
Abstract
Introduction
Nail dynamization is one of the proposed surgical options to manage femoral shaft non-union. This study aims to assess the efficacy and the ideal timing for dynamization in patients with femoral shaft delayed union or non-union.
Material and methods
Sixty-eight patients (38 male and 30 female, mean age 36.85 years old, range 22–58) were recruited. The patients were divided into three groups according to the fracture healing time: groupa A, fracture healing occurred within nine months; group B, fracture healing occurred between nine and 12 months; and group C, fracture healing after 12 months or secondary procedure needed for union. Callus-to-diaphysis ratio was calculated on femur X-rays at the time of dynamization.
Results
In 30 patients out of 68, the fracture healing was observed at nine month follow-up; in 26 patients, the fracture healed within 12 months; eight fractures healed in more than 12 months and only four fractures required a secondary procedure for union. Dynamization was successful in 64 patients out of 68 (94.12%). The mean callus-diaphysis ratio was significantly different in group A (p = 0.001) and in group B (p = 0.03), compared with group C. The timing of dynamization resulted significantly different between the three groups. Linear regression analysis revealed that nail dynamization should be performed between three and six months after trauma. The optimal callus-to-diaphysis ratio should be comprised between 1.47 and 1.19, at the time of dynamization.
Discussion
Nail dynamization revealed safe and effective in the treatment of femoral delayed union and non-union. It should be considered as a first-line treatment for femoral non-union or delayed union.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Femoral shaft fractures are a quite common injury in orthopaedic practice, with a reported incidence of 37.1 per 100,000 person-years in the USA [1]. This fracture pattern can be caused by high-energy traumas, such as pedestrian accidents, motor vehicle accidents, sports injuries, and falls from a height, but it can also be found in low-energy traumas, mainly in older adults with osteoporotic bone [2] and from metastatic bone disease [3].
Closed reduction with a reamed intramedullary nail is widely considered as the treatment of choice for femoral shaft fractures [2, 4,5,6], since it has several advantages, including minimal accesses; respect for soft tissues and fracture haematoma; high union rate, ranging from 90 to 100%; and a lower post-operative infection rate, compared to open surgery [4, 5, 7].
However, delayed union or non-union occur even in femoral shaft fractures treated with reamed intramedullary nailing [5, 7]. Non-union is defined, according to the Food and Drugs Administration (FDA), as a fractured bone that has not completely healed within nine months of injury and that has not shown progression towards healing over three consecutive months on serial radiographs [7]. Femoral shaft non-union has an important economic and functional impact on the patient, by causing a persistent both physical but and psychological disability [8, 9].
Consequently, the study of the risk factors for femoral shaft non-union as well as the search for surgical strategies that could treat or prevent this serious complication is gaining a great interest in international literature.
Nail dynamization, i.e., the removal of interlocking screws either proximal or distal to the fracture site, is one of the proposed surgical options to manage femoral shaft non-union [10]. This simple procedure, generally performed under local anaesthesia, aims to obtain an increased bony compression at fracture site, thus improving osteogenesis and the transmission of weight-bearing forces [11, 12].
Several studies [5, 10,11,12,13,14,15,16] have investigated the efficacy of nail dynamization, but most of them have certain limitations, i.e., small sample size, concomitant evaluation of both femoral and tibial shaft fractures, different algorithms used for post-operative weight bearing, indications for dynamization, and timing of dynamization, thus making data interpretation challenging [10].
This study aims to assess the efficacy and the ideal timing for nail dynamization in patients with femoral shaft delayed union or non-union.
Materials and methods
Selection of study population: inclusion/exclusion criteria
The authors have retrospectively reviewed a series of 176 patients with femoral shaft fractures referring to our Department between January 2010 and December 2016. Clinical and radiological data were obtained from our trauma database. All the patients gave informed consent before enrolment.
Inclusion criteria were as follows: type 32 fracture according to Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association (AO/OTA) classification system; subsequent dynamization for delayed union or non-union; minimum clinical and radiological 12-month follow-up and surgical management with reamed intramedullary nailing.
Exclusion criteria were as follows: surgical management with open reduction and internal fixation; concomitant ipsilateral femoral neck fracture; periprosthetic fractures; exposed fractures; history of infections or malignant neoplasms; osteoporosis, defined as lumbar or hip T-score < − 2.5; immunosuppressive or steroid drug assumption; diabetes mellitus; BMI > 35 kg/m2.
