
Abstract
A variety of vascular liver disorders can induce hepatocellular tumors. They may be related to portal venous deprivation, venous outflow obstruction, or arterial diseases. Their common feature is an imbalance between hepatic arterial and portal venous blood flow leading to an increased hepatic arterial inflow. Consequently, hepatocellular tumors may arise, most commonly focal nodular hyperplasia-like lesions but hepatocellular adenomas and hepatocellular carcinoma may be seen as well. This article will review the most common vascular liver diseases associated with hepatocellular nodules (Budd–Chiari syndrome, congenital portosystemic shunt, hereditary hemorrhagic telangiectasia, and portal cavernoma). For each condition, imaging findings will be described as well as the differential diagnosis and the diagnostic clues.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Because of its dual blood supply, the liver is peculiar, with 70–80% derived from the portal vein and 20–30% from the hepatic artery. These two vessels connect at different levels, so that any decrease in portal blood flow is compensated by an increase in arterial flow [1]. Portal vein resistance increases in the presence of chronic hepatic venous system defects leading to an increase in hepatic arterial flow. Finally, certain arterial disorders may cause an increase in arterial flow. Increased hepatic arterial flow probably plays a role in the development of hepatocellular liver tumors. This has been experimentally confirmed in animal models in which hyperplastic liver lesions develop following surgical portosystemic shunts [2]. On the other hand, portocaval shunts preserving blood flow to the liver do not lead to liver tumors [3]. In a population of children who underwent portosystemic shunt surgery for extrahepatic portal vein obstruction, seven out of 45 (15%) developed liver nodules after a median of 80 months [4]. This article describes hepatocellular tumors that develop in patients with vascular liver diseases (Table 1).
Budd–Chiari syndrome
Budd–Chiari syndrome (BCS) is defined by an obstruction of the hepatic venous outflow tract in the absence of right heart failure or constrictive pericarditis. Since the 1990s and with advances in liver imaging, benign regenerative nodules have been described in association with BCS resulting in a significant improvement in patient survival [5]. These benign regenerative nodules are only found in chronic BCS, and mostly correspond to focal nodular hyperplasia (FNH). They have both the same macroscopic and microscopic features as FNH as well as displaying a map-like pattern of glutamine synthase expression [6]. Because they develop on an unhealthy liver, they are usually called focal nodular hyperplasia-like (FNH-like) lesions. These lesions do not seem to be associated with specific causes of BCS. It is not clear if interventional procedures such as TIPS play a role in the development of these lesions because they can grow spontaneously over time [7]. The exact prevalence of these regenerative lesions is difficult to determine, but in a large imaging series of BCS, liver nodules were observed in 28/77 (36%) of patients [8]. On imaging, they share common imaging features with traditional FNH. They are homogeneous and hypervascular and the largest lesions often contain a central scar [8, 9] However, certain imaging features differ from those of FNH such as hyperintensity on T1-weighted and variable signal T2-weighted MR images (either iso-, hypo-, or hyperintense). Indeed, when liver lesions are hyperintense on precontrast fat-suppressed T1-weighted images, subtraction from precontrast images must be performed to evaluate hyperenhancement. Because other liver tumors may develop in BCS, the most discriminant imaging features are number and size. In most cases, there are numerous FNH-like lesions (often more than 10) and they are no larger than 3 cm in diameter [8, 10,11,12,13]. The diagnosis can be difficult because (i) they may increase in size and/or in number [8, 14], (ii) there may be wash-out on contrast-enhanced CT or MR imaging during portal venous and/or delayed phase (probably because of increased signal intensity of the surrounding liver due to liver congestion); (iii) the pathologic diagnosis can be difficult in the absence of specific immunohistochemistry; and (iv) other hepatocellular lesions such as hepatocellular adenomas (HCA) or hepatocellular carcinoma (HCC) may develop in BCS (Fig. 1).

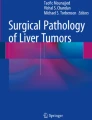
Drawings representing liver vessels and liver nodules developed on most common vascular diseases. A Normal liver vessels anatomy and normal liver enhancement. B Budd–Chiari syndrome. Abnormal hepatic veins showing complete occlusion, marked stenosis, and hepatic venous collaterals. Decreased portal vein diameter and increased hepatic artery diameter resulting in increased liver enhancement on arterial-phase imaging (liver appears brighter than normal liver in A). Multiple FNH-like lesions are hypervascular on arterial-phase imaging. C Congenital portosystemic shunt. Complete portal flow deprivation and increased hepatic artery diameter resulting in increased liver enhancement on arterial-phase imaging (liver appears brighter than normal liver in A). FNH-like lesions (often large) are hypervascular on arterial-phase imaging. D Hereditary haemorrhagic telangiectasia. Marked increased in size of hepatic arteries with arteriovenous and portovenous shunts (dotted circles). Increased patchy liver enhancement on arterial-phase imaging (liver appears brighter than normal liver in A). Multiple FNH-like lesions are hypervascular on arterial-phase imaging. E Cavernous transformation of the portal vein. Extrahepatic portal vein obstruction with portal cavernoma and increased hepatic artery diameter resulting in increased enhancement in peripheral liver segments on arterial-phase imaging. Multiple small-sized FNH-like lesions are hypervascular on arterial-phase imaging
A multicenter pathological series of liver nodules associated with BCS showed that FNH-like lesions were the most frequent. Nevertheless, four of 27 FNH-like lesions reported in the initial pathological report were not confirmed as FNH-like lesions and two were HCAs (one inflammatory and one exon 3 beta-catenin mutated) [15] (Fig. 2).

