
Abstract
Purpose
This study aimed to evaluate the outcomes of dual plating for unstable distal femoral fractures via a subgroup analysis between periprosthetic and non-periprosthetic fractures.
Methods
This retrospective cohort study analyzed the outcomes of dual plating for unstable distal femoral fractures among 49 consecutive patients (43 women and 6 men) enrolled from July 2008 to August 2020. The patients were divided into periprosthetic (group P, n = 29) and non-periprosthetic (group N, n = 20) groups. The radiographic outcomes included the mechanical lateral distal femoral angle (mLDFA) and union rate based on the computed tomography findings. The clinical parameters included the knee range of motion and knee society score (KSS).
Results
The mean patient age was 71.1 years, and the average follow-up period was 37 months (range, 12–138 months). Union was achieved in 47 patients (96%). The average final mLDFA was 90.5° in group P and 88.3° in group N. The average final knee range of motion was 130° in group P and 107° in group N. The average final KSS was 73.8 in group P and 87.1 in group N.
Conclusion
Dual plating for distal femoral fractures yielded an excellent union rate and limb alignment with a low complication rate.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
With the growing aging population, the incidence rate of osteoporosis and the number of total knee arthroplasties (TKAs) continues to increase and consequently increase periprosthetic and non-periprosthetic distal femoral fractures (PDFFs and NDFFs, respectively) [1, 2]. However, the optimal surgical treatment for unstable distal femoral fractures is still challenging for several reasons, including poor bone quality, limited distal bone stock, medial cortical comminution, and blood supply alteration [3,4,5,6,7,8]. Conventional single lateral locked plating for distal femoral fractures has been reported to yield a nonunion rate of up to 15%, which does not seem to be satisfactory [9, 10]. Among PDFFs after TKA, Su type III fractures with distal fracture extension beyond the anterior flange or cases with severely comminuted medial cortices are likely to have poor outcomes with single lateral plating owing to limited (poor) bone stock, which leads to insufficient fixation power and loss of the medial buttress and consequently to varus collapse [4, 5, 11, 12]. Meanwhile, several studies have shown that single locked plate osteosynthesis for unstable NDFFs with extensive metaphyseal comminution yields high rates of mechanical complications, such as varus collapse, loss of fixation, and nonunion [3, 13,14,15,16].
Dual plating has been introduced to overcome the limitations of internal fixation for unstable distal femoral fractures [4, 17, 18]. Recently, it was reported that for comminuted distal femoral fractures or very low PDFFs, dual plating yielded an excellent union rate and a lower revision rate with better clinical outcomes than did conventional single lateral plating [17, 19, 20]. However, there is still a paucity of literature. We hypothesized that this technique would yield a satisfactory bone union rate and a good limb alignment for both PDFFs and NDFFs. The purpose of this study was to evaluate the surgical outcomes of dual plating for unstable distal femoral fractures via a subgroup comparison between PDFFs and NDFFs.
Methods
Study design and patient selection
This single-centre retrospective cohort study was approved by our institutional review board. All research was performed in accordance with relevant guidelines/regulations. All study participants provided informed consent. The inclusion criteria were distal femoral fractures treated with dual plating from July 2008 to August 2020, age of ≥ 20 years, and a follow-up period of ≥ 12 months. Meanwhile, the exclusion criteria were periprosthetic fracture during TKA, previously known infection or obvious fracture-related infection, polytrauma (injury severity score of > 18), pathologic fracture, and radiation-related fracture. To obtain large-scale empirical results of dual plating for unstable distal femoral fractures, we enrolled suitable patients from our institutional database as much as possible (Fig. 1).

Flowchart of patient enrollment. ISS, injury severity score
Indications of dual plating were as follows: (1) limited (poor) distal bone stock, including implant-stable periprosthetic fracture and far distal fracture, (2) metaphyseal comminution, and (3) poor bone quality among elderly patients. A total of 49 patients (43 women and 6 men) were enrolled and consequently divided into two groups: PDFF (group P, n = 29) and NDFF (group N, n = 20) groups.
