
Abstract
Purpose
The objective of this article is to report associated anomaly incidences of a large CS cohort and analyze interrelationships among vertebral anomaly types and associated abnormalities.
Methods
We retrospectively searched and extracted medical records of 1289 CS inpatients surgically treated in our institute from January 2010 to December 2019. All patients have taken spine X-ray, CT, MRI, echocardiogram, urogenital ultrasound, and systemic physical examination. We analyzed information on demographics, CS types, and associated anomalies.
Results
CS type was found to be 49.1% for failure of formation (FF), 19.5% for failure of segmentation (FS), and 31.4% for mixed defects (MD). Intraspinal defects were found in 29.4% patients (16.0% for FF, 45.4% for FS, 40.5% for MD), cardiac in 13.7% (12.3% for FF, 14.3% for FS, 15.6% for MD), genitourinary in 5.8% (4.1% for FF, 6.0% for FS, 8.4% for MD), gastrointestinal in 3.6% (4.7% for FF, 1.6% for FS, 3.0% for MD), and musculoskeletal in 16.4% (10.3% for FF, 19.9% for FS, 23.7% for MD). The intraspinal and musculoskeletal defect incidences were significantly higher in patients with failure of segmentation and mixed defects. We also observed a decreasing trend for intraspinal and musculoskeletal defect incidences as well as a tendency for more failure of formation and less failure of segmentation from 2010 to 2019.
Conclusions
The intraspinal and musculoskeletal defect incidences were higher in patients with failure of segmentation and mixed defects. Strong interrelationships were found between intraspinal and musculoskeletal defects and among cardiovascular, genitourinary, and gastrointestinal defects. From 2010 to 2019, the proportion of patients with failure of formation increased significantly, causing a decrease in the intraspinal and musculoskeletal defect incidences over time. Female sex, failure of segmentation, and mixed defects could be considered risk factors for more associated anomalies in CS individuals, which would help surgeons in medical management and prenatal consultation.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Congenital scoliosis (CS) is the lateral curvature of the spine resulting from vertebral deformities that develop during four to six weeks of gestation and are present at birth. CS was reported to occur at a ratio of approximately 1 in every 1000 live births [1]. Congenital scoliosis is caused by abnormal vertebral development, and a multifactorial aetiology of CS is universally accepted [2,3,4]. While certain genetic and environmental factors have been implicated in congenital scoliosis [5,6,7,8,9], the aetiology of most CS remains unclear.
It is widely observed in clinical practice that CS patients usually have comorbidities of other congenital abnormalities. Among all kinds of congenital defects, intraspinal, cardiovascular, and genitourinary defects are the most common. Several previous studies have reported the incidences of different congenital defects in CS patients [7, 10,11,12,13,14,15,16,17,18,19]. However, the incidences varied greatly in different studies, and the interrelationship among these anomalies and the trend in recent years has not been fully clarified.
We retrospectively analyzed information from 1289 CS patients who were admitted for congenital scoliosis from January 2010 to December 2019 in our institute. The objective of this article is to report anomaly incidences of a large CS cohort and analyze interrelationships among vertebral anomaly types and associated abnormalities.
Material and methods
We retrospectively searched for cases who were admitted for congenital scoliosis from January 2010 to December 2019 in our institute from the inpatient database using ICD-10 codes (Q67.501, Q67.502). In total, 1289 inpatients are included in our study.
The CS types (namely failure of formation, failure of segmentation, and mixed defects) were diagnosed from the patients’ X-ray and spine CT [20, 21]. Echocardiogram, urogenital ultrasound, spine imaging, including MRI, X-ray and CT, and systemic physical examination were undertaken in all patients to screen and diagnose associated anomalies.
After automated extraction of patient information from the inpatient database, all patients’ medical records, including imaging reports, were reviewed and re-evaluated case by case to minimize missing data.
Statistical analysis
Descriptive statistics are expressed as the mean ± standard deviation for continuous variables and percentage (%) for categorical variables. The chi-square test was used to evaluate the relationships between categorical variables. P value < 0.05 was considered to indicate a statistically significant result. Statistical analysis was performed using IBM SPSS Statistics 23. Statistical graphs were plotted using Graphpad Prism 7.
