
Abstract
Purpose
The conventional surgical treatment of moderate to severe hallux valgus (HV) deformity includes proximal metatarsal osteotomies (PMOs). Recent evidence suggests that the extension of indications for distal metatarsal osteotomies (DMOs) may result in comparable outcomes. The purpose of this study was to compare the efficacy of proximal with that of distal metatarsal osteotomies for moderate to severe HV deformity.
Methods
We searched PubMed, Scopus, and CENTRAL up to 25 July 2017. We included studies comparing the results of proximal and distal metatarsal osteotomies for moderate to severe HV deformity. The primary outcomes included the assessment of the first intermetatarsal angle (IMA) and American Orthopaedic Foot and Ankle Society (AOFAS) scoring system. For the secondary outcomes, we considered the hallux valgus angle, sesamoid position, and participants’ satisfaction. We also reported and analyzed complications. We evaluated all outcomes in the short-term (≤ 1 year) and medium-term (> 1 and < 10 years). The quality assessment was performed using the Cochrane risk of bias and ROBINS-I tools for randomized and non-randomized studies, respectively.
Results
Data from 696 cases were considered in this review. For the assessment of the first IMA, there was a slight advantage in favour of the PMO group in the medium term (SMD was − 0.38, 95% CIs − 0.65 to − 0.12, p < 0.05, I2 = 21%). For the rest outcomes, we did not detect any significant differences between the intervention groups.
Conclusions
For clinical and radiological outcomes, the quantitative synthesis demonstrated that there were no significant differences between PMO and DMO groups in the medium term. These findings were supported by data from non-randomized studies. For the reported complications, we did not detect any significant differences between the intervention groups.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hallux valgus (HV) is a progressive complex tri-planar deformity of the forefoot, which is characterized by a valgus deviation and occasionally pronation of the great toe, varus angulation of the first metatarsal, lateral displacement of the sesamoids and the extensor tendons, and a first metatarsophalangeal (MTP) joint bunion formation [1]. Although a wide variation in the prevalence of HV has been reported, there is a strong correlation of this deformity with female sex and advancing age [2,3,4,5]. Mann and Coughlin classified HV into three types based on hallux valgus angle (HVA) and intermetatarsal angle (IMA): mild (HV < 20°, IMA < 11°), moderate (HV 20–40°, IMA 11–16°), and severe (HV > 40°, IMA > 16°) [6].
Numerous surgical procedures have been described for correction of HV. The conventional treatment of severe deformity includes proximal metatarsal osteotomies (PMOs). On the other hand, distal metatarsal osteotomies (DMOs) are recommended for mild and moderate HV deformity [6, 7]. However, recent evidence indicates that the outcomes after distal metatarsal osteotomies for moderate to severe HV deformity appear to be satisfactory.
We hypothesized that the extension of indications for DMOs may result in comparable clinical and radiological outcomes with those of PMOs. The aim of this study was to compare the efficacy of proximal and distal metatarsal osteotomies for correction of moderate to severe HV deformity, through a random-effects meta-analysis study design.
Methods
The present meta-analysis was prospectively registered with PROSPERO (CRD42017068312). We also used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [8].
Inclusion and exclusion criteria
We enrolled studies that compared the results of proximal and distal metatarsal osteotomies in adults with moderate to severe hallux valgus deformity. This review included studies that compared any type of PMO with any type of DMO.
We excluded patients treated with scarf osteotomy as this is considered a mid-shaft rather a proximal or distal metatarsal osteotomy [9, 10]. We also did not consider studies assessing the efficacy of Lapidus procedure, since this is classified as an arthrodesis of the tarsometatarsal (TMT) joint [11].
Outcome assessment
The primary outcome measures were the American Orthopaedic Foot and Ankle Society (AOFAS) scoring system [12] and first IMA. The secondary outcomes were the HVA, tibial sesamoid position, participants’ satisfaction, and post-operative complications [13]. We assessed all the above outcomes in the following time periods: short term (≤ 1 year) and medium term (> 1 and < 10 years).