Surgical techniques and post-operative rehabilitation
For dual plating with separate incisions, the order of fixation was dependent on the fracture pattern and easiness of reduction. Fixation was achieved through limited open reduction and/or minimally invasive percutaneous osteosynthesis (MIPO) to preserve the local blood supply for the soft tissue and bone. Lateral MIPO using a distal femoral locking compression plate (LCP-DF, Depuy Synthes®, West Chester, PA, USA) and medial MIPO through the subvastus approach using a proximal humeral internal locking system plate (Philos, Depuy Synthes®, West Chester, PA, USA) were the most frequently used combinations; however, other plates were also used.
All patients followed the same standardized post-operative rehabilitation program and were encouraged to perform early assisted ambulation. Gentle passive knee range of motion (ROM) exercise using a continuous passive motion machine was initiated after drain removal. The patients were followed up at six week intervals for the first three month and two month intervals thereafter until bone union was identified. At each visit, we routinely obtained plain knee radiographs of the affected site using four orthogonal views: anteroposterior, lateral, and both oblique views. Three-dimensional computed tomography (CT) was performed at post-operative three months and additionally reperformed when bone union seemed to be expected on the radiographs.
Demographic and fracture characteristics
The baseline demographic characteristics, such as age, sex, body mass index, presence of diabetes, and mechanism of injury, as well as the fracture characteristics, such as open wound, Su [5] classification for PDFFs, AO/OTA classification [21] for NDFFs, and comminution, were recorded. We defined fracture comminution as loss of buttress on either side of the cortices after reduction.
Radiographic evaluation and parameters
Bone union was defined as bridging of callus formation across the fracture site on the sagittal and coronal reconstructed CT images at two or more cortices. CT scans have advantages in the detection of callus bridging. Generally, it is not easy to evaluate bone bridging fixed with dual plates using two orthogonal radiographs because two plates and several screws hide the cortical surface and interfere with the evaluation of bone bridging. We also used a radiographic union score for hip (RUSH) [22] score of ≥ 15 supplementarily. Nonunion was defined as a condition with no sign of bone healing until nine months after surgery.
The mechanical lateral distal femoral angle (mLDFA) at pre-injury (when possible), at the immediate post-operative and three month post-operative periods, and at the last follow-up radiography was measured to analyze the changes in the femoral mechanical axis. We defined the varus collapse angle as the amount of increase in the mLDFA from the immediate post-operative period to the follow-up period. Mechanical failure resulting from varus collapse was defined as a more than five degree change in alignment at the coronal plane on the immediate post-operative radiograph. The number of screws fixed in the distal bone stock, working length, and plate length was recorded.
Clinical parameters
The clinical parameters included the knee ROM, walking ability evaluated using the Koval score [23], and knee society score (KSS) [24] at post-operative one year. The need for reoperation and complications, such as infection, mechanical failure, and nonunion, was also evaluated.
Statistical analysis
Between-group comparisons of the demographic and fracture characteristics (continuous variables) were performed using the t-test, Wilcoxon rank-sum test, or Kruskal–Wallis test. Categorical variables were analyzed using Fisher’s exact test.
Within-group comparisons of the radiographic outcomes, mLDFA, before surgery, and at each follow-up point were performed using a paired t-test. Between-group comparisons of the surgical outcomes (union time, varus collapse angle, final mLDFA, and KSS) were performed using a paired t-test and the Kruskal–Wallis test. P-values of < 0.05 were considered statistically significant.
Results
Patient and fracture characteristics
The mean patient age was 71.1 years, and 86% of the patients (93% in group P and 75% in group N) were aged ≥ 60 years. The average follow-up period was 36.9 months (range, 12–138 months). There were no significant between-group differences in the demographic and fracture characteristics, except for sex, the injury severity score, and the rate of high-energy injury (Table 1).