Results
In total, 1289 CS patients were included in our study. The mean patient age was 12.4 ± 8.1 years old, and 54.0% were female (Table 1). Annual trends in age and sex structures were similar from 2010 to 2019.
Typical X-rays and spine CT 3D-reconstructions of three CS types were shown in Fig. 1.

Typical X-ray and CT 3D-reconstruction of three CS types, a X-ray and CT 3D-reconstruction of a patient with failure of formation (a hemivertebrae between T11 and T12) b X-ray and CT 3D-reconstruction of a patient with failure of segmentation (T9 to T11 segmentation defect), c X-ray and CT 3D-reconstruction of a patient with mixed defects (T9 hemivertebrae, T6 to T8 segmentation defect and fused ribs)
Among all 1289 CS patients, failure of formation was seen in 633 patients (49.1%), failure of segmentation in 251 patients (19.5%), and mixed defects in 405 patients (31.4%). The distribution of different vertebral anomaly types in male and female patients is presented in Table 1. There are significantly more cases with failure of formation and less failure of segmentation and mixed defects in male patients. Among the patients with congenital scoliosis, 39 patients had a constellation of abnormalities as part of a syndrome (Table 2). Within those syndromes, Klippel-Feil syndrome (n = 23) and VACTERL association (n = 11) were the most common.
The incidences of associated defects in different systems and those incidences reported by previous studies are summarized in Table 3. Intraspinal defects were found in 379 (29.4%) out of 1289 CS patients, cardiovascular defects in 177 patients (13.7%), genitourinary defects in 75 patients (5.8%), gastrointestinal defects in 46 patients (3.6%), and musculoskeletal defects in 211 patients (16.4%). We also found five patients with auricular defects (2 with congenital deafness and 3 with microtia) and nine patients with cleft lip and palate (Table 4).
The numbers of specific associated anomalies in this CS series are summarized in Table 4. Among 379 patients with intraspinal defects, diastematomyelia, syringomyelia, and tethered cord were the first three most frequent defects in our series, with incidences of 19.3% (n = 249), 13.2% (n = 170), and 9.1% (n = 117), respectively. There were 125 male patients (21.1%) and 254 female (36.5%) patients with intraspinal defects (Fig. 2a). The incidence of intraspinal defects was significantly lower in men than in women (p < 0.001). Intraspinal anomalies were found in 101 patients (16.0%) with failure of formation, 114 patients (45.4%) with failure of segmentation, and 164 patients (40.5%) with mixed defects (Fig. 2b). The patients with failure of segmentation and mixed defects were found to have significantly higher incidence of intraspinal defects.

Interrelationship of different associated anomalies, sexes and vertebral anomaly types, a Interrelationship between different associated anomalies and sexes. *p < 0.05, **p < 0.01, ***p < 0.001, b Interrelationship between different associated anomalies and vertebral anomaly types. *p < 0.05, **p < 0.01, ***p < 0.001
In this study, 177 patients (13.7%) were found to have cardiovascular abnormalities (Table 4). Valvular malformation was the most frequent defect with an incidence of 6.3%. The cardiovascular abnormalities had almost the same incidence between sexes (Fig. 2a). Patients with failure of segmentation and mixed defects had a slightly higher frequency of cardiovascular abnormalities, but the difference was not significant (p = 0.495) (Fig. 2b).
Genitourinary anomalies were found in 75 patients (5.8%) where a single kidney and an ectopic kidney were the most frequent comorbidities (Table 4). There was no significant difference between sexes (Fig. 2a), but patients with failure of segmentation and mixed defects did have a significantly higher incidence of genitourinary defects (p < 0.05) (Fig. 2b). The incidence of gastrointestinal anomalies was 3.6% in our study. Accessory spleen and anal atresia were the most frequent. There was no significant difference between sexes or vertebral anomaly types.
