
Abstract
Purpose
Although the most complex management of Gartland type IV supracondylar humeral fracture (SCHF) due to instability, the gold standard of initial treatment remains closed reduction and percutaneous pinning. However, open reduction was inevitable in most published studies. This study reports the outcome of treatment by leverage-assisted closed reduction.
Method
Twenty-seven patients were diagnosed as Gartland type IV SCHF during surgery in 214 preoperative Gartland type III fractures. Leverage-assisted reduction with percutaneous lateral pinning was done in these patients after failure of close reduction. Evaluations were performed with radiographic examination, clinical assessment and Flynn’s criteria by interview and physical examination.
Result
All 27 patients obtained acceptable reduction by leverage-assisted close reduction and percutaneous pinning. The average follow-up was 23.6 (18–30 months). There was no neurovascular complication, infection, nonunion, myositis ossificans or Volkmann’s contracture. Evaluation of Baumann’s angle was towards varus (74–74.2°). There was no significant difference (p = 0.1876). Flynn’s criteria were excellent in 22 (81.5 %) patients, good in four (14.8 %) and fair in one (3.7 %). The rate of excellent and good outcome was 96.3 % and of satisfactory 100 %.
Conclusion
We recommend leverage-assisted closed reduction as an option before open reduction in type IV SCHF, not only for gold standard management but also because of satisfactory outcomes and the low incidence of major complications.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
A supracondylar humeral fracture (SCHF) is the one of the most common fractures in children, accounting for 18 % of all paediatric fracture types [1], and is often associated with the development of serious complications [2]. SCHF are classified into two types: extension (98 %) and flexion (2 %) [3]. In extension fractures, Gartland classification is used to describe injury severity and to focus therapeutic management [4]. There were three classic types (I, II, III), which are now divided into four types according to the degree of fracture displacement measured in the lateral view on a plain radiographs [4, 5]. Type I fracture is nondisplaced (subtype Ia) or minimally displaced (<2 mm) (subtype Ib) and is associated with an intact anterior humeral line. Type II fracture presents with slight displacement (>2 mm), with a posterior angulation of the distal fragment and the posterior cortex remaining intact (subtype IIa) or when the fracture presents a straight or rotatory displacement with contact between the two fragments (subtype IIb). Type III fracture has a posteromedial (IIIa) or posterolateral (IIIb) displacement associated with loss posterior cortex integrity, resulting in extension of the distal fragment on the sagittal plane and rotation in the transverse plane. Type IV fracture has multidirectional instability characterised by complete circumferential tear of the periosteum and instability in flexion and extension [4, 6]. This type of SCHF is not often diagnosed by imaging studies but during manoeuvres in the operating room to reduce the fracture.
The current concepts of management popularly are that type I fractures are managed nonsurgically, but most displaced injuries (type II, III and IV) require surgical intervention [4]. Displaced SCHF have always presented a management challenge [7], and the gold standard technique is closed reduction and percutaneous pinning [8].
Although type IV fractures require the most complex management due to instability, initial management must be the same as for types II and III, i.e. closed reduction and pinning with K wires [6]. However, in most published studies, open reduction was common in previous reduction failures using closed methods [9]. To our knowledge, leveraged management of type IV SCHF in children has not been studied. The purpose of this study was, therefore, to determine the utility of leverage assistance and percutaneous pinning to treat type IV SCHF in children.
Materials and method
Our Institutional Ethics Committee approved the protocol for this study. From July 2013 to July 2014, 214 patients with Gartland type III SCHF were managed at our hospital; 12.6 % patients (27/214) with type IV SCHF were diagnosed during surgery and treated with leverage assistance and percutaneous lateral K-wire pinning. All patients were without neurovascular symptoms before operation. There were 16 (59.3 %) boys and 11 (40.7 %) girls. The average age was 5.2 (2–11) years, and the mean presentation from injury was 5.4 hours (1–16 hours). Left elbow injury occurred in 15 patients and the right elbow in 12. The most common mode of trauma was fall while playing (n = 22, 81.5 %), fall from a rolling scooter (n = 4, 14.8 %) and a fall from three months (n = 1, 3.7 %). All patients were operated upon at 14.6 hours after admission (6–20 hours). All patients primarily accepted close reduction (detail as previously) and leverage assistance if closed reduction failed. Patients were discharged 48 hours post-operatively, and the first follow-up was after one week.