In group P, according to the Su classification, there were two patients with type I fractures, four with type II fractures, and 23 with type III fractures. There were two cases needing a revision stem, which were classified as Su type I fractures (Fig. 2). Comminution was observed in 48% of the patients in group P: 0% with Su type I fractures, 50% with Su type II fractures, and 52% with Su type III fractures. On average, 9.3 distal screws were inserted. The mean plate length was 6.0 holes in the medial side and 7.2 holes in the lateral side. The mean working length was 2.1 holes in the medial and 2.5 holes in the lateral side.

An 86-year-old woman treated with double plating for Su type I periprosthetic fracture. a Pre-operative AP and lateral radiographs. b Pre-operative computed tomography scan (coronal cut). c Immediate postoperative AP radiograph. Long dual plates were used owing to a lack of bone stock in the distal segment. d Three-year post-operative AP radiograph. AP, anteroposterior
Among the 20 patients in group N, 75% were aged ≥ 60 years, and 35% had high-energy injuries. Only two patients presented AO/OTA 33A3 fractures, and the other 18 patients had 33C fractures. The subtypes of the 33C fractures and number of patients with each subtype were as follows: C1 (n = 3), C2 (n = 14), and C3 (n = 1). Comminution was observed in 85% of the patients in group N. Three C1 fractures did not show comminution. All three patients with C1 fractures were aged > 70 years and had osteoporotic far distal fractures. Two of them had severe osteoporosis based on the bone mineral density, while one had a proximal femoral stem from a previous hip surgery.
There were three cases of open fracture in group N: one case of Gustilo type 1 fracture and two cases of Gustilo type 2 fracture. We performed a staged surgical procedure for the two cases of Gustilo type 2 fractures for soft tissue and infection control. One patient achieved bone union after secondary bone grafting, while the other patient needed revision osteosynthesis owing to mechanical failure (Fig. 3).

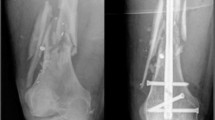
A 69-year-old man with Gustilo type 2 AO/OTA 33 C2.2 fracture. a Initial AP and lateral radiographs. A lateral open wound was noted at the level of severe metaphyseal comminution (left knee). b. Immediate post-operative AP and lateral radiographs. Debridement and dual locking plate fixation were performed. At 4 weeks after the initial surgery without any sign of infection, auto bone grafting was performed to fill the bony defect. c Three-month post-operative AP and lateral radiographs. Metal failure occurred after a minor slip down. d AP and lateral radiographs after revisional fixation. Revisional fixation was performed using longer lateral plates. e Whole lower bone standing AP radiograph at 14 months after revisional surgery. AP, anteroposterior
Surgical outcomes
Bone union was achieved in 47 patients (96%). And the mean union time was 36.2 ± 22.1 weeks. The mean final RUSH score was 19.9 ± 3.7 in group P and 19.1 ± 2.9 in group N. There was no significant difference in the union rate and union time between the groups (Table 2). The mean mLDFA after surgery was restored to 90.5° and 87.7° and maintained at 90.5° and 88.3° until final follow-up in groups P and N, respectively. The average final varus collapse angle was − 0.1° in group P and 0.6° in group N. The changes in the mLDFA and varus collapse angle by time in each group are plotted in Fig. 4, and all cases, except for two cases of mechanical failure, had a well-maintained mLDFA. There were no differences in the overall change in the mLDFA and varus collapse angle by time between the groups (mLDFA: p = 0.533, varus collapse angle: p = 0.640).