Musculoskeletal defects were found in 211 patients (16.4%), most of which were rib defects (Table 4). Non-significantly higher incidence (p = 0.076) and significantly higher incidence (p < 0.001) were observed in female patients and patients with failure of segmentation and mixed defects respectively (Fig. 2a, 2).
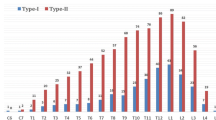
As for the level of congenital spinal defects, there were 5.7% (n = 74) of patients had cervical spine involved, 78.1% (n = 1008) had thoracic spine involved and 33.6% (n = 434) had lumbar spine involved. Intraspinal and musculoskeletal defects had higher incidences in patients with cervical and thoracic spine involved than in patients with lumbar spine involved (33.8% vs. 33.4% vs. 20.7% for intraspinal defects; 28.4% vs. 19.1% vs. 9.0% for musculoskeletal defects). No difference with statistical significance was observed in the incidences of cardiac, urogenital, and gastrointestinal defects among three groups (Table 5).
The interrelationship between different organ defects is shown in Fig. 3. Intraspinal defects were found in 44.9% of patients with musculoskeletal defects, an incidence significantly higher than that in the total CS population. Cardiac, genitourinary, and gastrointestinal defects were found to have a strong interrelationship with each other, although the association between cardiac and genitourinary defects was not significant. A significant correlation between genitourinary and musculoskeletal defects was also observed.

Interrelationship of different associated anomalies. The depth of color refers to the odds ratio between two associated defects, *p < 0.05, **p < 0.01, ***p < 0.001
After analyzing incidence changes in different associated anomalies during the last ten years (Fig. 4a), we found that intraspinal and musculoskeletal defects had an obvious decreasing trend from 2010 to 2019. Similarly, the proportion of failure of formation in our center had an obvious increasing tendency, while the proportion of failure of segmentation obviously decreased during the last ten years (Fig. 4b).

Trends in incidences of different associated anomalies and vertebral anomaly types from 2010 to 2019, a Trends in incidences of different associated anomalies, b Trends in vertebral anomaly types from 2010 to 2019, c Association between trends in incidences of different associated anomalies and trends in vertebral anomaly types from 2010 to 2019
Discussion
Several independent studies covering different ethnic populations have been published in recent years. However, most of these studies did not cover and analyze all common associated anomalies of CS and their interrelationship but focused only on one or two certain systems. Therefore, we conducted this study to fully depict the distribution, incidences and interrelationship of vertebral anomaly types and associated anomalies. To the best of our knowledge, this is the largest CS series of the Chinese population so far. In our study, a total of 1289 CS patients were included and all their medical records, including imaging examination reports, were reviewed and re-evaluated.
In all CS patients, 49.1% were typed as failure of formation, 19.5% as failure of segmentation, and 31.4% as mixed defects. This distribution was similar to that in previous studies [7, 14, 16, 18, 19]. We also found that failure of formation was significantly more common in male patients, whereas failure of segmentation or mixed defects were significantly more common in female patients. This finding contradicts the studies of Hassan et al. [14] and Ahmet et al. [18], which showed that failure of segmentation and mixed defects were more common in male patients than in females. This contradiction of type distribution in sex might suggest that different ethnic groups have different pathogenesis of CS.
The incidence of intraspinal anomalies was 29.4%, which was in the range of previous studies [7, 12,13,14, 16,17,18,19]. The most common associated anomaly of intraspinal defect was diastematomyelia, with an incidence of 19.3%, followed by syringomyelia (13.2%) and tethered cord (9.1%). This result was in accordance with the studies in the Chinese population [12, 13], but contradicted the studies of Basu et al. [7], Gupta et al. [16], and Ahmet et al. [18]. This discrepancy suggests that the spectrum of associated intraspinal anomalies varies among different ethnic and geographical populations. Based on our clinical practice, a low conus without tethered cord usually presents no symptom and needs no intervention. As to tethered cord, surgical treatment is always the first choice, and the purpose of operation is to release the tethered spinal cord. Membranous diastematomyelia does not require any treatment unless the patient has obvious neurologic deficit, while the treatment of bony diastematomyelia usually needs the cooperation of orthopedic surgeons and neurosurgeons. Asymptomatic intraspinal defects can only be found by spinal MRI, so we recommend routine spinal MRI screening before surgery.