Literature search
We performed a literature search including the following electronic databases up to 25 July 2017: PubMed, Scopus, and Cochrane Central Register of Controlled Trials (CENTRAL). In these database searches, we applied no language restrictions. We also considered reference lists of relevant studies. Furthermore, we searched the following registries for completed unpublished comparative studies: ClinicalTrials.gov; Australian New Zealand Clinical Trials Registry (ANZCTR); and the International Standard Randomized Controlled Trial Number (ISRCTN) Register.
For the search strategy, we used the following terms: “hallux valgus,” “random*,” “comparative study,” “retrospective study,” “distal osteotomy,” “proximal osteotomy.” We adapted this search to each included database. In electronic supplementary material (ESM) 1, we provide the detailed search strategy we used for the PubMed.
Study selection
Two review authors (KT and DK) searched for records in a blinded fashion. Then, the titles and abstracts of these records were screened for eligibility. For the remaining articles, we obtained the full texts and assessed them for potential inclusion. We considered only RCTs in the meta-analysis.
Data extraction
Two reviewers (KT and DK) extracted the data independently. We abstracted information including the year of publication, comparators in the control group, and the number and demographics of patients in the included intervention groups. We also extracted information about the intervention characteristics, study outcomes, follow-up, and complications.
Quality assessment
Two investigators (KT and DK) independently performed the quality assessment of individual trials using the Cochrane Collaboration’s “risk of bias” and ROBINS-I tools for randomized and non-randomized studies, respectively [14, 15]. For the assessment of the included trials, we considered the following domains: randomization; allocation concealment; blinding of patients; blinding of personnel; blinding of outcome assessors; incomplete outcome data; selective reporting; and other bias. We judged each domain as either low, unclear, or high risk of bias.
Furthermore, we assessed the quality across studies. For each domain of the Cochrane’s risk of bias tool, if more than half of the information was from studies at a low risk of bias, we judged the domain to be at a low risk of bias. If most information was from studies at an unclear/high risk of bias, we considered the domain to be at an unclear/high risk of bias, respectively. For all study outcomes, we considered the domain of masking of outcome assessors to be crucial [16].
For the assessment of non-randomized trials, we considered three major domains:
-
1.
Pre-intervention
-
2.
At intervention
-
3.
Post-intervention
In the first domain, we assessed the risk of bias due to confounding and in the selection of patients for the study as well. In the second domain, we evaluated the risk of bias in classification of interventions. In the third domain, we assessed the risk of bias due to deviations from intended interventions and missing data. Furthermore, for the latter domain, we evaluated the risk of bias in the measurement of outcomes and selection of the reported results. The possible judgments were “low risk,” “moderate risk,” “serious risk,” and “critical risk” of bias. In this systematic review, the exploration for the presence of small study effects and publication bias depended on the number of the included studies (i.e., 10 as a minimum). This exploration is performed using funnel plots and statistical models [17, 18].
Finally, we contacted the corresponding authors of the included studies to request additional information in regard to the quality assessment. We resolved any discrepancies about the risk of bias assessment through discussion.
Statistical analysis
We used the Review Manager (RevMan) Software (version 5.3) to perform pair-wise meta-analysis [19]. For continuous outcomes, we conducted random effects quantitative synthesis utilizing the effect size of standardized mean difference (SMD) and calculated 95% confidence intervals (CIs) according to the inverse variance method. For dichotomous outcomes, we conducted a random effects meta-analysis using the Mantel-Haenszel method and considered the effect measure of odds ratio (OR).
In this review, a p value of less than 0.05 indicated statistical significance. We explored for statistical heterogeneity using the Q statistic and measured the extent of heterogeneity using the I2 statistic. We considered the following classification of statistical heterogeneity [20]:
-
I2 = 0–40%: not important heterogeneity
-
I2 = 30–60%: moderate heterogeneity
-
I2 = 50–90%: substantial heterogeneity
-
I2 = 75–100%: considerable heterogeneity
Synthesis of the results
For clinical and radiological outcomes, we avoided combining data from different study designs [21]. Instead, we provided a qualitative presentation of the results from non-randomized studies with the aim to supplement the results of our meta-analysis [21].