Mean and standard error plots of the mLDFA and varus collapse angle in each group according to the follow-up period. a mLDFA (°). b Varus collapse angle (°). mLDFA, mechanical lateral distal femoral angle
The average final knee ROM was 130° in group P and 107° in group N. The average final Koval score was 1.7 in group P and 1.8 in group N. The average final KSS was 73.8 in group P and 87.1 in group N. There were two cases of mechanical failure: one in each group (Figs. 3 and 5). There were six cases (12%) needing secondary surgery. No case of infection was observed. We found no difference in the documented complications between the groups.

A 73-year-old woman with mechanical failure in group P. a Initial AP and lateral radiographs. The lateral cortex was severely comminuted. b Immediate post-operative AP and lateral radiographs. A long lateral locking plate and posteromedial one-third tubular plate were fixed. c Eighteen-month post-operative AP radiograph. Varus collapse and mechanical failure were noted. d Two-year post-operative AP radiograph. A golf club deformity with nonunion was noted. AP, anteroposterior
Discussion
Several radiological, cadaveric, biomechanical, and clinical studies advocated promising results with the safe and successful placement of additional medial plates for distal femoral fractures [17, 25,26,27,28,29]. In our study, dual plate osteosynthesis for unstable distal femoral fractures yielded satisfactory radiographic outcomes with a low complication rate: 96% of the cases achieved bone union with good mechanical alignment. In the subgroup comparison, both groups showed similar surgical outcomes. Park et al. reported excellent outcomes after dual plating for 21 cases of Su type III PDFFs [19]. Similar to our results in the periprosthetic group, 20 out of 21 of their cases achieved union, and the mean mLDFA was 89°. A few previous studies have focused on promising surgical outcomes of dual plating osteosynthesis for Su type III PDFFs or comminuted distal femoral fractures [18, 19]. In our study, we reviewed dual plate osteosynthesis for both periprosthetic and non-periprosthetic distal femoral fractures in a large sample size.
In both groups, a good mechanical alignment was maintained until the final follow-up. To achieve a neutral mechanical alignment, we set the ideal target for the mLDFA to 90° for periprosthetic fractures and 87–88° for non-periprosthetic fractures. An appropriate reduction was achieved post-operatively, as noted by the mean mLDFA of 90.5° in group P and 87.7° in group N. This reduction was well maintained at a mean mLDFA of 90.5° in group P and 88.3° in group N until the final follow-up. The mean varus collapse angle converged to 0° in both groups. Similar to the findings of Park et al. that a good mechanical alignment of Su type III periprosthetic fractures was achieved after dual plating [19], we also achieved excellent maintenance of limb alignment until the final follow-up without varus collapse in a majority of the patients.
Herein, the clinical parameters in both groups were satisfactory and comparable to each other. The knee ROM was better in group P (130°) than in group N (107°) (p = 0.14). However, group N (87.1) had a better KSS than group P (73.8). The average walking ability assessed using the Koval score was similar at the final follow-up (group P: 1.7, group N: 1.8). Although the patients in group N had more severe injuries from high-energy trauma, the underlying knee disability and relatively older age of the patients in group P would affect the results.
The mean union time was 34 weeks in group P, and 40 weeks in group N. These results are quite longer than those of previous studies (≤ 20 weeks) [17, 19]. There can be several possible reasons. First, stricter criteria of bone union on CT were applied in our study. Second, the dual plate construct was too rigid to permit micromotions between fracture fragments. Because locking plate osteosynthesis is based on indirect bone healing, the least micromotion of a too rigid construct with a short working length could delay the union process [30,31,32]. In our study, the rigid dual plate construct with a short working length might have contributed to the small number of mechanical failures and longer union time. Third, medial plates could affect vascular insufficiency and consequently delayed healing. A recent cadaveric injection study showed that the medial periosteal arteries might be compressed by medial plating of the distal femur [29]. Periosteal vascular insults could potentially affect bone healing after dual plating.