Moreover, our data indicated that female patients and patients with failure of segmentation or mixed defects have a significantly higher incidence of intraspinal defects (p < 0.001), which is consistent with previous studies. Thus, we recommend that female sex, failure of segmentation, or mixed defects should be considered as risk factors for intraspinal defects, and spinal MRI should be performed for patients with these risk factors. The association of CS and genetic factors has been proven by many previous studies. Among those genetic factors, chromosome aneuploidies, chromosomal deletion, or insertion and gene point mutation are the most common. Chromosome aneuploidies, such as trisomy 22, and chromosomal deletion or insertion, such as 10 Mb 9q33.1q34.11 deletion, are considered as more severe mutation and are associated with non-isolated vertebral malformation [22]. One the other hand, compound inheritance of a rare null mutation and a hypomorphic allele of TBX6 was confirmed to account for up to 11% of congenital scoliosis cases [9], and patients with perturbations in TBX6 dosage only present simple hemivertebrae/butterfly vertebrae at lower part of the spine and have very low incidences of intraspinal anomalies [23]. With the decrease of TBX6 expression, the spinal phenotype would become more severe [24]. As for CS types, compared with failure of formation, especially simple hemivertebrae, failure of segmentation and mixed defects are usually regarded as more severe spinal defects. Thus, we hypothesized that more severe genetic factors, such as chromosome aneuploidies, chromosomal deletion or insertion, and severe alteration of gene dosage, are associated with more severe spinal defects, including FS and MD, and higher incidence of other organ malformation, especially intraspinal defects. But this needs to be further studied and clarified.
Regarding the comparison between congenital scoliosis and idiopathic scoliosis, Johan et al. [25] systematically reviewed 8622 patients with idiopathic scoliosis (IS) in 51 studies and reported a 11.4% incidence of intraspinal defects with syrinx and Chiari malformation the most common. The author also reported intraspinal defect incidence of 16–21% in patients with early-onset scoliosis, which is higher than that in patients with late-onset scoliosis. Several other independent studies also reported the intraspinal defect incidences of 2% to 18% in IS population [26,27,28,29] and found that juvenile IS had higher incidences of intraspinal defects than adolescent IS (27% vs. 14%). The result that the incidence of intraspinal defects in patients with CS is higher than that in patients with IS but comparable to that in patients with EOS, including juvenile IS, suggests some similarities in pathogenic mechanism between CS and EOS, such as genetic factors or embryonic factors. But this hypothesis needs to be further clarified.
Apart from intraspinal anomalies, 442 patients (34.3%) had at least one associated anomaly in other organs. Cardiovascular defects were found to have an incidence of 13.7% in our study, which was within the range of early reports [7, 12, 13, 15, 17, 18]. The most frequently associated defect was valvular malformation, followed by atrial septal defect. This result was in line with Liu et al. [12] and Shen et al. [13] but inconsistent with Basu et al. [7] and Eliane et al. [17]. The incidences of atrial septal defect, ventricular septal defect, and patent ductus arteriosus were much lower in the Chinese population. We supposed that as China is still a developing country, patients with congenital heart disease from economically underdeveloped areas may prioritize treatment of heart disease; thus, they are unable to have their CS treated surgically due to economic burden.
The incidence of genitourinary defects (5.8%) was lower in our study than in previous studies [7, 11, 13, 17, 18]. In our hospital, urogenital ultrasound is a routine examination for CS patients, but intravenous pyelogram was an uncommon examination. As some defects of genitourinary system, such as duplex systems in the urogenital system, are hard to judge using ultrasound only, the incidence of genitourinary defects might be underestimated in our study. The most common genitourinary defects were single kidney and ectopic kidney. In our clinical practice, these genitourinary defects, such as unilateral kidney, seldom cause damage to renal function or require medical management in CS populations, and thus can only be found in routine screening using urinary ultrasound.
