
Abstract
Purpose
One of the most widespread diseases of children’s orthopaedic problems is flatfoot. If conservative therapy failed, surgical treatment would be indicated. Lateral calcaneal lengthening (LCL) and subtalar arthroereisis (SA) are two types of operations used to correct symptomatic flexible flatfoot (FFF). The purpose of this study is to compare the functional and radiographic features of these two surgical procedures.
Patients and methods
In this prospective randomized clinical trial study, we recruited 66 patients between 2018 and 2019. For clinical assessment, American Orthopedics Foot and Ankle Society (AOFAS), visual analog scale (VAS), subtalar motion, presence of medial longitudinal arch, and family satisfaction were measured. Evaluation of radiographic angles was based on AP (AP Tal-1Met) and Lat (Lat Tal-1Met) view of Talus-1st metatarsal angle (Meary’s angle) and calcaneal pitch.
Result
There was no significant difference between the two types of surgery regarding Lat Tal-1Met and AP Tal-1Met. The significantly larger angle in the LCL group was calcaneal pitch (P value < 0.001). AOFAS significantly increased from 68.71 ± 5.70 to 87.87 ± 7.14 (P value < 0.001) and from 67.28 ± 6.01 to 86.14 ± 7.56 (P value < 0.001) in LCL and SA respectively. Family satisfaction was significantly higher in the SA (8.14 ± 0.97) comparing to LCL (7.29 ± 0.86) at the latest follow-up (P value < 0.001).
Conclusion
While both groups have substantial improvement in clinical and radiographic aspects, the SA technique is less-invasive, rapid symptom relief, and has early weight-bearing capacity.
Trial registration
IRCT20180823040853N1
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
One of the most common complaints in paediatric orthopaedic surgery is flatfoot. Most cases are asymptomatic and do not need any treatment. If being present, symptoms may be resolved by conservative therapy. If it fails, the surgical procedure will be indicated. Boys are generally affected two times more than girls [1,2,3].
There are three clinical types of flatfoot: flexible flatfoot (FFF), FFF with a short Achilles tendon, and rigid flatfoot most commonly associated with tarsal coalitions [4].
Flexible flatfoot (FFF) pain is mainly related to the activity [1]. The deformity will appear with a weight-bearing position in which we can see the low or absence of medial arch, valgus hindfoot, and forefoot supination. In FFF at the terminal phase of stance, the subtalar joint is prone while in the normal foot, the joint is supinated in the propulsive phase [5, 6].
In 1975, Evans described lateral calcaneal lengthening (LCL) for the first time [7] and it was modified by Mosca in 1995 [8]. Several papers have shown this technique has good clinical outcomes [9,10,11,12,13]. Some of the most common complications reported are calcaneocuboid joint subluxation [7, 8, 13,14,15], delayed or non-union [16], overcorrection, and graft migration [13, 15].
Another technique is the subtalar arthroereisis (SA) via calcaneo-stop, an implant that restricts subtalar eversion firstly described by Alvarez in 1970 [17]. Implants have different types: metal, bone, or synthetic [1]. Advocates described SA as the minimally invasive procedure and opponents explained it as the surgery with a foreign body in the foot for long-life [18]. Some of the most common complications are sinus tarsi pain, under correction, implant migration, infection, and overcorrection [19,20,21]. Other complications including subtalar problem, graft donor site problem, hardware prominence, and nerve injury for LCL, and infection and wound problem for both operations was mentioned [3].
Many papers are confirming the effectiveness of both operations for correcting an FFF. Nonetheless, limited evidence is available regarding the comparison of these two types of operation. We decided to recognize different aspects of these two procedures comparatively in a clinical trial setting for better-selecting decisions. Our goal is to compare clinical and radiographic results between them. These would be evaluated by pre-operative and post-operative radiographic and clinical criteria. We hypothesized that both surgical techniques will relieve flatfoot symptoms and correct radiographic angles, and they will be equivalent in their results.