By applying the inclusion and exclusion criteria, 68 patients (38 male and 30 female, mean age 36.85 years old, range 22–58) were recruited for the current study. The patients were then divided into three groups according to the fracture healing time:
-
Group A: fracture healing occurred within nine months
-
Group B: fracture healing occurred between nine and 12 months
-
Group C: fracture healing after 12 months or secondary procedure needed for union.
Surgical management and post-operative care
The average time from trauma to surgery was about 45 hours (range 20–69 hours). All the patients were treated by the same surgical team. The intramedullary nailing was always performed after the fracture reduction was obtained on a traction table; anterograde intramedullary reamed nails were used. The distal screws were implanted in both static and dynamic holes. The mean length of post-operative hospital stay was six days (range 5–13 days). Passive mobilization, i.e., static quadriceps exercises and passive mobilization of the knee with an electric motion device, started on post-operative day 1. The patients observed a non-weight-bearing until the callus formation, but they were encouraged, under the supervision of a physiotherapist, to actively mobilize the hip and the knee progressively. After the callus formation, partial weight bearing was authorized with a 10-weight increase a week for six weeks. Timing to dynamization was left to the discretion of the treating surgeon.
Radiographic study
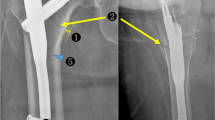
Two orthopaedic surgeons, with more than five years of experience in lower limb surgery, evaluated the anteroposterior (AP) and lateral (LL) femur X-rays performed at baseline and at follow-ups, in order to assess the correct intramedullary nail placement and the bone healing. At the time of dynamization, callus-to-diaphysis ratio, i.e., the ratio between the diameter of the fracture callus and the diameter of the normal diaphysis bone, was assessed in all the patients [10].
The fracture was considered healed when a bone callus could be depicted in at least three bone cortices out of four in AP and LL views [4].
Statistical analysis
Statistical analysis was performed using STATA/MP 14 for Windows (Stata Corp LP, College Station, USA). The Shapiro-Wilk test was conducted to verify the normal distribution of the data. One-way ANOVA (analysis of variance) was used to assess the differences between the three groups. Bonferroni multiple-comparison test was then executed to evaluate the differences between each group.
Pearson correlation test was performed to assess the association between the fracture union time, the timing for dynamization, and the callus-diaphysis index.
Logistic regression analysis was conducted to investigate the effects of the timing of dynamization and of the callus-to-diaphysis ratio on the fracture union. The tests were two-tailed with a confidence level of 5%.
Results
Sixty-eight patients (38 male and 30 female, mean age 36.85 years old, range 22–58) were recruited for the current study. In 30 patients out of 68 (44.12%), the fracture healing was observed at 9-month follow-up (group A); in 26 patients out of 68 (38.24%), the fracture healed within 12 months (group B); 8 fractures out of 68 healed in more than 12 months (11.76%, group C) and only four fractures out of 68 required a secondary procedure for union (7.35%, group C). Patients underwent nail dynamization, on average, at 6.7 months after fracture (range 3–10 months). Mean time to fracture union after the nail dynamization was 5.6 months. Dynamization was successful in 64 patients out of 68 (94.12%). Unhealed fractures were managed with nail exchanging after dynamization; bone grafting was used, in addiction, in one patient out of four. The main data of the study are summarized in Table 1.
Table 2 shows the Turkey-Kramer test results: the mean callus-diaphysis ratio was significantly different in group A (p = 0.001) and in group B (p = 0.03), compared with group C (Table 2). Moreover, the timing of dynamization resulted significantly different between the three groups (Table 2).
Pearson correlation test is shown in Table 3: a significant correlation between union time, timing of dynamization, and callus-diaphysis ratio was observed in group A (p = 0.031; p = 0.387) and group B (0.0123; 0.0115) (Table 3).
Linear regression analysis results are shown in Table 4. The impact of the timing of dynamization (X) on the fracture total union time (Y) is summarized by the following equation:
It could be noted that if the nail dynamization is performed between three and six months after trauma, the fracture heals within nine months after trauma.
The role of the callus-to-diaphysis ratio (Z) on the fracture total union time (Y) is described by the following equation:
This equation shows that the optimal callus-to-diaphysis ratio should be comprised between 1.47 and 1.19 at the time of dynamization, in order to obtain a fracture healing within nine months after trauma.
Discussion
Nail dynamization is a treatment option for delayed union or non-union of femoral midshaft fractures.
This procedure accelerates the bone healing, since the removal of interlocking screws results in an increased contact area and an enhanced compression forces at the fracture site, as well as in a better distribution of the weight-bearing forces [17]. These mechanical factors promote the osteogenesis at the fracture site, thus accelerating the fracture healing [18].