The frequency of gastrointestinal anomalies in our series (3.6%) was also lower in our study than previous studies [13, 17]. We supposed the reason was as follow. Most gastrointestinal anomalies reported in previous studies in Chinese population were hypersplenotrophy, which is not a clinically meaningful manifestation and cannot be distinguished with splenomegaly caused by other diseases. Apart from hypersplenotrophy, incidence of other gastrointestinal anomalies in our series was comparable to previous studies. In our clinical practice, patients suffering from anal or oesophagus atresia would come across relevant and severe gastrointestinal symptoms in fetal period and called for surgery as soon as possible.
Musculoskeletal anomalies (16.4%) were observed to have a higher incidence than in the report by Shen et al. (4.9%) [13]. However, in our study, most musculoskeletal anomalies were rib defects, which were not counted as musculoskeletal anomalies in their study. After excluding these rib defects, the incidence and distribution of musculoskeletal anomalies was comparable. CS individuals with rib defects tend to have more severe and progressive curves as rib defects lead to additional forces that cause extra deformities.
Regarding the interrelationship between other organ defects and sex, Ahmet et al. [18] reported no significant association between cardiac and renal defects and sex. This study expanded the analysis into more systems and observed a similar finding: none of the cardiovascular, genitourinary, or gastrointestinal defects was significantly associated with sex, although female patients did have a higher incidence of musculoskeletal defects.
In regard to the interrelationship between vertebral anomaly types and associated defects, patients with failure of segmentation or mixed defects were found to have a higher incidence of anomalies in other organs. Specifically, other than intraspinal defects, genitourinary, and musculoskeletal defects were found to have significantly higher incidences in patients with failure of segmentation and mixed defects. This significant interrelationship between associated anomalies and vertebral anomaly types may indicate that patients with failure of segmentation or mixed failure had much greater embryonic injury [7], either genetic or environmental, in the development of the spine, which had a more serious influence on adjacent organs.
The significant interrelationship between intraspinal defects and musculoskeletal defects observed in our study has never been reported. In our series, most musculoskeletal defects were rib abnormalities such as fused rib or rib absence. The rib is an important component of the bony structure of the thorax, which is derived from somites in the early embryonic stage [30]. The same embryonic origin of the rib and vertebrae and the close correlation of the development of the notochord and somites might give rise to the strong interrelationship of vertebral anomalies, intraspinal defects, and musculoskeletal defects found in our study.
Another interesting finding regarding the interrelationship between different organ defects is that cardiovascular, genitourinary, and gastrointestinal defects were strongly interrelated with each other, which is a new discovery. This interrelationship among cardiac, genitourinary, and gastrointestinal defects might be explained by their germ layer origins and common developmental process. For example, the gastrointestinal system and urinary tract both originate from the endoderm, while the cardiovascular system, reproductive system, and kidney all derive from the mesoderm [31]. In addition, the studies on VACTERL association, the phenotype spectrum of which covers vertebral defects, anal atresia, cardiac defects, and renal defects, might provide some explanation for this interrelationship. The familial clustering phenomenon of VACTERL was found by Solomon et al. [32], suggesting a genetic role in its causality. Later, Hilger et al. [33] revealed ZIC3 and FOXF1 to be related to VACTERL association. These genetic factors also help to explain the interrelationship in our study. Certain signaling pathways might also be involved. TGF-β family signaling functions in the development of both the mesoderm and endoderm and thus has the potential to affect the normal morphogenesis of certain organs [34].