Method
Randomization and patient selection
This prospective, randomized clinical trial study has a parallel design with equal randomization (Fig. 1). Children with symptomatic flexible flatfoot (FFF) visited between 2018 and 2019 were recruited. All of them complained of painful flatfoot and they had failed conservative treatment like physiotherapy and adaptive footwear lasting at least six months. Clinical and radiographic examination was used for diagnosis. In most children, the pain was felt in the medial of midfoot or at sinus tarsi. During activities, they were suffering from fatigue in the foot. All cases had low longitudinal arch gate phases and hindfoot valgus (Fig. 2). The radiographic study was used to confirm clinical signs and symptoms. There is a lack of consensus about the normal range of each angle; nonetheless, we consider 10° >, 13° >, 17° < for Meary’s angle in AP and lateral plane, and calcaneal pitch respectively [22].

CONSORT 2010 flow diagram

Pre-operative standing photograph
Patients with underlying bone metabolic disease, cerebral palsy, myelomeningocele, arthrogryposis, parathyroid problems, history of surgery, trauma or cancer, and more than 12 years old were excluded. The age of participants ranged from eight to 12.
Participants were randomly assigned to the LCL group or SA with a computer-generated random sequence. The block randomization method was used with a block size of four.
A physician checked the patients for eligibility and another allocated them to the specific group using sequentially numbered, opaque, sealed envelopes (SNOSE). It was not possible to blind the surgeon or participants. The person who analyzed the data was blinded.
This study was registered at irct.ir (IRCT20180823040853N1) and it was approved by the Ethics Committee of Isfahan University of Medical Science (IR.MUI.MED.REC.1398.415). Written informed consent was obtained from all parents and legal representatives of children.
According to the equation for parallel design trials, considering α = 0.05, β = 0.10, and a standardized effect size of ∆ = 0.85, we reached 30 participants per group. Considering the dropout rate of 20%, 36 subjects were recruited in each group.
Surgical intervention
In the LCL group, patients were positioned supine under general anaesthesia. We made a 3-cm incision over the anterolateral of the calcaneus. The sural nerve was preserved. Peroneus longus and brevis were left intact. After exposing the calcaneocuboid joint, the anterior and medial facet of the calcaneus was identified. We began performing osteotomy about 1.5 cm proximal to the calcaneocuboid joint parallel to the calcaneocuboid joint and continuing between the medial and anterior facet interval. The laminar spreader was inserted into the osteotomy site to measure the graft size. Tricortical wedge-shaped bone allograft from the patella bone was placed on the site. Gastrocsoleus recession was performed in two patients. The short leg cast was applied for about six weeks. Weight-bearing was allowed three to four weeks after the operation. All the procedures were performed by the same orthopaedic surgeon. (Fig. 3a).

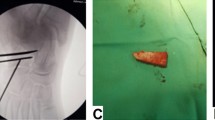
a LCL post-operative photography. b SA during operation and post-operative photography
In the SA group, all patients had a supine position under general anesthesia. We incised the lateral area of the sinus tarsi with a length of 1.5 cm. The soft tissues were dissected gently. Then, the foot was positioned internally rotated for better access to sinus tarsi. The cancellus screw with a size of 24–26 mm depending on the patient’s age was inserted about 1 cm medial to the lateral part of the calcaneus bone as vertical as possible. The screw’s head had to stick out enough to prevent excessive subtalar eversion. Afterward, with CR (computed radiography), the correct placement of the screw was checked. In one of our patients, we performed the gastrocsoleus recession. The short leg cast was applied for about six weeks like LCL. We permitted all patients weight-bearing 48–72 hours after surgery. All the procedures were performed by the same orthopaedic surgeon (Fig. 3b).