Mechanical failure after surgery was observed only in two patients (4%). A 73-year-old woman in group P showed gradual varus collapse and mechanical failure (Fig. 5); a short medial plate would not be enough to maintain the medial buttress. A 69-year-old man in group N had Gustilo type 2 open fracture with severe comminution (Fig. 3). Although mechanical failure occurred after a slip down, the short lateral plate would not support stable fixation considering the relatively long zone of comminution. Comminuted fractures are typically treated with longer bridging constructs, where the plate length is at least twice the zone of comminution, and four well-spaced bicortical screws are placed in the shaft [33].
Thus, dual plating helped provide strong stability and maintain alignment for distal femoral fractures with a poor distal bone stock or metaphyseal comminution and yielded a very low mechanical failure rate in our study. (1) Twenty-three cases of Su type III fractures and two cases of Su type I fractures with a femoral stem had limited (poor) distal bone stock. In these cases, it was difficult to insert a sufficient number of distal screws with a single plate; however, the dual plate allowed a stable fixation. Generally, very low NDFFs in elderly porotic bones could achieve enough stability after dual plating despite the poor bone stock. (2) Distal femoral fractures with metaphyseal comminution could avoid varus collapse after dual plating even if the risk is high owing to loss of the medial buttress effect [12, 20].
This study has several limitations. The study retrospectively analyzed heterogeneous groups with small sample size and did not involve a long-term follow-up. To enroll a large sample size as much as possible, we set the duration of patient enrollment to approximately 12 years, which could indicate the inclusion of heterogeneous participants. However, we believe that our study provides one of the largest empirical data to surgeons who have difficulties in selecting dual plate osteosynthesis for distal femoral fractures. To the best of our knowledge, this study is the largest comparative study of the radiographic outcomes of dual plating between PDFFs and NDFFs. As distal femoral fractures are not common but have an increasing incidence and are challenging to manage in the geriatric population, much larger prospective studies are required to analyze the indications and outcomes of dual plating.
In conclusion, dual plating osteosynthesis yielded satisfactory clinical outcomes and a well-maintained alignment of the distal femur in the patients with PDFFs and NDFFs. Therefore, we believe that dual plating is a promising surgical option for unstable distal femoral fractures with poor bone stock or metaphyseal comminution.
Data availability
The data presented in this study are available upon request from the corresponding author. The data are not publicly available because of the conditions of the ethics committee of our university.
References
Elsoe R, Ceccotti AA, Larsen P (2018) Population-based epidemiology and incidence of distal femur fractures. Int Orthop 42:191–196. https://doi.org/10.1007/s00264-017-3665-1
Parvizi J, Jain N, Schmidt AH (2008) Periprosthetic knee fractures. J Orthop Trauma 22:663–671. https://doi.org/10.1097/BOT.0b013e31816ed989
Ebraheim NA, Liu J, Hashmi SZ, Sochacki KR, Moral MZ, Hirschfeld AG (2012) High complication rate in locking plate fixation of lower periprosthetic distal femur fractures in patients with total knee arthroplasties. J Arthroplasty 27:809–813. https://doi.org/10.1016/j.arth.2011.08.007
Kim W, Song JH, Kim JJ (2015) Periprosthetic fractures of the distal femur following total knee arthroplasty: even very distal fractures can be successfully treated using internal fixation. Int Orthop 39:1951–1957. https://doi.org/10.1007/s00264-015-2970-9