Furthermore, we found an obvious decrease in the incidences of intraspinal and musculoskeletal defects from 2010 to 2019. The distribution of vertebral anomaly types was also observed to change apparently during these ten years. In short, more patients with failure of formation and fewer patients with failure of segmentation were surgically treated in our center. This tendency might be explained by either the distribution shift of vertebral anomaly types in our population or the preference of patients in our hospital. As intraspinal and musculoskeletal defects were strongly associated with different vertebral anomaly types, the distribution shift of vertebral anomaly types might contribute to the decrease in their incidence. As expected, we noted a strong negative correlation between the tendency of the proportion of failure of formation and the trend of incidences of intraspinal and musculoskeletal defects (Fig. 4c). This result further demonstrated that patients with failure of formation could present with a lower incidence of intraspinal and musculoskeletal defects in a dynamic model.
Generally, our study has two major strengths. First, to our knowledge, this is one of the largest CS cohorts in the Chinese population. Second, we not only comprehensively analyzed the incidences and interrelationships but also first introduced the trends of vertebral anomaly types and all common associated anomalies in the last decade. However, as this is a retrospective study of extracted medical records, the quality and reliability of this study were largely influenced by the recorders, imaging interpreters and the medical record quality.
In a conclusion, our study found that associated anomalies, especially intraspinal anomalies, had much higher incidences in female patients (36.5% vs. 29.4% for intraspinal anomalies), patients with failure of segmentation (45.4% vs. 29.4%), and patients with mixed defects (40.5% vs. 29.4%). Thus, female sex, failure of segmentation, and mixed defects could be considered risk factors for CS patients, which deserves more attention from surgeons in medical management and prenatal consultation. Based on these results and our clinical experience, we recommended that a thorough screening for associated anomalies be performed for outpatients with one or more risk factors and all inpatients before surgery (Fig. 5). However, as genetic factors may play a role, the incidences and interrelationship of specific associated anomalies might be discrepant in different ethnicities. Therefore, it is important to run similar studies to provide further clarification and comparison on such findings in different ethnicities.

Diagnostic algorithm
References
Giampietro PF, Blank RD, Raggio CL et al (2003) Congenital and idiopathic scoliosis: clinical and genetic aspects. Clin Med Res 1(2):125–136. https://doi.org/10.3121/cmr.1.2.125
Batra S, Ahuja S (2008) Congenital scoliosis: management and future directions. Acta Orthop Belg 74(2):147–160
Giampietro PF, Raggio CL, Blank RD, McCarty C, Broeckel U, Pickart MA (2013) Clinical, genetic and environmental factors associated with congenital vertebral malformations. Mol Syndromol 4(1–2):94–105. https://doi.org/10.1159/000345329
Li Z, Yu X, Shen J (2015) Environmental aspects of congenital scoliosis. Environ Sci Pollut Res Int 22(8):5751–5755. https://doi.org/10.1007/s11356-015-4144-0
Chen Y, Liu Z, Chen J et al (2016) The genetic landscape and clinical implications of vertebral anomalies in VACTERL association. J Med Genet 53(7):431–437. https://doi.org/10.1136/jmedgenet-2015-103554
Giampietro PF (2012) Genetic aspects of congenital and idiopathic scoliosis. Scientifica (Cairo) 2012:152365. https://doi.org/10.6064/2012/152365
