
Abstract
Renal fusion anomalies are common congenital anomalies of the urogenital tract and have their genesis in the early embryonic period. They are classified into partial fusion anomalies (e.g., crossed fused ectopia, and horseshoe kidney) and complete fusion anomalies (e.g., fused pelvic kidney). Horseshoe kidney is the most common renal fusion anomaly and is characterized by the presence of two distinct functioning kidneys on either side of the vertebral column, with fusion occurring at the inferior poles in majority of the cases. Crossed fused ectopia is characterized by the presence of an ectopic kidney that crosses the midline and fuses with the orthotopic contralateral kidney, whereas fused pelvic (pancake) kidney is a complete fusion anomaly characterized by extensive medial fusion of both kidneys in the pelvis. Fusion anomalies are often associated with abnormalities of renal rotation, migration, and vascular supply, which predispose the kidneys to a number of complications and create difficulty during retroperitoneal surgeries and interventions. They are also associated with other congenital abnormalities of the urogenital tract, gastrointestinal tract, cardiovascular system, and skeletal system. Hence, a thorough understanding of the etiopathogenesis and radiological features of fusion anomalies is important for directing patient management. This review summarizes the embryological basis, clinical presentation and imaging approach to renal fusion anomalies, followed by detailed anatomical and radiological description of the morphological types, and the complications associated with these anomalies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Renal fusion anomalies are among the common congenital anomalies of the urogenital tract. They are classified into partial fusion anomalies (e.g., crossed fused ectopia, and horseshoe kidney) and complete fusion anomalies (e.g., fused pelvic kidney). Fusion anomalies are often associated with abnormalities of renal rotation, migration, and vascular supply, which predispose the kidneys to a number of complications and create difficulty during retroperitoneal surgeries and interventions. They are also associated with other congenital abnormalities of the urogenital tract, gastrointestinal tract, cardiovascular system, and skeletal system. This review summarizes the embryological basis, clinical presentation and imaging approach to renal fusion anomalies, followed by detailed anatomical and radiological description of the morphological types, and the complications associated with these anomalies.
Embryological basis
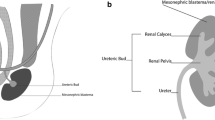
Genesis of fusion anomalies occur in the early embryonic period [1]. Renal development begins in the 4th week of gestation with the formation of nephrogenic cords in the intermediate mesoderm. The kidneys develop from three systems that succeed each other; namely, the pronephros, mesonephros, and metanephros. The metanephros, which is the final system to develop during the 5th week, induces the development of the ureteric bud as an outgrowth from the mesonephric duct. During the early stages of development, the kidneys lie close to each other in the presacral region and receive blood supply from the neighboring pelvic branches of the dorsal aorta. As gestation advances, growth of the lumbosacral region causes the kidneys to relatively ascend to their final position in the lumbar region, between the 6th and 9th weeks. The kidneys then are supplied by new vascular branches from the neighboring dorsal aorta, and the lower pelvic branches regress or form accessory renal arteries [2, 3]. The origin of renal fusion anomalies has not been completely understood; however, several theories have been suggested.
(a) Arterial fork theory This is the most widely accepted theory, according to which both kidneys ascend close to each other between the arterial fork formed by the umbilical arteries [1, 4, 5]. Any change in the course of the umbilical arteries leads to apposition of the developing kidneys and results in fusion.
(b) Abnormal caudal flexion and rotation theory Renal fusion anomalies can be symmetrical (horseshoe kidney with midline fusion), or asymmetrical (horseshoe kidney with lateral fusion and crossed fused ectopia). Symmetrical fusion anomalies result from factors which affect both kidneys simultaneously and equally, as seen with abnormal ventral flexion of the caudal fetus, which delays the ascent of kidneys and results in fusion. Asymmetrical fusion anomalies result from factors that differentially affect the two kidneys, such as abnormal lateral flexion or rotation of the caudal fetus. Association of fusion anomalies with abnormalities of the caudal spine supports this hypothesis [4].