For the reported complications, we proceeded with a quantitative comparison between the intervention groups, after accounting for the randomization of the included studies. Briefly, we classified unintended events into complications involving bone and soft tissues. We thereafter conducted a post hoc meta-analysis, which was requested by the peer reviewers, using subgroup analyses for randomized and non-randomized studies.
Subgroup and sensitivity analyses
We accounted for the impact of the soft tissue release on the outcomes of the included operations by conducting a pre-specified subgroup analysis. Moreover, we performed a sensitivity analysis, in which we excluded trials at an unclear and high risk of bias. Finally, we conducted a post hoc sub-analysis, in which we kept only studies assessing patients with an IMA of > 16°.
Clinical interpretation of the results
For the classification of effect sizes in this meta-analysis, an SMD value of 0.2 showed a small effect, a value of 0.5 denoted a moderate effect, and a value of 0.8 indicated a large effect [22]. For the clinical interpretation of the results, we accounted for the level of evidence and statistical power of the analyses.
Results
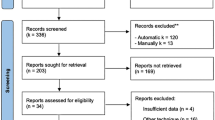
The literature search yielded 568 potentially relevant studies. Duplicates were removed and the remaining 431 studies were screened according to the information provided in their title and abstract. After the exclusion of 420 records, we assessed the remaining 11 articles for eligibility. In two articles, the patients did not present moderate to severe HV deformity [23, 24]. We enrolled 9 published studies in the qualitative synthesis [25,26,27,28,29,30,31,32,33]. Finally, we statistically pooled the results from 5 randomized trials (Fig. 1).

Flow diagram of the study selection procedure. HV= Hallux valgus
Study characteristics
In this systematic review, we considered nine comparative studies comprising a total of 696 feet. We abstracted information from 604 patients. Of the six randomized trials considered in the present review, five were eligible for inclusion in the quantitative synthesis [26, 28, 30, 32, 33]. The enrolled studies were published between 1991 and 2015. Four trials were conducted in Korea [29,30,31,32], one in the USA [25], one in Sweden [33], one in Turkey [26], one in China [27], and one in Thailand [28]. The mean age of participants in the intervention groups ranged between 31 and 65 years of age (Table 1).
In the proximal osteotomy group, we considered the following procedures: proximal crescentic, proximal chevron, Ludloff (30° proximal oblique diaphyseal), opening wedge, Mau (proximal oblique), and proximal closing wedge metatarsal osteotomies. On the other hand, in the distal metatarsal osteotomy group, we enrolled the following interventions: distal chevron, Bösch (subcapital linear), Hohmann, and Lindgren-Turan (30° subcapital transverse) osteotomies. For a thorough presentation of the intervention-related characteristics of the included studies, please see Table 2.
Quality assessment
For the RCTs, the results of the quality assessment of individual studies are shown in Table 3. Adequate randomization was performed in two trials of the present systematic review [28, 30]. For all the enrolled studies, there were no available registration protocols. We highlight that due to the different anatomical sites of the osteotomies, it was not possible for the participants to be blinded to the interventions they received. Successful blinding of the outcome assessors was reported in three trials [28, 30, 32]. For the risk of bias assessment across trials, most domains were at an unclear risk of bias (ESM 2). The findings from the quality assessment of non-randomized studies are presented in ESM 2. It should be noted that the number of the included studies did not allow us for creating funnel plots for the assessment of publication bias.
Synthesis of the results from randomized studies
Short-term assessment
Four studies were eligible for inclusion in the short-term outcome assessment of the present SR [28, 29, 31, 33]. Statistical pooling was possible for 185 feet. For the first IMA and HVA, there was a statistically significant difference in favour of the PMO group (SMD was − 0.71, 95% CIs − 1.02 to − 0.41, p < 0.05; and − 0.95, 95% CIs − 1.26 to − 0.64, p < 0.05, respectively) (ESM 3). In these analyses, heterogeneity was insignificant.