Su ET, DeWal H, Di Cesare PE (2004) Periprosthetic femoral fractures above total knee replacements. J Am Acad Orthop Surg 12:12–20
Streubel PN, Gardner MJ, Morshed S, Collinge CA, Gallagher B, Ricci WM (2010) Are extreme distal periprosthetic supracondylar fractures of the femur too distal to fix using a lateral locked plate? J Bone Joint Surg Br 92:527–534. https://doi.org/10.1302/0301-620X.92B3.22996
Kregor PJ, Hughes JL, Cole PA (2001) Fixation of distal femoral fractures above total knee arthroplasty utilizing the less invasive stabilization system (L.I.S.S.). Injury 32(Suppl 3):SC64-75. https://doi.org/10.1016/s0020-1383(01)00185-1
Anakwe RE, Aitken SA, Khan LA (2008) Osteoporotic periprosthetic fractures of the femur in elderly patients: outcome after fixation with the LISS plate. Injury 39:1191–1197. https://doi.org/10.1016/j.injury.2008.02.003
Ristevski B, Nauth A, Williams DS et al (2014) Systematic review of the treatment of periprosthetic distal femur fractures. J Orthop Trauma 28:307–312. https://doi.org/10.1097/BOT.0000000000000002
Ebraheim NA, Kelley LH, Liu X, Thomas IS, Steiner RB, Liu J (2015) Periprosthetic distal femur fracture after total knee arthroplasty: a systematic review. Orthop Surg 7:297–305. https://doi.org/10.1111/os.12199
Matlovich NF, Lanting BA, Vasarhelyi EM, Naudie DD, McCalden RW, Howard JL (2017) Outcomes of surgical management of supracondylar periprosthetic femur fractures. J Arthroplasty 32:189–192. https://doi.org/10.1016/j.arth.2016.06.056
Sim JA, Shon OJ, Joo YB, Sohn HS, Byun SE, Kim JW (2021) Clinical outcomes of osteosynthesis of well-fixed periprosthetic proximal tibial fractures (Felix type 2A) after total knee arthroplasty. Injury. https://doi.org/10.1016/j.injury.2021.06.022
Henderson CE, Lujan TJ, Kuhl LL, Bottlang M, Fitzpatrick DC, Marsh JL (2011) 2010 mid-America Orthopaedic Association Physician in Training Award: healing complications are common after locked plating for distal femur fractures. Clin Orthop Relat Res 469:1757–1765. https://doi.org/10.1007/s11999-011-1870-6
Ebraheim NA, Martin A, Sochacki KR, Liu J (2013) Nonunion of distal femoral fractures: a systematic review. Orthop Surg 5:46–50. https://doi.org/10.1111/os.12017
Hoffmann MF, Jones CB, Sietsema DL, Tornetta P 3rd, Koenig SJ (2013) Clinical outcomes of locked plating of distal femoral fractures in a retrospective cohort. J Orthop Surg Res 8:43. https://doi.org/10.1186/1749-799X-8-43
Davison BL (2003) Varus collapse of comminuted distal femur fractures after open reduction and internal fixation with a lateral condylar buttress plate. Am J Orthop (Belle Mead NJ) 32:27–30
Bologna MG, Claudio MG, Shields KJ, Katz C, Salopek T, Westrick ER (2020) Dual plate fixation results in improved union rates in comminuted distal femur fractures compared to single plate fixation. J Orthop 18:76–79. https://doi.org/10.1016/j.jor.2019.09.022
Medda S, Kessler RB, Halvorson JJ, Pilson HT, Babcock S, Carroll EA (2020) Technical trick: dual plate fixation of periprosthetic distal femur fractures. J Orthop Trauma. https://doi.org/10.1097/BOT.0000000000001869
Park KH, Oh CW, Park KC et al (2020) Excellent outcomes after double-locked plating in very low periprosthetic distal femoral fractures. Arch Orthop Trauma Surg. https://doi.org/10.1007/s00402-020-03655-5
Liu JF, Zhou ZF, Hou XD, Chen YX, Zheng LP (2021) Hybrid locked medial plating in dual plate fixation optimizes the healing of comminuted distal femur fractures: A retrospective cohort study. Injury 52:1614–1620. https://doi.org/10.1016/j.injury.2021.01.003
Meinberg EG, Agel J, Roberts CS, Karam MD, Kellam JF (2018) Fracture and Dislocation Classification Compendium-2018. J Orthop Trauma 32(Suppl 1):S1–S170. https://doi.org/10.1097/BOT.0000000000001063