(c) Theory of abnormal ureteral development This theory suggests that renal fusion anomalies result from an abnormal converging course of the ureteric buds that forces the metanephric blastema to fuse [5].
(d) Theory of abnormal metanephric migration According to this theory, a teratogenic event in the early renal development causes abnormal migration of the metanephric cells across the primitive streak, resulting in fusion. Association of fusion anomalies with renal tumors supports this theory [4, 6].
(e) Genetic theory No single genetic cause has been unequivocally linked with the development of renal fusion anomalies. Observations such as male preponderance, familial clustering and association with chromosomal abnormalities (Turner and Edward syndromes) suggest a genetic association [4].
Clinical features
The presentation of renal fusion anomalies peaks at three age groups: (a) young children, in whom the anomalies are discovered in combination with other, more significant congenital malformations; (b) puberty, due to associated genital tract abnormalities which result in delayed menarche; and (c) in adults, as an incidental imaging finding [7].
Majority of the patients with renal fusion anomalies are asymptomatic for the anomaly and are incidentally detected on imaging or autopsy. These patients do not require any specific treatment. Symptoms, when they occur, are often related to other congenital or acquired conditions associated with renal fusion anomalies, such as urinary tract obstruction from pelviureteric junction obstruction, calculus formation, vesicoureteric reflux, recurrent urinary tract infection, renovascular hypertension, susceptibility to trauma, and an increased risk of malignancies [8, 9].
Imaging approach
Prenatal USG demonstrates the fetal kidneys from as early as 9–12 weeks of gestation and corticomedullary differentiation from 15 weeks. Thus, antenatal USG can be used to detect major congenital renal anomalies. The USG should include evaluation of the presence, location, size, echogenicity and fusion of the kidneys, along with examination of the urinary bladder, external genitalia, and amniotic fluid [10]. Detection of renal abnormalities warrants postnatal physical examination and ultrasonography at birth and 4–6 weeks postpartum [8].
Transabdominal USG is often the first imaging performed in both children and adults. It helps in evaluating the location, size, and orientation of the kidneys and assess the presence of fusion. However, it is limited by operator dependence, reduced sensitivity in obese patients, and poor detection of horseshoe kidneys with fibrous isthmus [8, 11].
Intravenous urography (IVU) can demonstrate abnormal location and orientation of the kidneys and pelvicalyceal system, along with the course of the ureters and rough assessment of the excretory renal function. However, it cannot be used to differentiate between parenchymal and fibrous isthmus in horseshoe kidneys, or demonstrate complex vascular anatomy [11,12,13].
Cross-sectional imaging (CT/MR urography) helps in evaluating complex renal anatomy, relationship with adjacent structures, vascular anatomy, and complications. CT is better in the evaluation of certain complications such as calculus disease and trauma. Hence, CT urography is considered the investigation of choice for the evaluation of renal fusion anomalies [8, 11, 12]. MRI may be more valuable in the pediatric population due to the lack of ionizing radiation.
Nuclear medicine studies, often done for other indications, may incidentally detect the presence of fusion anomalies by the identification of abnormal location, orientation, and fusion of the kidneys [11]. They may also be used to assess for complications in fusion anomalies, such as urinary tract obstruction and vesicoureteric reflux (VUR).
Morphological types
Horseshoe kidney
Horseshoe kidney is the most common renal fusion anomaly, accounting for 90% of all cases. It has an incidence of 1 in 400–600 live births and a male-to-female ratio of 2:1 [11, 14].