Surgical technique
Patients were treated under general anesthesia in the supine position. After preparation and draping, longitudinal traction was applied under general anesthesia, with an assistant applying countertraction on C-arm fluoroscopy with the elbow in extension and forearm in supination. Leveraged assistance reduction was applied immediately after reduction failed using closed reduction during the entire procedure, and type IV SCHF was addressed. On C-arm fluoroscopy lateral views, the tip for leverage was located at the mid-diaphyseal humerus of a posterior fracture, skin incision was performed by the sharp tip of the leverage, and a blunt tip was used to enter (normal leverage diameter 2.5–3.5 mm based on patient age). Leverage with a blunt tip crossed the soft tissue to the cortex of the fracture fragment (Figs. 1 and 2). A very important point is that the radial pulse is checked during every step.

Leverage-assisted reduction: Leverage with blunt tip crosses the soft tissue of the posterior proximal cortex of the humerus after skin incision using the sharp tip of leverage instrument in extension type (a1) or distal humerus in flexion type (b1) fractures. Top of distal fracture used as the pivot (red point) in extension type (a2) or bottom of a proximal fracture used as the first pivot (dashed red point) in flexion type (b2) fractures. Pulling down on the leverage device to assist reduction on the pivot point in extension type (a3) or lifting up on the second pivot (red point) in flexion type (b3) fractures

Adjustment of radial or ulnar deviation using leverage to correct the deviation on the radius or ulnar side: Fracture lifted to create a little space between the two fragments then gently moved laterally (for ulnar deviation) (b) or medially (for radial deviation) on the pivot until acceptable reduction is achieved (c)
Reduction was checked by fluoroscopy. The assistant kept the proximal part of the arm and leveraged bone in a stable position, and three K wires of 1.6 mm were passed from the lateral epicondyle through a stab wound. Final reduction and pin placement was checked by anteroposterior (AP) and lateral X-rays. Pins were cut off over the skin, and pin tails were wrapped. An above-elbow plaster slab in 80º of flexion was applied with the forearm in its natural position.
Postoperative and functional assessment
Follow-up included regular clinical examination and AP and lateral X-rays at one, four, six and nine weeks and an average of 23.6 months (18–30 months) after operation. The cast and pins were removed at four weeks’ follow-up in the outpatient department. Patients subsequently started recovery of elbow motion on their own. No patient underwent physical therapy. Clinical examination included neurovascular function, range of motion (ROM) of both elbows, measurement of carrying angle and determination of infections. ROM and carrying angle of the both elbows were measured by a manual full-circle goniometer. Baumann’s angle was calculated during surgery and at final follow-up; carrying angle of the injured and normal sides was measured at the final follow-up. Flynn’s criteria are used to assess functional and cosmetic outcomes at the final follow-up. Comparison was based on the function component of the injured elbow compared with the contralateral elbow. Flexion, extension and cosmetic differences in terms of carrying angle were also compared. The lesser of the two results was considered as the final result.
Statistical analysis
Student’s t test was used to compare continuous data of Baumann angle in normal distribution. Statistical analysis was performed with SPSS software (version 14.0; Chicago, IL, USA). To determine statistical significance of Baumann’s angle right after operation and at final follow-up, we used a p value <0.05.
Results
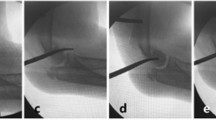
Twelve patients (12.6 %, 27/214) were diagnosis as having type IV SCHF during surgery for pre-operative Gartland type III SCHF. All type IV SCHF were treated with leverage assistance to recover the ligament and acquire successful reduction (Fig. 3). All fractures healed within four to six weeks; there were no neurovascular complication, infection, nonunion, myositis ossificans or Volkmann’s contracture.