Chiavaras MM, Bains S, Choudur H et al (2013) The Radiographic Union Score for Hip (RUSH): the use of a checklist to evaluate hip fracture healing improves agreement between radiologists and orthopedic surgeons. Skeletal Radiol 42:1079–1088. https://doi.org/10.1007/s00256-013-1605-8
Koval KJ, Aharonoff GB, Rosenberg AD, Bernstein RL, Zuckerman JD (1998) Functional outcome after hip fracture. Effect of general versus regional anesthesia. Clin Orthop Relat Res:37–41
Insall JN, Dorr LD, Scott RD, Scott WN (1989) Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res:13–14
Steinberg EL, Elis J, Steinberg Y, Salai M, Ben-Tov T (2017) A double-plating approach to distal femur fracture: a clinical study. Injury 48:2260–2265. https://doi.org/10.1016/j.injury.2017.07.025
Kim JJ, Oh HK, Bae JY, Kim JW (2014) Radiological assessment of the safe zone for medial minimally invasive plate osteosynthesis in the distal femur with computed tomography angiography. Injury 45:1964–1969. https://doi.org/10.1016/j.injury.2014.09.023
Jiamton C, Apivatthakakul T (2015) The safety and feasibility of minimally invasive plate osteosynthesis (MIPO) on the medial side of the femur: a cadaveric injection study. Injury 46:2170–2176. https://doi.org/10.1016/j.injury.2015.08.032
Muizelaar A, Winemaker MJ, Quenneville CE, Wohl GR (2015) Preliminary testing of a novel bilateral plating technique for treating periprosthetic fractures of the distal femur. Clin Biomech (Bristol, Avon) 30:921–926. https://doi.org/10.1016/j.clinbiomech.2015.07.008
Rollick NC, Gadinsky NE, Klinger CE et al (2020) The effects of dual plating on the vascularity of the distal femur. Bone Joint J 102-B:530–538. https://doi.org/10.1302/0301-620X.102B4.BJJ-2019-1776
Mardian S, Schaser KD, Duda GN, Heyland M (2015) Working length of locking plates determines interfragmentary movement in distal femur fractures under physiological loading. Clin Biomech (Bristol, Avon) 30:391–396. https://doi.org/10.1016/j.clinbiomech.2015.02.006
Hake ME, Davis ME, Perdue AM, Goulet JA (2019) Modern implant options for the treatment of distal femur fractures. J Am Acad Orthop Surg 27:e867–e875. https://doi.org/10.5435/JAAOS-D-17-00706
Harvin WH, Oladeji LO, Della Rocca GJ et al (2017) Working length and proximal screw constructs in plate osteosynthesis of distal femur fractures. Injury 48:2597–2601. https://doi.org/10.1016/j.injury.2017.08.064
Lee C, Brodke D, Gurbani A (2021) Surgical tips and tricks for distal femur plating. J Am Acad Orthop Surg. https://doi.org/10.5435/JAAOS-D-20-01221
Funding
This research was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (2021R1A2C1012972).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. J-HS wrote the entire manuscript as a first author. B-SL and J-MK contributed to material preparation, data collection and analysis as co-authors. J-JK contributed to surgical protocol description as a co-author. J-WK contributed to entire study process and quality control as a corresponding author. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval
This study was performed in line with the principles of the Declaration of Helsinki. This single-center retrospective cohort study was approved by our institutional review board (Asan Institute for Life Science, approval no.: 2020–1282).
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
The authors affirm that human research participants provided informed consent for publication of the radiograph images in Figs. 2, 3, and 5.
Competing interests
The authors declare no competing of interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Seo, J.H., Lee, BS., Kim, JM. et al. Outcomes of dual plating for unstable distal femoral fractures: a subgroup comparison between periprosthetic and non-periprosthetic fractures. International Orthopaedics (SICOT) 46, 2685–2692 (2022). https://doi.org/10.1007/s00264-022-05543-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-022-05543-6