Follow-up assessment
Clinical assessment was carried out by the American Orthopedics Foot and Ankle Society (AOFAS) Ankle-hindfoot questionnaire [23] and visual analog scale (VAS) for pain measurement pre-operatively and in the latest follow-up. Moreover, we evaluated forefoot and hindfoot, subtalar motion, and the presence of medial longitudinal arc postoperatively. The forefoot assessment was in the transverse and frontal plane. The hindfoot evaluation was in the frontal and sagittal plane. The family was asked for expressing their satisfaction by a number 1 to 10 after surgery. The more satisfied, the higher number.
Radiographic evaluation was done in X-ray of AP and Lat view of the foot. The Talus-1st metatarsal angle (Meary’s angle) in AP (AP Tal-1Met) and Lat (Lat Tal-1Met) view, and the calcaneal pitch were measured pre- and post-operatively (Figs. 4 and 5). The Meary’s angle is between the line that passes from the centre of the longitudinal axes of the talus and the first metatarsal. Calcaneal pitch is an angle between the calcaneal inclination axis and horizontal surface on weight-bearing lateral foot radiography.

LCL radiography. a Pre-operative AP Tal-1Met. b Post-operative AP Tal-1Met. c Pre-operative Lat Tal-1Met and calcaneal pitch. d Post-operative Lat Tal-1Met and calcaneal pitch

SA radiography. a Pre-operative AP Tal-1Met. b Post-operative AP Tal-1Met. c Pre-operative Lat Tal-1Met and calcaneal pitch. d Post-operative Lat Tal-1Met and calcaneal pitch
An examiner blinded to group allocation evaluated forefoot and hindfoot alignment, VAS, subtalar motion, family satisfaction, presence of medial longitudinal, and radiographic parameters at about 12 months following operation time.
Statistical analyses
Data was imported to the Statistical package for social science (SPSS) software version 22.0 (IBM Corp. USA). Results are expressed as mean ± standard deviation. Chi-square and t test were used to analyze the baseline variables. A paired t test was used for comparing continuous data in each group pre-operative and post-operative. Analysis of covariance (ANCOVA) was used for comparing continuous variables when adjustment was made for pre-operative AOFAS, AP Tal-1Met, Lat Tal-1Met, calcaneal pitch, and VAS.
Results
We operated a total number of 66 patients, 31 (47%) and 35 (53%), in LCL and SA respectively. The operations were unilateral in all patients. The majority of patients were male (63.6%) while the sex distribution was not significantly different between the two groups. The mean ages of children in LCL and SA were 10.19 ± 1.54 and 10.06 ± 1.68 respectively and there was no significant difference between the age of the two groups (Table 1). The time between pre-operative assessment and post-operative follow-up was 17.6 months on average (range 11–20 months).
Clinical assessment
Both types of surgery demonstrated considerable improvement in clinical parameters. The mean AOFAS significantly increased from 68.71 ± 5.70 to 87.87 ± 7.14 (P value < 0.001) and from 67.28 ± 6.01 to 86.14 ± 7.56 (P value < 0.001) in LCL and SA respectively. After adjustment for pre-AOFAS, post-AOFAS was not significantly different between the two operations (P value = 0.431). Family satisfaction was significantly higher in SA (8.14 ± 0.97) than LCL (7.29 ± 0.86) at latest follow-up (P value < 0.001) (Table 2). In both groups, hindfoot valgus improved significantly post-operatively. However, it was not significantly different between the two groups (P value = 0.574) (Table 2).
Radiographic measures
In our study of radiographic parameters, AP Tal-1Met decreased statistically by a mean of 15.81 ± 2.84 and 16.80 ± 2.96 in LCL and SA respectively (P value < 0.001). Lat Tal-1Met decreased significantly by a mean of 14.39 ± 2.67 and 15.14 ± 2.14 in LCL and SA respectively (P value < 0.001). Calcaneal pitch angle increased significantly by a mean of 8.19 ± 2.17 and 5.31 ± 1.31 in LCL and SA respectively (P value < 0.001); however, we found no significant difference between the two types of surgery regarding Lat Tal-1Met and AP Tal-1Met (Table 3). The sole angle which was significantly larger in the LCL group was calcaneal pitch (P value < 0.001) and this is consistent with a previous study [2].