Radiographic images during the procedure: Pre-operative type III supracondylar humeral fracture (SCHF) was diagnosed as type IV with multidirectional instability (a and b). Reduction lever was inserted into the fracture to assist reduction (c and d). Kirschner wires were inserted from the lateral condyle for fracture fixation (e and f). Final reduction and pin placement was checked by anteroposterior and lateral view X-ray (g and h)
Baumann’s angles measured immediately after surgery and at final follow-up were not significantly different (p = 0.1876). Mean final follow-up Baumann’s angle was 74.2° ± 2.7°, and mean post-operative Baumann’s angle was 74° ± 2.5°. Carrying angle of the injured and normal sides was measured at the final follow-up: 22 (81.5 %) patients had 0–5° loss of carrying angle, four (14.8 %) had 5–10° loss and one (3.7 %) had 10–15° loss; 21 (77.8 %) lost <5° ROM in the injured elbow, five (18.5 %) lost 5–10° and one (3.7 %) lost 10–15°. There were 22 excellent, four good and one fair result according to Flynn’s criteria; the rate of excellent and good outcome was 96.3 % and of satisfactory was 100 % (Table 1).
Discussion
SCHF is the most common elbow fracture in children and occurs mostly between the ages of six and nine years [10]. When treating the supracondylar fracture, the main target is to gain functional anatomic reduction with no serious complications [11]. Type IV SCHF was mostly diagnosed during surgery and caused by iatrogenic manoeuvres [4], and the reported incidence of type IV SCHF is rare. In our study, 12.62 % of preoperative Gartland type III SCHF were changed to type IV SCHF during operation. According to the Gartland Classification, the treatment of type III or IV SCHF can be achieved through an anatomical reduction, ideally in a single intervention, which can be obtained using several methods, such as closed reduction and casting, closed reduction and percutaneous pinning, traction, and open reduction with internal fixation [12]. Although type IV SCHF requires the most complex management due to instability, initial management must be closed reduction and pinning with K wires [6]. However, it is one of the most difficult fractures to manage because of marked swelling, difficulty in reduction and maintaining the reduction until healing takes place. As reported, closed reduction of displaced pediatric supracondylar fractures fails in up to 25 % of patients and requires remanipulation because of inadequate reduction or malpositioning of wires in 1–7 % of patients [13]. This means that a certain portion of the displaced fractures cannot be reduced with the closed method, with the conversion rate to open reduction being between 3 and 46 % [14].
In this context, we treated 27 patients with type IV SCHF using leverage assistance and percutaneous pinning from the lateral side of the elbow after failure of closed reduction instead of open reduction. According to Flynn’s criteria, results showed that 77.8 % of patients had excellent outcomes and 18.5 % had good outcomes. Baumann’s angles were not significantly different during surgery or at final follow-up. All patients had satisfactory functional and cosmetic results after an average of 23.6 months’ follow-up. It is generally accepted that three to four weeks of immobilisation provides adequate clinical and radiographic healing and that the pin be removed at that point. Pin removal in our cases was four weeks. However, it is worth noting that while some surgeons initially adopt the open approach as the treatment modality, especially for type III fractures, the majority of surgeons believe it should be applied only if closed reduction fails [4, 6]. We recommended leverage assistance with closed reduction as one option before using open reduction.
The elbow is a very complex anatomical area, where many structures are related and must be well understood by the paediatric orthopaedic surgeon for proper supracondylar fracture management [4]. A 1 % complication rate has been reported following SCHF treatment [15]. Associated vascular complications are common with supracondylar fractures because of the vulnerable position of the neurovascular structures in relation to fracture fragments and possible haemorrhage [16]. In our procedure, anterior anatomic structures and vasculature were never relatively at risk of injury. A blunt leverage tip was use during the whole procedure after the skin was incised by a sharp tip. Sawaizumi et al. noted that there was no interposition of soft tissue in the fracture area when manual reduction was impossible, and the procedure was changed to open reduction [17]. We considered that when the blunt tip carefully followed the humeral cortex anteriorly and posteriorly, the neurovascular system remained relatively safe.