Compared with the alternative surgical procedures used in the management of femoral non-union or delayed union, i.e., nail exchanging, bone grafting, compression plating, and external fixation, dynamization is a faster, easier, and more economical surgical option [19].
In the past, nail dynamization was routinely performed to promote the fracture healing, while it is currently indicated mainly for delayed union or non-union [10, 13, 20]. This change could be bone healing the majority fractures [10, 13, 14]. Other studies have shown that nail dynamization, because of the locking screw removal, can cause bone shortening and loss of rotation stability at the fracture site, mainly in instable fracture patterns [8, 11, 14, 18, 20]. Moreover, fracture healing may be not achieved after nail dynamization, especially in long oblique, comminuted or spiroid fractures, thus requiring a secondary procedure for union [19].
Rupp et al. concluded in their work that for femoral and tibial diaphyseal shaft fractures, dynamization of the nail is an atraumatic, effective, and cheap surgical possibility to achieve bony consolidation, particularly in delayed non-unions before 24 weeks after initial surgery [21].
It is reported that the union rates of femoral fractures after nail dynamization range from 90 to 100% [10], while successful healing after femoral nail dynamization ranges from 19 to 82% [5, 10,11,12,13,14,15,16]. Several studies [5, 10,11,12,13,14,15,16] have investigated the efficacy of femoral nail dynamization, but most of them have certain limitations, which make data interpretation challenging [10].
The current study aims to assess the efficacy and the ideal time for dynamization in patients with femoral non-union or delayed union. This is, to the authors’ knowledge, the larger study conducted on femoral nail dynamization.
In this study, 68 patients, treated with femoral reamed endomedullary nail and subsequent dynamization for delayed union or non-union, were included. All the patients were then divided into three groups according to the fracture time healing: in group A patients with fractures which healed within nine months; in group B patients with fractures which healed between nine and 12 months; and in group C fractures which healed after 12 months or needed a secondary procedure for union.
The timing of dynamization resulted significant different in each group (Table 2); moreover, a significant correlation between the timing of dynamization and the fracture healing was observed in group A and group B (Table 3). Linear regression analysis revealed that when the nail dynamization is performed between three and six months, the fracture should heal within nine months after trauma. These data show that the timing of dynamization has a great impact on the fracture heling time, suggesting to perform it between three and six months after trauma. Indeed, a dynamization performed earlier than three months after trauma could be ineffective since it could disturb the plastic callus that is forming at the fracture site [9]. On the other hand, this study showed that when dynamization is performed after six months, the successful rate of this procedure lowers.
Callus-to-diaphysis ratio resulted significantly different in group C compared with group A and group B; a positive correlation between callus-to-diaphysis ratio and union time was found in group A and group B. Linear regression analysis revealed that the optimal callus-to-diaphysis ratio should be comprised between 1.47 and 1.19 at the time of dynamization, in order to obtain a fracture healing within nine months after trauma. These findings are consistent with the data observed by Vaughn et al., who reported that a callus-to-diaphysis ratio (CDR) greater than 1.17, at the timing of dynamization, had a 93% rate of union, whereas patients with a CDR less than 1.17 had a healing rate of only 20%. The current study confirms that the CDR is a useful tool to predict the outcome of a nail dynamization.
Dynamization in this study showed a high successful rate of 94.12%; this could be explained considering that patients with open fractures, osteoporotic fractures and history of infections were excluded from this study.
The non-standardized timing of nail dynamization, which was left to the discretion of the treating surgeon, is a limitation of this study. Our data should be further confirmed in a prospective randomized study, with a standard timing for nail dynamization.
Conclusion
In this study, femoral nail dynamization revealed safe and effective in the treatment of femoral delayed union and non-union, with a successful rate of 94.12%.
Moreover, in this study, a callus-to-diaphysis ratio between 1.47 and 1.19 at the time of dynamization revealed a predictive factor of fracture healing within 9 months after trauma. Consequently, CDR is an important tool that should be calculated at the time of dynamization, in order to predict the good outcome of this procedure.
On the basis of these data, nail dynamization should be considered as a first-line treatment for femoral non-union or delayed union. The ideal timing for an effective dynamization is between 3 and 6 months after injury.