Medium-term assessment
For the assessment of the IMA, there was a statistically significant difference in favor of PMO group in the medium term (SMD = − 0.38, 95% CIs − 0.65 to − 0.12, p < 0.05) (Fig. 2). For this analysis, we detected low heterogeneity levels (I2 = 21%, p = 0.28).

Forest plot of standardized mean differences for the assessment of the first intermetatarsal angle in the medium term. Three different subgroups are considered. Vertical line demonstrates no difference between the two comparison groups. An overall statistically significant difference in favour of the proximal metatarsal osteotomy group is shown. SMD standardized mean difference, IV inverse variance, SD standard deviation, CI confidence interval, PMO proximal metatarsal osteotomy, DMO distal metatarsal osteotomy
Regarding the AOFAS evaluation in the medium term, there were no statistically significant differences between the intervention groups (SMD = 0.18, 95% CIs − 0.21 to 0.57, p = 0.16) (Fig. 3). In this analysis, statistical heterogeneity levels were considered to be moderate, albeit not significant (I2 = 46%, p = 0.16).

Forest plot of standardized mean differences for the assessment of the American Orthopaedic Foot and Ankle Society scoring system in the medium term. Two different subgroups are considered. Vertical line demonstrates no difference between the two comparison groups. In the overall analysis, no statistically significant differences are shown. SMD standardized mean difference, IV inverse variance, SD standard deviation, CI confidence interval, PMO proximal metatarsal osteotomy, DMO distal metatarsal osteotomy
For the assessment of the HVA, we did not detect any significant differences between the intervention groups (SMD = − 0.25, 95% CIs − 0.57 to 0.06, p = 0.12) (Fig. 4). Heterogeneity was not statistically significant (I2 = 43%, p = 0.15).

Forest plot of standardized mean differences for the assessment of the hallux valgus angle in the medium term. Three different subgroups are considered. Vertical line demonstrates no difference between the two comparison groups. In the overall analysis, no statistically significant differences are shown. SMD standardized mean difference, IV inverse variance, SD standard deviation, CI confidence interval, PMO proximal metatarsal osteotomy, DMO distal metatarsal osteotomy
For the assessment of the participants’ satisfaction, and tibial sesamoid position, we did not detect any significant differences between the intervention groups (Fig. 5 and ESM 4, respectively). Statistical heterogeneity was low in all cases.

Forest plot of odds ratios for the assessment of the participants’ satisfaction in the medium term. Two different subgroups are considered. No statistically significant differences are shown. M-H Mantel-Haenszel, CI confidence interval, PMO proximal metatarsal osteotomy, DMO distal metatarsal osteotomy
Results from non-randomized studies
A descriptive presentation of the main clinical and radiographic findings from non-randomized studies is provided in ESM 5. For these studies, we did not detect any significant clinical differences between the intervention groups. It should be noted that in one study, statistically significant differences in favour of the DMO group were reported regarding the first IMA and tibial sesamoid position changes [27].
Complications
For a qualitative presentation of the reported complications, please see ESM 6. For the complications involving bone and soft tissues, we did not detect any significant differences between the intervention groups (odds ratio was 1.37, 95% CI [0.62 to 3.06], p = 0.44, I2 = 32%; and 1.3, 95% CIs 0.4 to 4.24, p = 0.66, I2 = 41%, respectively) (ESM 7).
Sensitivity analyses
We conducted a pre-determined sensitivity analysis, in which we excluded trials at an unclear and high risk of bias and detected insignificant heterogeneity levels (ESM 8). Moreover, we did not detect any significant differences between our primary and sensitivity analyses when we accounted for the severity of the deformity (ESM 8).