Open reduction led to concerns regarding elbow stiffness, myositis ossificans, unsightly scarring and iatrogenic neurovascular injury [18]. Overall, the incidence rates of iatrogenic ulnar nerve injury ranged from 0 to 6 % [19], and lateral pinning was recommended when suitable [4]. In this study, we used lateral pinning and had no iatrogenic nerve injury. Pirone et al. suggested an increased risk of infection after open reduction [20]. In our study, the incision of 2.5–3.5 mm created using the leverage pin healed naturally without suture. There was incision or pin-tract infection or myositis ossificans. With regards to our method of treatment, leverage-assisted reduction achieved a successful outcome with a low incidence of major complications.
Sawaizumi el al. were the first to report the leverage technique on displaced SCHF. Reduction using their technique was impossible in four elbows in relatively older male children (aged 13–15) [17]. They considered that a good indication for this technique is children aged 12 years of age or younger. This finding suited our study well, as enrolled patients were two to 11 years old; all achieved acceptable reduction with leverage assistance. Lee et al. evaluated the use of pin leverage in the reduction of Gartland type III SCHF in children and compared them with closed and open reductions [21]. They concluded that pin leverage gives good results in Gartland type III fractures.
To our knowledge, our study the first to report the application of leverage-assisted reduction in type IV supracondylar fracture treatment in children. However, the study is not without limitations. Due to the uncommon occurrence of type IV SCHF, the sample size was limited. Although the follow-up was >two years in most cases, they were shorter in some cases. Due to the mini-invasive procedure, there is risk of infection compared with closed reduction. There is also a considerable learning curve for surgeons when using this procedure; for instance, choosing a small incision point, force necessary to apply during leverage, etc. However, it is a reliable and safe way to reduce the unstable fracture if performed carefully and gently enough.
Conclusion
High rates of satisfactory results were found in the treatment of type IV SCHF using leverage-assisted reduction. We recommend starting with a closed-reduction technique for type IV SCHF; if an anatomical reduction cannot be obtained after closed attempts, leverage-assisted reduction is one option before open reduction. We obtained adequate anatomical reduction using leverage-assisted reduction, with excellent to good functional and cosmetic outcomes and few complications.
References
Kim TJ, Sponseller PD (2014) Pediatric supracondylar humerus fractures. J Hand Surg [Am] 39:2308–2311. doi:10.1016/j.jhsa.2014.07.005
Young S, Fevang JM, Gullaksen G, Nilsen PT, Engesater LB (2012) Parent and patient satisfaction after treatment for supracondylar humerus fractures in 139 children: no difference between skeletal traction and crossed pin fixation at long-term followup. Adv Orthop 2012:958487. doi:10.1155/2012/958487
Omid R, Choi PD, Skaggs DL (2008) Supracondylar humeral fractures in children. J Bone Joint Surg Am 90(5):1121–1132. doi:10.2106/JBJS.G.01354
Zorrilla de Neira JS, Prada-canizares A, Marti-Ciruelos R, Pretell-Mazzini J (2015) Supracondylar humeral fractures in children: current concepts for management and prognosis. Int Orthop (SICOT) 39(11):2287–2296. doi:10.1007/s00264-015-2975-4
Madjar-Simic I, Talic-Tanovic A, Hadziahmetovic Z, Sarac-Hadzihalilovic A (2012) Radiographic assessment in the treatment of supracondylar humerus fractures in children. Acta Inform Med 20(3):154–159. doi:10.5455/aim.2012.20.154-159