Complications
In the LCL, graft displacement 1 month after the operation in one girl caused pain. After two weeks of conservative treatment, her pain was alleviated. However, she has the lowest family satisfaction rate in LCL.
In the SA group, one patient complained about persistent pain seven months after surgery. Therefore, she underwent a removal screw. She recovered four months after the second procedure.
Discussion
SA via calcaneo-stop is widely utilized in European countries and LCL is adopted in the USA [24]. In SA, a device is implanted to correct alignment between talus and calcaneus generally [24]. SA was reported as minimally invasive for treatment of FFF [24, 25] and it changes the place of body load to the lateral column [25] and it prevents hindfoot eversion. LCL reduces forefoot abduction, midfoot pronation, and hindfoot valgus [26]. We believe that the best age for surgery is eight to 12 years which is mentioned in previous studies [25, 26]. We found that clinical and radiographic assessment improved one year post-operatively in both groups of surgery. Nevertheless, family satisfaction was significantly better in SA and calcaneal pitch angle increased in LCL more than SA statistically.
Previous studies have shown that each type of surgery would affect different parts of the foot. LCL would correct midfoot transverse plane deformity due to a greater decrease in the Tal-1Met angle [2]. However, we found that there is no significant difference in this angle in a 1-year follow-up between two types of surgery.
One study [27] suggested that calcaneal pitch increases statistically in SA in children which is consistent with our results. However, other studies stated that this angle in SA had been even decreased or not changed postoperatively [2, 28]. The reason for this contrast might be since our technique of operation, which was calcaneo-stop for the SA, differed from these studies. Nevertheless, LCL has a greater increase in the calcaneal pitch angle significantly. This outcome is consistent with a review study [3].
The review article [3] also declared that the AOFAS improvement was significantly higher in LCL comparing to SA. The method of SA procedure in this study was placing an implant in sinus tarsi while we had a contradicting surgical method, calcaneo-stop. For comparing postoperative AOFAS, we adjusted it with the pre-operative variable. However, this study compared the mean of differences between the minimum and maximum value of AOFAS. These two reasons might cause different results.
Before this study, the surgeon had considered LCL for severe forefoot abduction. Although some studies offered to consider LCL for this severity, we found that there is no difference in forefoot abduction after surgery.
As we mentioned, two to three days after surgery, all patients in SA were permitted for weight-bearing. As a result, we offer to operate both feet concurrently in SA type because of good rehabilitation, short recovery time, and satisfaction rate. However, for LCL, we recommend operating on each side separately at different times.
Although the calcaneal pitch angle was significantly higher in LCA after surgery, it did not cause any clinical improvement more than SA. Due to the similar clinical and radiological assessment, rapid symptom relief, early weight-bearing capacity, better family satisfaction, and minimally invasive of SA, we prefer SA in most cases for the future.
The first strength of the current study was comparing the two FFF surgery techniques which has not been compared before in radiological and clinical aspects. The second strength was the random allocation of patients which caused more reliable results.
Our limitation in this study was the short-term results of comparing these types of surgery which was 1 year after operation and patients have to be assessed several years after operation for comparing long-term outcomes.
Conclusion
The finding of this study states that there is no significant difference between the two groups in clinical and radiographic improvement except family satisfaction and calcaneal pitch; nonetheless, the SA technique is less-invasive, rapid symptom relief, and has early weight-bearing capacity.