Morphology Horseshoe kidney is a type of partial fusion anomaly, characterized by two distinct functioning kidneys on either side of the vertebral column. Generally, the inferior poles of the kidneys are directed medially and fuse across the midline, forming an isthmus of functioning renal parenchyma (80%) or fibrotic tissue. The isthmus is usually located anterior to the aorta and inferior vena cava (IVC) and prevents the normal ascension of kidneys above the origin of the inferior mesenteric artery (L3 vertebral level). Thus, the isthmus may be located anywhere along the path of normal ascent, occurring at the L4 vertebral level (40%), L3 vertebral level (40%), or the pelvis (20%). Fusion also prevents normal rotation of kidneys and hence, the renal pelvis is oriented anteriorly rather than anteromedially. The ureters often show an abnormally high union with the renal pelvis, course laterally as they cross the anterior surface of the isthmus, and assume a normal medial course further inferiorly [11, 14].
Classification Horseshoe kidney is classified as symmetrical and asymmetrical. Symmetrical horseshoe kidney is characterized by midline fusion, either at the inferior pole (U-shaped; most common; 90%), superior pole (inverted U-shaped), or both poles (disc kidney). Rarely, the superior pole of one kidney may fuse with the inferior pole of the other (S-shaped or sigmoid kidney). Asymmetrical horseshoe kidney is characterized by lateral fusion of the kidneys and is usually left-dominant [1]. These variants of fusion are demonstrated in Fig. 1.

Morphological types of horseshoe kidney
The arterial supply of horseshoe kidney is variable and several classification systems have been proposed [1]. One of the simpler surgical classification systems divides horseshoe kidneys into type I, where the two renal arteries arise from the normal position; type II, where, one or more ectopic arteries are seen arising from distal aorta or iliac arteries in addition to the orthotopic renal arteries; and type III, where all the renal arteries are ectopic in origin (Fig. 2). Variations in venous drainage are also described in horseshoe kidney [1].

Variant arterial anatomy in horseshoe kidneys (Type 1: renal arteries arising from the normal position, type 2: one or more ectopic renal arteries arising from the distal aorta or iliac arteries in addition to the normal orthotopic renal arteries, type 3: all renal arteries arising ectopically)
Imaging Plain radiographs show medially placed lower poles of the kidneys, which converge towards the spine. This appearance is contrary to the normal, where the upper poles are located medially and the renal axis parallels the outer margin of the psoas. IVU demonstrates medially rotated lower pole calyces facing the spine, referred to as the ‘hand holding calyces’ (Fig. 3a). The ureters curve laterally as they cross the isthmus, before assuming a normal medial course. This appearance is known as the ‘flower vase appearance’ (Fig. 3b). On USG, horseshoe kidneys should be suspected in the presence of inferiorly located, malrotated kidneys that appear unexpectedly small in the oblique sagittal images due to poor visualization of the lower pole. In such cases, observation of a preaortic soft tissue (isthmus) helps in establishing the diagnosis [15] (Fig. 3c, d). CT and MRI are excellent modalities capable of demonstrating the complex parenchymal, vascular and urinary tract anatomy of fusion anomalies. A parenchymal isthmus can be differentiated from a fibrotic isthmus by the presence of a soft tissue showing comparable enhancement to the renal parenchyma [8, 12] (Fig. 4, 5).

