejka pillow: comparison of both methods. OrtopTraumatol Rehabil 6:9-13. 10796 [pii]
Johnson AH, Aadalen RJ, Eilers VE, Winter RB (1981) Treatment of congenital hip dislocation and dysplasia with the Pavlik harness. Clin Orthop Relat Res (155):25–9
Walton MJ, Isaacson Z, McMillan D, Hawkes R, Atherton WG (2010) The success of management with the Pavlik harness for developmental dysplasia of the hip using a United Kingdom screening programme and ultrasound-guided supervision. J Bone Joint Surg Br 92:1013–1016. https://doi.org/10.1302/0301-620X.92B7.23513
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, Initiative S (2014) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg 12:1495–1499. https://doi.org/10.1016/j.ijsu.2014.07.013
Starnes DS, Tabor J, Yates D, Moore DS (2014) The Practice of Statistics. W. H. Freeman
Alshryda S, Howard JJ, Huntley JS, Schoenecker JG (2019) The pediatric and adolescent hip: essentials and evidence. Springer International Publishing
Storer SK, Skaggs DL (2006) Developmental dysplasia of the hip. Am Fam Physician 74:1310–1316
Atalar H, Sayli U, Yavuz OY, Uraş I, Dogruel H (2007) Indicators of successful use of the Pavlik harness in infants with developmental dysplasia of the hip. Int Orthop 31:145–150. https://doi.org/10.1007/s00264-006-0097-8
Viere RG, Birch JG, Herring JA, Roach JW, Johnston CE (1990) Use of the Pavlik harness in congenital dislocation of the hip. An analysis of failures of treatment. J Bone Joint Surg Am 72:238–244
Lerman JA, Emans JB, Millis MB, Share J, Zurakowski D, Kasser JR (2001) Early failure of Pavlik harness treatment for developmental hip dysplasia: clinical and ultrasound predictors. J Pediatr Orthop 21:348–353
Jones GT, Schoenecker PL, Dias LS (1992) Developmental hip dysplasia potentiated by inappropriate use of the Pavlik harness. J Pediatr Orthop 12:722–726
Vadillo P, Encinas-Ullan CA, Moraleda L, Albinana J (2015) Results of the Pavlik harness when treating Ortolani-positive hips: predictors of failure and arthrographic findings. J Child Orthop 9:249–253. https://doi.org/10.1007/s11832-015-0666-8
Novais EN, Kestel LA, Carry PM, Meyers ML (2016) Higher Pavlik harness treatment failure is seen in Graf type IV ortolani-positive hips in males. Clin Orthop Relat Res 474:1847–1854. https://doi.org/10.1007/s11999-016-4776-5
Borges JL, Kumar SJ, Guille JT (1995) Congenital dislocation of the hip in boys. J Bone Joint Surg Am 77:975–984. https://doi.org/10.2106/00004623-199507000-00001
Lee WC, Gera SK, Mahadev A (2019) Developmental dysplasia of the hip: why are we still operating on them? A plea for institutional newborn clinical screening. Singapore Med J 60:150–153. https://doi.org/10.11622/smedj.2018064
Köse N, Omeroğlu H, Ozyurt B, Akçar N, Ozçelik A, Inan U, Seber S (2006) Our three-year experience with an ultrasonographic hip screening program conducted in infants at 3 to 4 weeks of age. Acta Orthop Traumatol Turc 40:285–290
White KK, Sucato DJ, Agrawal S, Browne R (2010) Ultrasonographic findings in hips with a positive Ortolani sign and their relationship to Pavlik harness failure. The Journal of bone and joint surgery American volume 92:113-120. 92/1/113 [pii] https://doi.org/10.2106/JBJS.H.01880
Acknowledgements
We would like to thank our librarians at the above centers for obtaining some of the references that are used in the manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation and data collection were performed by Nicholas Heinz, Vasileios Alexopoulos, Ibrar Majid, and Sattar Alshryda. Data cleaning and analysis were performed by Nada Abdulla, Maryam Ashoor, Sattar Alshryda, and Amar Hassan Khamis. The first draft of the manuscript was written by Nada Abdulla and Sattar Alshryda and refined by Ibrar Majid and Emmanouil Morakis, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Informed consent
Not applicable, as only no identifiable data have been used.
Consent for publication
All authors have agreed to publication.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Abdulla, N., Ashoor, M., Heinz, N. et al. Prognostic factors for failed Pavlik harness treatment in infants with developmental dysplasia of the hip: a retrospective cohort study. International Orthopaedics (SICOT) 47, 2337–2345 (2023). https://doi.org/10.1007/s00264-023-05829-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-023-05829-3