References
Bouchard M, Mosca VS (2014) Flatfoot deformity in children and adolescents: surgical indications and management. J Am Acad Orthop Surg 22:623–632. https://doi.org/10.5435/JAAOS-22-10-623
Chong DY, Macwilliams BA, Hennessey TA, Teske N, Stevens PM (2015) Prospective comparison of subtalar arthroereisis with lateral column lengthening for painful flatfeet. J Pediatr Orthop B 24:345–353. https://doi.org/10.1097/BPB.0000000000000179
Suh DH, Park JH, Lee SH, Kim HJ, Park YH, Jang WY, Baek JH, Sung HJ, Choi GW (2019) Lateral column lengthening versus subtalar arthroereisis for paediatric flatfeet: a systematic review. Int Orthop 43:1179–1192. https://doi.org/10.1007/s00264-019-04303-3
Harris RI, Beath T (1974) Army Foot Survey: An Investigation of Foot Ailments in Canadian Soldiers. Ottawa, Ontario, Canada: National Research Council of Canada
Caravaggi P, Lullini G, Berti L, Giannini S, Leardini A (2018) Functional evaluation of bilateral subtalar arthroereisis for the correction of flexible flatfoot in children: 1-year follow-up. Gait Posture 64:152–158. https://doi.org/10.1016/j.gaitpost.2018.06.023
Faldini C, Mazzotti A, Panciera A, Perna F, Stefanini N, Giannini S (2018) Bioabsorbable implants for subtalar arthroereisis in pediatric flatfoot. Musculoskelet Surg 102:11–19. https://doi.org/10.1007/s12306-017-0491-y
Evans D (1975) Calcaneo-valgus deformity. J Bone Joint Surg (Br) 57:270–278
Mosca VS (1995) Calcaneal lengthening for valgus deformity of the hindfoot. Results in children who had severe, symptomatic flatfoot and skewfoot. J Bone Joint Surg Am 77:500–512. https://doi.org/10.2106/00004623-199504000-00002
Andreacchio A, Orellana CA, Miller F, Bowen TR (2000) Lateral column lengthening as treatment for planovalgus foot deformity in ambulatory children with spastic cerebral palsy. J Pediatr Orthop 20:501–505
Dumontier TA, Falicov A, Mosca V, Sangeorzan B (2005) Calcaneal lengthening: investigation of deformity correction in a cadaver flatfoot model. Foot Ankle Int 26:166–170. https://doi.org/10.1177/107110070502600209
Sangeorzan BJ, Mosca V, Hansen ST Jr (1993) Effect of calcaneal lengthening on relationships among the hindfoot, midfoot, and forefoot. Foot Ankle 14:136–141. https://doi.org/10.1177/107110079301400305
Yoo WJ, Chung CY, Choi IH, Cho TJ, Kim DH (2005) Calcaneal lengthening for the planovalgus foot deformity in children with cerebral palsy. J Pediatr Orthop 25:781–785. https://doi.org/10.1097/01.bpo.0000184650.26852.37
Zeifang F, Breusch SJ, Döderlein L (2006) Evans calcaneal lengthening procedure for spastic flexible flatfoot in 32 patients (46 feet) with a followup of 3 to 9 years. Foot Ankle Int 27:500–507. https://doi.org/10.1177/107110070602700704
Adams SB Jr, Simpson AW, Pugh LI, Stasikelis PJ (2009) Calcaneocuboid joint subluxation after calcaneal lengthening for planovalgus foot deformity in children with cerebral palsy. J Pediatr Orthop 29:170–174. https://doi.org/10.1097/BPO.0b013e3181982c33
Moraleda L, Salcedo M, Bastrom TP, Wenger DR, Albiñana J, Mubarak SJ (2012) Comparison of the calcaneo-cuboid-cuneiform osteotomies and the calcaneal lengthening osteotomy in the surgical treatment of symptomatic flexible flatfoot. J Pediatr Orthop 32:821–829. https://doi.org/10.1097/BPO.0b013e3182648c74
Thomas RL, Wells BC, Garrison RL, Prada SA (2001) Preliminary results comparing two methods of lateral column lengthening. Foot Ankle Int 22:107–119. https://doi.org/10.1177/107110070102200205