IVU and sonographic appearance of horseshoe kidney in a 25-year-old man with right flank pain. a 5-min delayed IVU spot image (supine) shows medially directed lower poles of both kidneys with closely placed lower pole calyces, giving the ‘hand holding calyces’ appearance. b 15-min delayed spot image (prone) shows lateral course of the ureters over the isthmus and normal medial course further inferiorly, giving the ‘flower vase appearance’. c On the oblique sagittal USG image, the right kidney appears unexpectedly small with poor visualization of the lower pole. d Axial USG image confirms the presence of a midline preaortic isthmus (asterisk) anterior to the aorta

U-shaped horseshoe kidney with a parenchymal isthmus, incidentally detected in a 32-year-old man evaluated for loculated pleural effusion. a Oblique coronal CECT image shows midline fusion of the kidneys at the lower poles through an enhancing parenchymal isthmus (asterisk). b Oblique sagittal image shows the location of the isthmus anterior to aorta, inferior to origin of the inferior mesenteric artery (arrow). c Cinematic rendered and d coronal CECT images show orthotopic renal arterial supply from the aorta (solid arrows) as well as ectopic supply (isthmic artery) from the right common iliac artery (dashed arrows). e, f Curved reformatted coronal CECT images show orthotopic renal venous drainage into the inferior vena cava (solid arrows) and ectopic venous drainage into the right common iliac vein (dashed arrow)

U-shaped horseshoe kidney with a fibrous isthmus incidentally detected in a 47-year-old man evaluated for suspected inflammatory bowel disease. a Oblique coronal CECT image shows medially placed lower poles of the kidneys, converging towards the spine. b Axial CECT image shows a non-enhancing, fibrous isthmus at the site of fusion (arrow)
Crossed fused ectopia
Crossed fused ectopia is the second most common renal fusion anomaly, with an incidence of 1 in 1300–7500 live births and a male predominance [1, 14].
Morphology Crossed fused ectopia is a type of partial fusion anomaly characterized by the presence of an ectopic kidney that crosses the midline and fuses with the orthotopic contralateral kidney. The ureter of the ectopic kidney crosses the midline, with the ureteric orifice located orthotopically. Most commonly, the left kidney is ectopic [1, 14].
Classification McDonald and McClellan classified crossed fused ectopia into 6 types: (a) inferior ectopia, the most common type, which shows unilateral fusion with inferior location of the ectopic kidney relative to the orthotopic kidney; (b) sigmoid or S-shaped kidney, the second most common type, where the ectopic kidney is located inferior to orthotopic kidney and is axially rotated relative to the latter; (c) lump kidney, where there is extensive renal fusion forming an irregular renal mass/lump; (d) L-shaped kidney, where ectopic is transversely oriented and the upper pole of the ectopic kidney fuses with the lower pole of the orthotopic kidney; (e) doughnut or disc kidney, where there is fusion along the medial concave surface of both the kidneys; and (f) superior ectopia (least common type), where there is unilateral fusion with the ectopic kidney located superior to the orthotopic kidney [16]. These different types are demonstrated in Fig. 6.

Morphological types of horseshoe kidney
Imaging IVU demonstrates the ectopic location and fusion of the affected kidney in the contralateral side, with the ureter crossing the midline to insert into the bladder orthotopically (Fig. 7). Crossed fused ectopia is identified on USG by the absence of kidney on one side and its ectopic location in the contralateral lumbar/iliac region. Fusion is identified by the presence of anterior and posterior notches in the resultant elongated renal mass, and by the presence of two separate renal sinuses. Identification of ureteral jet on USG may suggest the diagnosis of crossed fused ectopia when the ipsilateral kidney is not visualized [17]. CT and MR urography help to confirm the diagnosis and demonstrate detailed anatomy of the anomaly [8, 18] (Fig. 8).

IVU appearance of crossed fused ectopia in two different individuals, demonstrated on the 15-min delayed spot images. a The left kidney is ectopically located on the right side, inferior to the right kidney. The two kidneys are axially rotated in comparison to each other with the pelvis of the right kidney directed medially and that of the ectopic left kidney directed laterally, suggestive of S-shaped ectopia. b The right kidney is ectopically located on the left side, inferior to the left kidney, and has a transverse orientation, suggestive of L-shaped ectopia. In both the cases, the ureter of the ectopic kidney is crossing the midline and orthotopically opening into the urinary bladder

Inferior crossed fused ectopia incidentally detected in a 32-year-old man. a Oblique coronal, b sagittal and c cinematic rendered CECT images show ectopic location and fusion of the right kidney to the inferior pole of the orthotopic left kidney without axial rotation (both the renal hila facing anteromedially). d On the maximum intensity projection urographic phase image, the right ureter is observed to cross the midline and drain into the urinary bladder on the right side
Fused pelvic kidney
Fused pelvic kidney (also known as pancake or cake kidney) is one of the rarest fusion anomalies with an estimated incidence of 1 in 65,000–375,000 and a male predominance [14, 19].