References
Arneson TJ, Melton LJ, Lewallen DG, O’Fallon WM (1988) Epidemiology of diaphyseal and distal femoral fractures in Rochester, Minnesota, 1965-1984. Clin Orthop Relat Res:188–194
Salminen ST, Pihlajamäki HK, Avikainen VJ, Böstman OM (2000) Population based epidemiologic and morphologic study of femoral shaft fractures. Clin Orthop Relat Res:241–249
Vermesan D, Prejbeanu R, Haragus H et al (2017) Case series of patients with pathological dyaphiseal fractures from metastatic bone disease. Int Orthop 41:2199–2203. https://doi.org/10.1007/s00264-017-3582-3
Lee JR, Kim H-J, Lee K-B (2016) Effects of third fragment size and displacement on non-union of femoral shaft fractures after locking for intramedullary nailing. Orthop Traumatol Surg Res 102:175–181. https://doi.org/10.1016/j.otsr.2015.11.014
Pihlajamäki HK, Salminen ST, Böstman OM (2002) The treatment of nonunions following intramedullary nailing of femoral shaft fractures. J Orthop Trauma 16:394–402
Chen W, Jing Y, Lv H et al (2016) Displaced femoral shaft fractures treated by antegrade nailing with the assistance of an intramedullary reduction device. Int Orthop 40:1735–1739. https://doi.org/10.1007/s00264-015-3036-8
Somford MP, van den Bekerom MPJ, Kloen P (2013) Operative treatment for femoral shaft nonunions, a systematic review of the literature. Strategies Trauma Limb Reconstr 8:77–88. https://doi.org/10.1007/s11751-013-0168-5
Lynch JR, Taitsman LA, Barei DP, Nork SE (2008) Femoral nonunion: risk factors and treatment options. J Am Acad Orthop Surg 16:88–97
Koso RE, Terhoeve C, Steen RG, Zura R (2018) Healing, nonunion, and re-operation after internal fixation of diaphyseal and distal femoral fractures: a systematic review and meta-analysis. Int Orthop. https://doi.org/10.1007/s00264-018-3864-4
Vaughn J, Gotha H, Cohen E et al (2016) Nail dynamization for delayed union and nonunion in femur and tibia fractures. Orthopedics. https://doi.org/10.3928/01477447-20160819-01
Gelalis ID, Politis AN, Arnaoutoglou CM et al (2012) Diagnostic and treatment modalities in nonunions of the femoral shaft. A review. Injury 43:980–988. https://doi.org/10.1016/j.injury.2011.06.030
Huang K-C, Tong K-M, Lin Y-M et al (2012) Evaluation of methods and timing in nail dynamisation for treating delayed healing femoral shaft fractures. Injury 43:1747–1752. https://doi.org/10.1016/j.injury.2012.06.024
Tigani D, Fravisini M, Stagni C et al (2005) Interlocking nail for femoral shaft fractures: is dynamization always necessary? Int Orthop 29:101–104. https://doi.org/10.1007/s00264-004-0627-1
Wu CC (1997) The effect of dynamization on slowing the healing of femur shaft fractures after interlocking nailing. J Trauma 43:263–267
Wu CC, Shih CH (1993) Effect of dynamization of a static interlocking nail on fracture healing. Can J Surg 36:302–306
Wu C-C, Chen W-J (1997) Healing of 56 segmental femoral shaft fractures after locked nailing: poor results of dynamization. Acta Orthop Scand 68:537–540. https://doi.org/10.3109/17453679708999022
Johnson KD, Johnston DW, Parker B (1984) Comminuted femoral-shaft fractures: treatment by roller traction, cerclage wires and an intramedullary nail, or an interlocking intramedullary nail. J Bone Joint Surg Am 66:1222–1235
Akram Saji MA, Rabari YB, Kumar Gupta R et al (2017) Comparative study of static versus dynamic intramedullary nailing of tibia. Int J Orthop Sci 3:283–286. https://doi.org/10.22271/ortho.2017.v3.i3e.52
Yokota H, Tanaka SM (2005) Osteogenic potentials with joint-loading modality. J Bone Miner Metab 23:302–308. https://doi.org/10.1007/s00774-005-0603-x
Vécsei V, Häupl J (1989) The value of dynamic adjustment in locking intramedullary nailing. Aktuelle Traumatol 19:162–168
Rupp M, Biehl C, Budak M et al (2018) Diaphyseal long bone nonunions — types, aetiology, economics, and treatment recommendations. Int Orthop 42:247–258. https://doi.org/10.1007/s00264-017-3734-5
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study was conducted in accordance with the declaration of Helsinki. Informed consent was obtained from all participants.
Conflict of interest
The authors declare that there are no conflicts of interest.
Rights and permissions
About this article

Cite this article
Vicenti, G., Bizzoca, D., Carrozzo, M. et al. The ideal timing for nail dynamization in femoral shaft delayed union and non-union. International Orthopaedics (SICOT) 43, 217–222 (2019). https://doi.org/10.1007/s00264-018-4129-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-018-4129-y