Discussion
In this systematic review, we explored the efficacy of proximal and distal metatarsal osteotomies for the surgical management of moderate to severe HV deformity. Proximal metatarsal osteotomy offers a greater correction of the deformity and minimal shortening of the metatarsal, because the correction is performed near the first metatarsocuneiform joint. However, osteotomy at this site is relatively unstable and takes longer to heal than a DMO. Proximal metatarsal osteotomy is also likely to heal in dorsiflexion, which could cause transfer metatarsalgia [31]. On the other hand, DMO offers only relatively smaller amount of correction of the deformity, causing some post-operative shortening of the first metatarsal with a risk of avascular necrosis of the metatarsal head. However, DMO requires a shorter incision and improves pain and functional ability in a wider range of deformities [28]. Recent studies have shown that the extension of indications of distal metatarsal osteotomies may be a viable option. In the present systematic review, we used information from 696 feet with the aim to clarify this controversy. For patient-reported and clinician-oriented outcomes, the quantitative synthesis showed that there were no significant differences between the intervention groups in the medium term. These findings were supported by data from non-randomized studies and remained robust after controlling for the severity of the deformity.
Dealing with clinical diversity
We highlight that the scope of a systematic review determines the extent to which the included studies are diverse [20]. In the present study, we performed a comparison linked to the anatomical location of the metatarsal osteotomies using a pair-wise meta-analysis study design. Taking into account that the optimal proximal and distal metatarsal osteotomies for moderate to severe hallux valgus deformity have yet to be defined, we considered that a meta-analysis study design was appropriate to test our hypothesis. After analyzing data, we observed insignificant heterogeneity indicating that the intervention effects were not significantly affected by factors that varied across studies [20].
Medium-term clinical and radiographic findings
For the assessment of the first IMA, we detected a slight superiority in favor of the PMO group. Among the PMOs and DMOs, evidence from randomized and non-randomized studies showed that none was favoured in terms of the patients’ satisfaction and AOFAS assessment. These findings remained robust after adjusting for the risk of bias. Finally, we highlight that we detected higher complication rates in the PMO group.
Clinical implications
For the management of HV deformity, PMOs are considered to be more technically demanding and require a more restricted post-intervention protocol compared to DMOs [9, 34]. As we did not detect any significant differences between the therapeutic efficacy of proximal and distal metatarsal osteotomies, this study suggests that the decision between these two interventions depends on a surgeon’s skills and/or preference. We also highlight that health policy makers should take into account the higher number of reported complications after proximal metatarsal osteotomies and cost-effectiveness of different techniques for bunion surgery [35].
Strengths and limitations of the present systematic review
In this SR, the sample size was adequate enough to allow us for testing our hypothesis. However, half of the included studies were judged to be at an unclear risk of bias. Thus, we suggest that the results of the present systematic review be interpreted with caution. It should be noted that in 89 cases of the present systematic review, a simultaneous bilateral correction was performed. We also noticed a variability in the definition of moderate and severe hallux valgus deformity among the included studies. Finally, we detected that there was a limited reporting of long-term results in the enrolled studies (i.e., at 10 years and beyond).
Implications for future research
For a thorough pre-operative assessment, we recommend that the authors of the future studies should not only focus on the pre-operative HVA and IMA measurements, but also interphalangeal angle, first metatarsal protrusion distance, and sesamoid rotation angle [36, 37]. Moreover, we suggest that more emphasis is placed on the reporting of long-term observations.
Conclusions
In conclusion, for the management of moderate to severe HV deformity, we found no significant clinical and radiographic differences between patients treated with proximal and distal metatarsal osteotomies. This was also the case for the reported complications. Accordingly, we underline that the extension of the indications for distal metatarsal osteotomies may be a viable option. Between proximal and distal metatarsal osteotomies, we recommend that an orthopedic surgeon decide not only on the basis of his/her personal skills and/or preference but also on the cost-effectiveness of the available techniques.