Morphology Pancake kidney is a complete renal fusion anomaly characterized by the presence of a pelvic renal mass formed by extensive medial fusion of both kidneys. Pancake kidney is drained by two short ureters, which do not cross the midline (unlike crossed ectopia) and have orthotopic insertion in the urinary bladder. Rarely, a pancake kidney may be drained by a single ureter. The pancake kidney often retains primitive renal vasculature and may have a single renal artery (arising from the distal aorta or iliac arteries) and vein (draining into the IVC or iliac veins) which increases the risk of compromise from pelvic trauma, pregnancy, and neoplasms [1].
Imaging Pancake kidney is characterized by the absence of kidneys in the renal fossa, their ectopic paramedian location in the pelvis, and presence of extensive medial fusion. Each kidney often has two separate collecting systems draining into the respective anteriorly placed renal pelvises, and short ipsilateral ureters that do not cross midline before inserting into bladder orthotopically [20, 21] (Fig. 9).

Pancake kidney, incidentally detected in a 27-year-old man. a Oblique coronal, b axial, and c cinematic rendered CECT images show the ectopic location of both kidneys in the greater pelvis, with extensive medial fusion. d Coronal maximum intensity projection image of the urographic phase shows the short course of the ureters (dashed arrows), which drain orthotopically without crossing the midline. Two tiny calculi are noted in the left kidney (arrow)
Complications
Renal fusion anomalies are often asymptomatic and picked-up incidentally. However, by virtue of their anatomy, they are predisposed to number of complications such as pelviureteric junction obstruction (PUJO), multicystic dysplastic kidney (MCDK), VUR, renal stones, recurrent renal infections, trauma, and neoplasms [11, 14, 22].
Associated anomalies
Pelviureteric junction obstruction (PUJO)
PUJO is the most common associated finding in renal fusion anomalies. The specific causes of obstruction include (a) congenital narrowing at the PUJ, (b) abnormally high insertion of the ureter into renal pelvis, causing delayed emptying and stasis, (c) narrowing due to the proximal ureter coursing over the isthmus, and (d) pelviureteric compression by aberrant renal vessels. On imaging, the pelvis is disproportionately dilated and ballooned-out with abrupt transition at the PUJ and a collapsed ureter (Fig. 10). The presence of abnormal course of the ureter and aberrant renal arteries also can be assessed on cross-section imaging [11, 14, 22].

Horseshoe kidney with right PUJ obstruction and scoliosis in a 25-year-old man who presented with right flank pain. a Axial CECT image shows a dilated right renal pelvis (arrow). b Volume rendered image of the urographic phase shows a ballooned-out right renal pelvis with transition at the pelviureteric junction. Thoracolumbar levoscoliosis is also present
Multicystic dysplastic kidney (MCDK)
MCDK is often the result of intrauterine urinary tract obstruction, commonly PUJ obstruction. It is often unilateral, left sided, and asymptomatic; however, may be associated with other urinary tract abnormalities in the contralateral kidney such as PUJO and VUR. When bilateral, MCDK is incompatible with life. On imaging, the affected kidney is small in size and replaced by multiple non-communicating cysts without any appreciable parenchyma [11, 22].
Vesicoureteric reflux (VUR)
VUR is frequently associated with renal fusion anomalies, with an incidence of 50% in horseshoe kidney [11, 14]. Bhatnagar et al. observed that 4 out of 6 patients with crossed fused renal ectopia had VUR [23]. The gold standard for the evaluation of VUR is micturating cystourethrogram (MCU). Nuclear medicine studies such as direct and indirect radionuclide cystography can also be used to evaluate VUR. IVU, CT urography, and conventional MRI lack the functional information to demonstrate VUR, however, may show secondary changes such as hydroureteronephrosis and cortical scarring [11, 22].