Basu PS, Elsebaie H, Noordeen MH (2002) Congenital spinal deformity: a comprehensive assessment at presentation. Spine (Phila Pa 1976) 27(20):2255–2259. https://doi.org/10.1097/00007632-200210150-00014
Hensinger RN (2009) Congenital scoliosis: etiology and associations. Spine (Phila Pa 1976) 34(17):1745–1750. https://doi.org/10.1097/BRS.0b013e3181abf69e
Wu N, Ming X, Xiao J, Wu Z et al (2015) TBX6 null variants and a common hypomorphic allele in congenital scoliosis. N Engl J Med 372(4):341–350. https://doi.org/10.1056/NEJMoa1406829
Beals RK, Robbins JR, Rolfe B (1993) Anomalies associated with vertebral malformations. Spine (Phila Pa 1976) 18(10):1329–1332. https://doi.org/10.1097/00007632-199308000-00012
Rai AS, Taylor TK, Smith GH, Cumming RG, Plunkett-Cole M (2002) Congenital abnormalities of the urogenital tract in association with congenital vertebral malformations. J Bone Joint Surg Br 84(6):891–895. https://doi.org/10.1302/0301-620x.84b6.11814
Liu YT, Guo LL, Tian Z, Zhu WL, Yu B, Zhang SY, Qiu GX (2011) A retrospective study of congenital scoliosis and associated cardiac and intraspinal abnormities in a Chinese population. Eur Spine J 20(12):2111–2114. https://doi.org/10.1007/s00586-011-1818-2
Shen J, Wang Z, Liu J, Xue X, Qiu G (2013) Abnormalities associated with congenital scoliosis: a retrospective study of 226 Chinese surgical cases. Spine (Phila Pa 1976) 38(10):814–818. https://doi.org/10.1097/BRS.0b013e31827ed125
Ghandhari H, Tari HV, Ameri E, Safari MB, Fouladi DF (2015) Vertebral, rib, and intraspinal anomalies in congenital scoliosis: a study on 202 Caucasians. Eur Spine J 24(7):1510–1521. https://doi.org/10.1007/s00586-015-3833-1
Bozcali E, Ucpunar H, Sevencan A, Balioglu MB, Albayrak A, Polat V (2016) A retrospective study of congenital cardiac abnormality associated with scoliosis. Asian Spine J 10(2):226–230. https://doi.org/10.4184/asj.2016.10.2.226
Gupta N, Rajasekaran S, Balamurali G, Shetty A (2016) Vertebral and intraspinal anomalies in Indian population with congenital scoliosis: a study of 119 consecutive patients. Asian Spine J 10(2):276–281. https://doi.org/10.4184/asj.2016.10.2.276
Beauregard-Lacroix E, Tardif J, Camurri MV et al (2017) Retrospective analysis of congenital scoliosis: associated anomalies and genetic diagnoses. Spine (Phila Pa 1976) 42(14):E841–E847. https://doi.org/10.1097/BRS.0000000000001983
Sevencan A, Misir A, Ucpunar H, Balioglu MB, Gur V, Akinci S (2019) The incidence and interrelationship of concomitant anomalies in congenital scoliosis. Turk Neurosurg 29(3):404–408. https://doi.org/10.5137/1019-5149.JTN.24429-18.2
Mohanty SP, Pai Kanhangad M, Narayana Kurup JK, Saiffudeen S (2020) Vertebral, intraspinal and other organ anomalies in congenital scoliosis. Eur Spine J 29(10):2449–2456. https://doi.org/10.1007/s00586-020-06450-3
McMaster MJ, Ohtsuka K (1982) The natural history of congenital scoliosis. A study of two hundred and fifty-one patients. J Bone Joint Surg Am 64(8):1128–47
Winter RB, Moe JH, Wang JF (1973) Congenital kyphosis. Its natural history and treatment as observed in a study of one hundred and thirty patients. J Bone Joint Surg Am 55(2):223–256
Lemire GT, Beauregard-Lacroix E, Campeau PM et al (2020) Retrospective analysis of fetal vertebral defects: associated anomalies, etiologies, and outcome. Am J Med Genet A 182(4):664–672. https://doi.org/10.1002/ajmg.a.61468
Liu J, Wu N, Deciphering Disorders Involving S, study CO, Yang N et al (2019) TBX6-associated congenital scoliosis (TACS) as a clinically distinguishable subtype of congenital scoliosis: further evidence supporting the compound inheritance and TBX6 gene dosage model. Genet Med 21(7):1548–1558. https://doi.org/10.1038/s41436-018-0377-x
Chen W, Lin J, Wang L, Li X, Zhao S et al (2020) TBX6 missense variants expand the mutational spectrum in a non-Mendelian inheritance disease. Hum Mutat 41(1):182–195. https://doi.org/10.1002/humu.23907