References
Badekas A, Georgiannos D, Lampridis V, Bisbinas I (2013) Proximal opening wedge metatarsal osteotomy for correction of moderate to severe hallux valgus deformity using a locking plate. Int Orthop 37:1765–1770. https://doi.org/10.1007/s00264-013-2019-x
Cho NH, Kim S, Kwon DJ, Kim HA (2009) The prevalence of hallux valgus and its association with foot pain and function in a rural Korean community. J Bone Joint Surg Br 91(4):494–498. https://doi.org/10.1302/0301-620X.91B4.21925
Nguyen US, Hillstrom HJ, Li W, Dufour AB, Kiel DP, Procter-Gray E, Gagnon MM, Hannan MT (2010) Factors associated with hallux valgus in a population-based study of older women and men: the MOBILIZE Boston Study. Osteoarthr Cartil 18(1):41–46. https://doi.org/10.1016/j.joca.2009.07.008
Nix S, Smith M, Vicenzino B (2010) Prevalence of hallux valgus in the general population: a systematic review and meta-analysis. J Foot Ankle Res 3:21. https://doi.org/10.1186/1757-1146-3-21.
Roddy E, Zhang W, Doherty M (2008) Prevalence and associations of hallux valgus in a primary care population. Arthritis Rheum 59(6):857–862. https://doi.org/10.1002/art.23709.
Coughlin MJ, Saltzman CL, Anderson RB. Mann’s surgery of the foot and ankle. 9th Edition.
Easley ME, Trnka HJ (2007) Current concepts review: hallux valgus part II: operative treatment. Foot Ankle Int 28(6):748–758
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Annals of Internal Medicine 151:W65eW94
Easley ME, Darwish HH, Schreyack DW, DeOrio JK, Trnka HJ (2012) Hallux valgus: proximal first metatarsal osteotomies. In: Saxena A (ed) International advances in foot and ankle surgery. Springer, London
Wülker N, Mittag F (2012) The treatment of hallux valgus. Dtsch Arztebl Int 109(49):857–867; quiz 868. https://doi.org/10.3238/arztebl.2012.0857
Lapidus PW (1960) The author’s bunion operation from 1931 to 1959. Clin Orthop 16:119–135
Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M (1994) Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int 15(7):349–353
Sammarco GJ, Idusuyi OB (2001) Complications after surgery of the hallux. Clin Orthop Relat Res 391:59–71
Higgins JPT, Altman DG (2008) Chapter 8: assessing risk of bias in included studies. In: Higgins JPT, Green S (eds) Cochrane handbook for systematic reviews of interventions. John Wiley & Sons, Chichester
Sterne JAC, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, Henry D, Altman DG, Ansari MT, Boutron I, Carpenter JR, Chan AW, Churchill R, Deeks JJ, Hróbjartsson A, Kirkham J, Jüni P, Loke YK, Pigott TD, Ramsay CR, Regidor D, Rothstein HR, Sandhu L, Santaguida PL, Schünemann HJ, Shea B, Shrier I, Tugwell P, Turner L, Valentine JC, Waddington H, Waters E, Wells GA, Whiting PF, Higgins JP (2016) ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355:i4919. https://doi.org/10.1136/bmj.i4919
Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ (1996) Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 17(1):1–12
Egger M, Smith GD, Scheider M, Minder C (1997) Bias in meta analysis detected by a simple graphical test. BMJ 315:629e34
Mavridis D, Salanti G (2014) Exploring and accounting for publication bias in mental health: a brief overview of methods. Evidence Based Mental Health 17:11e5. https://doi.org/10.1136/eb-2013-101700
The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). 5.1. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011. http://www.cc-ims.net/revman/download.
Deeks JJ, Higgins JPT, Altman DG (2008) Chapter 9: analysing data and undertaking meta-analyses. In: Higgins JPT, Green S (eds) Cochrane handbook for systematic reviews of interventions. John Wiley & Sons, Chichester
Reeves BC, Deeks JJ, Higgins JPT, Wells GA (2008) Chapter 13: including non-randomized studies. In: Higgins JPT, Green S (eds) Cochrane handbook for systematic reviews of interventions. John Wiley & Sons, Chichester
Cohen J (1988) Statistical power analysis for the behavioral sciences. 2nd Edition. Hillsdale, NJ, USA: Lawrence Erlbaum Associates.