Other anomalies
Renal fusion anomalies can be associated with partial or complete duplication of the ureters (Fig. 11), abnormal ureteric course (e.g. retrocaval ureter) (Fig. 12), and ectopic ureteric insertion. Other associated anomalies include persistent urogenital sinus, cloacal malformation, VACTERL (vertebral anomaly, anorectal malformation, cardiac defect, trachea-esophageal fistula, renal abnormality, and limb anomaly), Edward and Turner syndrome. Imaging helps in the detailed evaluation of malformations and plays a pivotal role in planning surgery [14].

Horseshoe kidney with partial duplication of the left ureter in a 24-year-old lady with recurrent urinary tract infection. a 5-min and b 15-min delayed IVU spot images show medially directed lower pole calyces (hand holding calyces), duplication of the left pelvicalyceal system, and partial duplication of the left ureter with orthotopic opening of the left ureter into the urinary bladder

Horseshoe kidney with retrocaval ureter in a 35-year-old man with right flank pain. a Axial CECT image shows horseshoe kidney with a midline parenchymal isthmus located anterior to the aorta. b Delayed urographic phase oblique axial image shows right hydronephrosis with transition at the retrocaval course of the right ureter (arrows). c Cinematic rendered image shows medial deviation of the ureter at the location of the retrocaval course (dashed arrow)
Renal stone disease
Renal stones are a common complication of fusion anomalies, with a prevalence of 16–60% in horseshoe kidney [11] (Fig. 13). They are often a consequence of urinary stasis or recurrent infection secondary to PUJO, VUR, or abnormal orientation of the pelvicalyceal system. Renal stones are often multiple, with a predisposition to the formation of staghorn calculi and xanthogranulomatous pyelonephritis [11, 22].

Horseshoe kidney with left renal calculus in a 52-year-old male patient with left flank pain. a Plain radiograph shows a large lamellated calculus in the left flank region (arrow). b 15-min Delayed IVU spot image shows ‘hand holding’ lower pole calyces and a ‘flower vase’ appearance of the ureters, suggestive of horseshoe kidney. A filling defect is seen in the lower pole calyx (dashed arrow), corresponding to the calculus seen in the plain radiograph. c Axial USG image confirms the calculus (calipers) in the left kidney
Renal infections
Renal infections commonly occur in renal fusion anomalies and are seen in approximately one-third of the patients with horseshoe kidneys. Predisposing factors include stasis, obstruction, reflux, and stone disease that are frequently associated with renal fusion anomalies. The most common route is ascending infection, usually in association with VUR.
IVU demonstrates pyelonephritis as an enlarged kidney with striated nephrogram, which may be better appreciated on CECT. CT and MRI show enlarged kidneys with perinephric fat stranding and occasionally, abscess formation. Uncontrolled infection may lead to abscess formation. Diabetic patients may develop emphysematous pyelonephritis, a more severe form of the disease, characterized by intrarenal and perinephric air foci [11, 22].
Traumatic kidney injury
Fusion anomalies predispose the kidneys to traumatic injury. Horseshoe kidney is more vulnerable to trauma due to its lower, more anterior position and lack of protection by the rib cage. Also, the midline isthmus is particularly vulnerable to compression injuries against the spine. PUJO, when present, increases the risk of injury to the upper urinary tract. CECT is modality of choice in assessing traumatic renal injury and demonstrates renal lacerations, intrarenal or perinephric hematoma, vascular and collecting system injury. Thus, it assists in grading and triage, and in planning the management [11, 14, 22].