Heemskerk JL, Kruyt MC, Colo D, Castelein RM, Kempen DHR (2018) Prevalence and risk factors for neural axis anomalies in idiopathic scoliosis: a systematic review. Spine J 18(7):1261–1271. https://doi.org/10.1016/j.spinee.2018.02.013
Winter RB, Lonstein JE, Heithoff KB, Kirkham JA (1997) Magnetic resonance imaging evaluation of the adolescent patient with idiopathic scoliosis before spinal instrumentation and fusion. A prospective, double-blinded study of 140 patients. Spine (Phila Pa 1976) 22(8):855–858. https://doi.org/10.1097/00007632-199704150-00005
Do T, Fras C, Burke S, Widmann RF, Rawlins B, Boachie-Adjei O (2001) Clinical value of routine preoperative magnetic resonance imaging in adolescent idiopathic scoliosis. A prospective study of three hundred and twenty-seven patients. J Bone Joint Surg Am 83(4):577–579. https://doi.org/10.2106/00004623-200104000-00014
Inoue M, Minami S, Nakata Y et al (2005) Preoperative MRI analysis of patients with idiopathic scoliosis: a prospective study. Spine (Phila Pa 1976) 30(1):108–114. https://doi.org/10.1097/01.brs.0000149075.96242.0e
Rajasekaran S, Kamath V, Kiran R, Shetty AP (2010) Intraspinal anomalies in scoliosis: an MRI analysis of 177 consecutive scoliosis patients. Indian J Orthop 44(1):57–63. https://doi.org/10.4103/0019-5413.58607
Kaplan KM, Spivak JM, Bendo JA (2005) Embryology of the spine and associated congenital abnormalities. Spine J 5(5):564–576. https://doi.org/10.1016/j.spinee.2004.10.044
Kiecker C, Bates T, Bell E (2016) Molecular specification of germ layers in vertebrate embryos. Cell Mol Life Sci 73(5):923–947. https://doi.org/10.1007/s00018-015-2092-y
Solomon BD, Pineda-Alvarez DE, Raam MS, Cummings DA (2010) Evidence for inheritance in patients with VACTERL association. Hum Genet 127(6):731–733. https://doi.org/10.1007/s00439-010-0814-7
Hilger AC, Halbritter J, Pennimpede T et al (2015) Targeted resequencing of 29 candidate genes and mouse expression studies implicate ZIC3 and FOXF1 in human VATER/VACTERL association. Hum Mutat 36(12):1150–1154. https://doi.org/10.1002/humu.22859
Zinski J, Tajer B, Mullins MC (2018) TGF-beta family signaling in early vertebrate development. Cold Spring Harb Perspect Biol 10 (6).https://doi.org/10.1101/cshperspect.a033274
Funding
The study was supported by grants from National Natural Science Foundation of China (No. 81972037, 81902178), National Key Research & Development Program of China (No. 2017YFC1104902), Beijing Natural Science Foundation (No. L192015), Fundamental Research Funds for the Central Universities (No. 3332019021), and China Postdoctoral Science Foundation (No. 2020M670008ZX).
Author information
Authors and Affiliations
Contributions
Conceptualization: Guanfeng Lin and Jianguo Zhang; methodology: Guanfeng Lin, Xiran Chai and Yang Yang; formal analysis and investigation: Guanfeng Lin, Xiran Chai; writing—original draft preparation: Guanfeng Lin, Xiran Chai; writing—review and editing: Guanfeng Lin, Xiran Chai, Shengru Wang, Yang Yang, Jianxiong Shen, and Jianguo Zhang; funding acquisition: Yang Yang, Shengru Wang, and Jianguo Zhang; resources: Jianxiong Shen, Jianguo Zhang; supervision: Jianguo Zhang.
Corresponding author
Ethics declarations
Ethics approval
Approval for the study was obtained from the ethics committee at Peking Union Medical College Hospital.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Lin, G., Chai, X., Wang, S. et al. Cross-sectional analysis and trend of vertebral and associated anomalies in Chinese congenital scoliosis population: a retrospective study of one thousand, two hundred and eighty nine surgical cases from 2010 to 2019. International Orthopaedics (SICOT) 45, 2049–2059 (2021). https://doi.org/10.1007/s00264-021-05061-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-021-05061-x