Jahss MH, Troy AI, Kummer F (1985) Roentgenographic and mathematical analysis of first metatarsal osteotomies for metatarsus primus varus: a comparative study. Foot Ankle 5(6):280–321
Williams L, Wilson S, Kuwada GT (1995) A comprehensive retrospective analysis of complications and radiographic findings following bunionectomy procedures for first ray deformities. Lower Extremity 2(1):11–28
Bar-David T, Trepal MJ (1991) A retrospective analysis of distal Chevron and Basilar osteotomies of the first metatarsal for correction of intermetatarsal angles in the range of 13 to 16 degrees. J Foot Surg 30(5):450–456
Bostan B, Güneş T, Erdem M, Aşcı M, Şen C, Erdogan H (2008) Comparison of modified Lindgren-Turan operation and proximal crescentic osteotomy combined with distal soft tissue procedure in the treatment of hallux valgus. Joint Dis Rel Surg 19(2):61–65
Chiang CC, Lin CF, Tzeng YH, Huang CK, Chen WM, Liu CL (2012) Distal linear osteotomy compared to oblique diaphyseal osteotomy in moderate to severe hallux valgus. Foot Ankle Int 33(6):479–486
Chuckpaiwong B (2012) Comparing proximal and distal metatarsal osteotomy for moderate to severe hallux valgus. Int Orthop 36(11):2275–2278. https://doi.org/10.1007/s00264-012-1656-9
Lee JY, Lee YS, Song KC, Choi KY (2015) Change in first metatarsal length after proximal and distal Chevron osteotomies for hallux valgus deformity. J Foot Ankle Surg 54(4):525–530. https://doi.org/10.1053/j.jfas.2014.07.004
Lee KB, Cho NY, Park HW, Seon JK, Lee SH (2015) A comparison of proximal and distal Chevron osteotomy, both with lateral soft-tissue release, for moderate to severe hallux valgus in patients undergoing simultaneous bilateral correction: a prospective randomised controlled trial. Bone Joint J 97-B(2):202–207. https://doi.org/10.1302/0301-620X.97B2.34449
Park CH, Jang JH, Lee SH, Lee WC (2013) A comparison of proximal and distal chevron osteotomy for the correction of moderate hallux valgus deformity. Bone Joint J 95-B(5):649–656. https://doi.org/10.1302/0301-620X.95B5.30181
Park HW, Lee KB, Chung JY, Kim MS (2013) Comparison of outcomes between proximal and distal chevron osteotomy, both with supplementary lateral soft-tissue release, for severe hallux valgus deformity: a prospective randomised controlled trial. Bone Joint J 95-B(4):510–516. https://doi.org/10.1302/0301-620X.95B4.30464
Resch S, Stenström A (1993) Results after chevron osteotomy and proximal osteotomy for hallux valgus: a prospective, randomized study. Foot 3(3):99–104
Cassinelli SJ, Herman R, Harris TG (2016) Distal metatarsal osteotomy for moderate to severe hallux valgus. Foot Ankle Int 37(10):1137–1145
Wagner E, Ortiz C, Torres K, Contesse I, Vela O, Zanolli D (2016) Cost effectiveness of different techniques in hallux valgus surgery. Foot and Ankle Surgery 22(4):259–264. https://doi.org/10.1016/j.fas.2015.11.004
Dixon AE, Lee LC, Charlton TP, Thordarson DB (2015) Increased incidence and severity of postoperative radiographic hallux valgus interphalangeus with surgical correction of hallux valgus. Foot Ankle Int 36(8):961–968. https://doi.org/10.1177/1071100715579905
Lee KM, Ahn S, Chung CY, Sung KH, Park MS (2012) Reliability and relationship of radiographic measurements in hallux valgus. Clin Orthop Relat Res 470(9):2613–2621. https://doi.org/10.1007/s11999-012-2368-6
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Tsikopoulos, K., Papaioannou, P., Kitridis, D. et al. Proximal versus distal metatarsal osteotomies for moderate to severe hallux valgus deformity: a systematic review and meta-analysis of clinical and radiological outcomes. International Orthopaedics (SICOT) 42, 1853–1863 (2018). https://doi.org/10.1007/s00264-018-3782-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-018-3782-5