Renal neoplasms
Fusion anomalies are associated with both benign and malignant tumors of the kidneys. This predisposition has been attributed to a teratogenic insult in the early embryonic period that acts as a common precursor to the development of the fusion anomaly and oncogenesis. The isthmus is the most common site of neoplasms. RCC accounts for 45% of all the tumors seen in horseshoe kidneys (Fig. 14). However, some studies suggest that the risk of RCC in a horseshoe kidney is the same as the general population [24]. Horseshoe kidney is also at an increased risk for transitional cell carcinoma, Wilms’ tumor, neuroendocrine tumors, squamous cell carcinoma, and oncocytoma compared to the general population. TCC accounts for 28% of all the tumors and the increased risk has been attributed to stasis, calculi, and recurrent infections observed in these patients. Primary renal leiomyosarcoma is another very rare tumor associated with horseshoe kidneys. It arises from the renal capsule, or the smooth muscle cells in the renal pelvis and blood vessels [11]. Malignancy in crossed fused ectopia is extremely rare [11, 14, 22, 25]. Imaging plays an important role in planning the surgical approach, which may be different from that of normal patients. In patients where preoperative embolization of the renal mass is considered, CT or MR angiography may be necessary to evaluate the variable vascular anatomy seen in fusion anomalies [26].

Horseshoe kidney with clear cell renal carcinoma in a 69-year-old man with hematuria for 3 months. a Oblique coronal and b axial CECT images show horseshoe kidney with a well-defined, partially exophytic mass at the upper pole of the left kidney. The mass shows peripheral hyperenhancement and central necrotic areas
Conclusion
Renal fusion anomalies are relatively common congenital malformations with complex anatomical features. The three main types include the horseshoe kidney, crossed fused ectopia and the fused pelvic kidney. Although, most cases are asymptomatic, fusion anomalies predispose the kidneys to a number of complications, such as urinary tract obstruction and reflux, renal stones, recurrent renal infections, trauma, and neoplasms. Knowledge of the complex imaging anatomy of the fusion anomalies and their associated complications helps in planning appropriate therapy. Imaging plays a significant role in evaluation of these complex fusion anomalies as well as early detection of their complications.
References
Babu Csr, Sharma V, Gupta OP. Renal Fusion Anomalies: A Review of Surgical Anatomy. Anat Physiol [Internet]. 2015 [cited 2020 Oct 26];s5. Available from: https://www.omicsonline.org/open-access/renal-fusion-anomalies-a-review-of-surgical-anatomy-2161-0940-S5-001.php?aid=57809
Libretti S, Aeddula NR. Embryology, Genitourinary. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 [cited 2020 Oct 27]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK559309/
Rehman S, Ahmed D. Embryology, Kidney, Bladder, and Ureter. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 [cited 2020 Oct 27]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK547747/
Taghavi K, Kirkpatrick J, Mirjalili SA. The horseshoe kidney: Surgical anatomy and embryology. J Pediatr Urol. 2016 Oct;12(5):275–80.
Doménech-Mateu JM, Gonzalez-Compta X. Horseshoe kidney: A new theory on lts embrogenesis based on the study of a 16-mm human embryo: horseshoe kidney morphogenesis. Anat Rec. 1988 Dec;222(4):408–17.
Natsis K, Piagkou M, Skotsimara A, Protogerou V, Tsitouridis I, Skandalakis P. Horseshoe kidney: a review of anatomy and pathology. Surg Radiol Anat. 2014 Aug;36(6):517–26.
Glodny B, Petersen J, Hofmann KJ, Schenk C, Herwig R, Trieb T, et al. Kidney fusion anomalies revisited: clinical and radiological analysis of 209 cases of crossed fused ectopia and horseshoe kidney. BJU Int. 2009 Jan;103(2):224–35.
Ramanathan S, Kumar D, Khanna M, Al Heidous M, Sheikh A, Virmani V, et al. Multi-modality imaging review of congenital abnormalities of kidney and upper urinary tract. World J Radiol. 2016 Feb 28;8(2):132–41.