Leitch KK, Kay RM, Femino JD, Tolo VT, Storer SK, Skaggs DL (2006) Treatment of multidirectionally unstable supracondylar humeral fractures in children. A modified Gartland type IV fracture. J Bone Joint Surg Am 88(5):980–985
Bhuyan BK (2012) Close reduction and percutaneous pinning in displaced supracondylar humerus fractures in children. J Clin Orthop Trauma 3(2):89–93. doi:10.1016/j.jcot.2012.09.004
Randsborg PH (2013) Fracture in children: aspects on health service, epidemiology and risk facors. Acta Orthop Suppl 350(84):1–24. doi:10.3109/17453674.2013.789731
Novais EN, Andrade MA, Gomes DC (2013) The use of a joystick technique facilitates closed reduction and percutaneous fixation of multidirectionally unstable supracondylar humeral fractures in children. J Pediatr Orthop 33(1):14–19. doi:10.1097/BPO.0b013e3182724d07
Abzug JM, Herman MJ (2012) Management of supracondylar humerus fractures in children: current concepts. J Am Acad Orthop Surg 20(2):69–77. doi:10.5435/JAAOS-20-02-069
Pretell Mazzini J, Rodriguez Martin J, Andres Esteban EM (2010) Surgical approaches for open reduction and pinning in severely displaced supracondylar humerus fractures in children: a systematic review. J Child Orthop 4(2):143–152. doi:10.1007/s11832-010-0242-1
Sadiq MZ, Syed T, Travlos J (2007) Management of grade III supracondylar fracture of the humerus by straight-arm lateral traction. Int Orthop 31(2):155–158
Pretell-Mazzini J, Rodriguez-Martin J, Andres-Esteban EM (2010) Does open reduction and pinning affect outcome in severely displaced supracondylar humeral fractures in children? A systematic review. Strateg Trauma Limb Reconstr 5(2):57–64. doi:10.1007/s11751-010-0091-y
Oh CW, Park BC, Kim PT, Park IH, Kyung HS, Ihn JC (2003) Completely displaced supracondylar humerus fractures in children: results of open reduction versus closed reduction. J Orthop Sci 8(2):137–141
Vallial N, Sommarhem A, Paavola M, Nietosvaara Y (2015) Pediatric distal humeral fractures and complications of treatment in Finland: a review of compensation claims from 1900 through 2010. J Bone Surg Am 97(6):494–499. doi:10.2106/JBJS.N.00758
Krusche-Mandl I, Aldrian S, Kottstorfer J, Seis A, Thalhammer G, Egkher A (2012) Crossed pinning in paediatric supracondylar humerus fractures: a retrospective cohort analysis. Int Orthop 36(9):1893–1898. doi:10.1007/s00264-012-1582-x
Sawaizumi T, Takayama A, Ito H (2003) Surgical technique for supracondylar fracture of the humerus with percutaneous leverage pinning. J Shoulder Elb Surg 12(6):603–606
Fu D, Xiao B, Yang S, Li J (2011) Open reduction and bioabsorbable pin fixation for late presenting irreducible supracondylar humeral fracture in children. Int Orthop 35(5):725–730. doi:10.1007/s00264-010-1018-4
Slobogean BL, Jackman H, Tennant S, Slobogean GP, Mulpuri K (2010) Iatrogenic ulnar nerve injury after the surgical treatment of displaced supracondylar fractures of the humerus: number needed to harm, a systematic review. J Pediatr Orthop 30(5):430–436. doi:10.1097/BPO.0b013e3181e00c0d
EI-Adl WA, EI-Said MA, Boghdady GW, Ali AS (2008) Results of treatment of displaced supracondylar humeral fractures in children by percutaneous lateral crossing wiring technique. Strateg Trauma Limb Reconstr 3(1):1–7. doi:10.1007/s11751-008-0030-3
Lee HY, Kim SJ (2007) Treatment of displaced supracondylar fractures of the humerus in children by a pin leverage technique. J Bone Joint Surg (Br) 89(5):646–650
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no competing interests exist.
Rights and permissions
About this article

Cite this article
Pei, X., Mo, Y. & Huang, P. Leverage application on Gartland type IV supracondylar humeral fracture in children. International Orthopaedics (SICOT) 40, 2417–2422 (2016). https://doi.org/10.1007/s00264-016-3206-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-016-3206-3