Pavone V, Vescio A, Canavese F, Costa D, Sessa G, Testa G (2019) Effects of body weight on the clinical and radiological outcomes of children with flexible flatfeet managed with the 'calcaneo-stop' procedure. J Pediatr Orthop B 28:228–234. https://doi.org/10.1097/BPB.0000000000000590
Evans AM, Rome K (2011) A Cochrane review of the evidence for non-surgical interventions for flexible pediatric flat feet. Eur J Phys Rehabil Med 47:69–89
Megremis P, Megremis O (2019) Arthroereisis for symptomatic flexible flatfoot deformity in young children: radiological assessment and short-term follow-up. J Foot Ankle Surg 58:904–915. https://doi.org/10.1053/j.jfas.2019.01.012
Metcalfe SA, Bowling FL, Reeves ND (2011) Subtalar joint arthroereisis in the management of pediatric flexible flatfoot: a critical review of the literature. Foot Ankle Int 32:1127–1139. https://doi.org/10.3113/fai.2011.1127
Mosca VS (2010) Flexible flatfoot in children and adolescents. J Child Orthop 4:107–121. https://doi.org/10.1007/s11832-010-0239-9
Davids JR, Gibson TW, Pugh LI (2005) Quantitative segmental analysis of weight-bearing radiographs of the foot and ankle for children: normal alignment. J Pediatr Orthop 25:769–776. https://doi.org/10.1097/01.bpo.0000173244.74065.e4
Sayyed-Hosseinian SH, Hassankhani GG, Bagheri F, Alavi N, Shojaie B, Mousavian A (2018) Validation of the Persian version of the American Orthopedic Foot and Ankle Society Score (AOFAS) Questionnaire. Arch Bone Jt Surg 6:233–239
Giannini S, Cadossi M, Mazzotti A, Persiani V, Tedesco G, Romagnoli M, Faldini C (2017) Bioabsorbable calcaneo-stop implant for the treatment of flexible flatfoot: a retrospective cohort study at a minimum follow-up of 4 years. J Foot Ankle Surg 56:776–782. https://doi.org/10.1053/j.jfas.2017.02.018
Jerosch J, Schunck J, Abdel-Aziz H (2009) The stop screw technique—a simple and reliable method in treating flexible flatfoot in children. Foot Ankle Surg 15:174–178. https://doi.org/10.1016/j.fas.2009.01.004
Viegas GV (2003) Reconstruction of the pediatric flexible planovalgus foot by using an Evans calcaneal osteotomy and augmentative medial split tibialis anterior tendon transfer. J Foot Ankle Surg 42:199–207. https://doi.org/10.1016/s1067-2516(03)70029-5
Pavone V, Vescio A, Di Silvestri CA, Andreacchio A, Sessa G, Testa G (2018) Outcomes of the calcaneo-stop procedure for the treatment of juvenile flatfoot in young athletes. J Child Orthop 12:582–589. https://doi.org/10.1302/1863-2548.12.180032
Morris C, Liabo K, Wright P, Fitzpatrick R (2007) Development of the Oxford ankle foot questionnaire: finding out how children are affected by foot and ankle problems. Child Care Health Dev 33:559–568. https://doi.org/10.1111/j.1365-2214.2007.00770.x
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical approval
This study was approved by the Ethics Committee of Isfahan University of Medical Science (IR.MUI.MED.REC.1398.415) and it was registered at irct.ir (IRCT20180823040853N1).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Tahririan, M.A., Ramtin, S. & Taheri, P. Functional and radiographic comparison of subtalar arthroereisis and lateral calcaneal lengthening in the surgical treatment of flexible flatfoot in children. International Orthopaedics (SICOT) 45, 2291–2298 (2021). https://doi.org/10.1007/s00264-020-04899-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-020-04899-x