Surabhi VR, Menias CO, George V, Matta E, Kaza RK, Hasapes J. MDCT and MR Urogram Spectrum of Congenital Anomalies of the Kidney and Urinary Tract Diagnosed in Adulthood. Am J Roentgenol. 2015 Sep;205(3):W294–304.
Hindryckx A, De Catte L. Prenatal diagnosis of congenital renal and urinary tract malformations. Facts Views Vis ObGyn. 2011;3(3):165–74.
Shah H, Ojili V. Multimodality imaging spectrum of complications of horseshoe kidney. Indian J Radiol Imaging. 2017;27(2):133.
Antil N. Horseshoe Kidney: From Womb To Tomb. 2018;2999 words.
Hameed BZ, Chawla A, Hegde P, Vasa T. Crossed Fused Ectopia of Kidney – An Account of Tertiary Healthcare Center Experience. Open Urol Nephrol J. 2018 Mar 30;11(1):1–13.
Chan SS, Ntoulia A, Khrichenko D, Back SJ, Tasian GE, Dillman JR, et al. Role of magnetic resonance urography in pediatric renal fusion anomalies. Pediatr Radiol. 2017 Dec;47(13):1707–20.
Nahm A-M, Ritz E. Horseshoe kidney. Nephrol Dial Transplant. 1999 Nov 1;14(11):2740–1.
Mcdonald JH, Mcclellan DS. Crossed renal ectopia. Am J Surg. 1957 Jun;93(6):995–1002.
Mudoni A, Caccetta F, Caroppo M, Musio F, Accogli A, Zacheo MD, et al. Crossed fused renal ectopia: case report and review of the literature. J Ultrasound. 2017 Dec;20(4):333–7.
Benitez CM, Cyr DR, Mack LA. Crossed Fused Renal Ectopia: A Sonographic Diagnosis. J Diagn Med Sonogr. 1985 Sep;1(5):218–20.
Lomoro P, Simonetti I, Vinci G, Fichera V, Prevedoni Gorone MS. Pancake kidney, a rare and often misdiagnosed malformation: a case report and radiological differential diagnosis. J Ultrasound. 2019 Jun;22(2):207–13.
Singhal PM, Vats M, Agarwal M, Neogi S. Pancake kidney: an incidental finding in a young man. BMJ Case Rep. 2018 Oct 2;bcr-2018-226751.
Choudhary AK, Tiwari AK, Khowal H, Chaudhary P, Arora MP. Pancake kidney: A rare developmental anomaly. Can Urol Assoc J. 2014 Jun 19;8(5–6):451.
O’Brien J, Buckley O, Doody O, Ward E, Persaud T, Torreggiani W. Imaging of horseshoe kidneys and their complications. J Med Imaging Radiat Oncol. 2008 Jun;52(3):216–26.
Bhatnagar V, Gupta A, Kumar R, Solanki S. Crossed fused renal ectopia: Challenges in diagnosis and management. J Indian Assoc Pediatr Surg. 2013;18(1):7.
Rubio Briones J, Regalado Pareja R, Sánchez Martín F, Chéchile Toniolo G, Huguet Pérez J, Villavicencio Mavrich H. Incidence of tumoural pathology in horseshoe kidneys. Eur Urol. 1998;33(2):175–9.
Stimac G, Dimanovski J, Ruzic B, Spajic B, Kraus O. Tumors in kidney fusion anomalies–report of five cases and review of the literature. Scand J Urol Nephrol. 2004;38(6):485–9.
Palmowski M, Kiessling F, López-Benítez R, Kauffmann GW, Hallscheidt P. Preoperative embolization of a tumor-bearing horseshoe kidney via both channels of a concomitant aortic dissection. Cardiovasc Intervent Radiol. 2007 Jun;30(3):501–3.
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Nil.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kubihal, V., Razik, A., Sharma, S. et al. Unveiling the confusion in renal fusion anomalies: role of imaging. Abdom Radiol 46, 4254–4265 (2021). https://doi.org/10.1007/s00261-021-03072-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-021-03072-1