A 27-year-old female with chronic Budd–Chiari syndrome related to a myeloproliferative neoplasm. TIPS placement. Two FNH-like lesions stable over time (arrows). A On T2-weighted MR imaging, the liver nodules are not seen. B On fat-suppressed T1-weighted MR imaging, two small-sized hyperintense lesions (in segment 4 and in the caudate lobe) are observed. C On contrast-enhanced T1-weighted MR sequence at the arterial phase, the lesions enhance on arterial phase (enhancement was also seen on substraction image, not shown). D, E They become isointense to the liver on portal venous and delayed phases. F On hepatobiliary phase, the lesions are strongly hyperintense relative to the liver. Note the morphologic liver changes and the splenomegaly
Hepatocellular carcinoma (HCC) is also a risk in patients with BCS (11/97 patients in a cohort with a mean 5-year follow-up), and thus these patients should be monitored [10]. Serum alpha-fetoprotein (AFP) is specific for HCC in these cases [10,11,12,13, 16]. It should be noted that patients with long-term IVC obstruction are at a higher risk of developing HCC than those with pure hepatic vein involvement [10, 16]. HCC usually appears hypervascular, heterogeneous, and solitary on imaging. The histological diagnosis is very difficult because HCC are usually very highly differentiated tumors (Fig. 3).

A 50-year-old female with chronic Budd–Chiari syndrome related to coagulation disorders. One 3-cm liver lesion in segment 5 diagnosed as hepatocellular carcinoma on histology (arrow). A On T2-weighted MR imaging, the liver lesion is moderately hyperintense. B On fat-suppressed T1-weighted MR imaging, the liver lesion is hypointense. C, D On contrast-enhanced T1-weighted MR sequence, the lesion enhances on arterial phase and does not show wash-out on portal venous phase. E: The lesion shows wash-out on delayed phase. F On hepatobiliary phase, the lesion is hypointense relative to the liver
The differences between FNH-like lesions and HCC have been reported in a study on contrast-enhanced ultrasound. While enhancement of most FNH-like lesions was center-to-periphery and it remained hyperechoic on portal venous and delayed phases, enhancement of most HCCs was heterogenous on arterial phase and hypoechoic on portal and delayed phases [13]. Nevertheless, the diagnosis between FNH-like lesions and HCC remains difficult at imaging and hepatobiliary MR contrast agents may help [17] but have not been extensively evaluated. Therefore, specific diagnosis requires extensive clinical, laboratory, and imaging work-up including, if possible, MR imaging with hepatobiliary MR contrast agents. If liver lesions have the predefined features of FNH-like lesions and AFP levels are low, patients should be followed up every six months by clinical, laboratory, and imaging assessment. If imaging features are atypical, if significant changes occur over time, or if serum AFP becomes elevated, a liver biopsy should be performed. There is no existing evidence that benign regenerative nodules become malignant but the number of studies is limited [18].
Congenital portosystemic shunts
Portosystemic shunts in patients without a history of trauma, liver biopsy, portal vein thrombosis, cirrhosis, or portal hypertension are considered congenital. The features of shunts vary since they can be intra- or extra-hepatic, simple or multiple, and they may induce partial or complete portal blood deprivation. They are classified as portohepatic (portal-to-hepatic vein), portocaval, and patent ductus venosus [19]. Congenital portosystemic shunts have been associated with genetic or chromosomic abnormalities as well as with congenital heart disease and the polysplenia syndrome. Although they may be clinically asymptomatic, they can also be revealed by severe complications in childhood, such as hepatopulmonary syndrome, encephalopathy, or heart failure.
The development of benign regenerative liver lesions is well known and seems to be related to major portal deprivation [20]. Thirteen out of 17 patients with portosystemic shunts had liver tumors in a pediatric study [21]. Although most patients have multiple liver nodules that are mostly FNH-like lesions, hepatocellular adenoma (HCA) or regenerative nodular hyperplasia can also be seen [20]. Ten of the 16 nodules from a series of five patients who underwent liver transplantation were FNH-like lesions, five were beta-catenin-mutated HCAs, and one was an inflammatory HCA [22]. It is interesting to note that FNH-like lesions are more often atypical on imaging than in patients with normal livers and may enlarge over time [20, 23]. These atypical lesions may be explained by complete and chronic portal blood deprivation. In children, shunt closure by interventional procedures or surgery can restore intrahepatic portal flow following complete or partial regression of benign liver lesions [21].
However, caution should be taken in the diagnosis of benign regenerative lesions because reports of HCCs are rare in patients with congenital portosystemic shunts [24]. Because patients with congenital portosystemic shunts and HCC are much older than those with benign hepatocellular tumors, HCC may arise on preexisting HCA, and in particular b-catenin-mutated HCA [15, 22]. As in BCS, contrast-enhanced imaging should look for imaging patterns observed in FNH-like lesions. Liver biopsy should be considered especially in patients with atypical lesions at imaging (Fig. 4).

A 22-year-old female with congenital portosystemic shunt and a FNH-like lesion (arrow). A On ultrasound, the lesion is homogeneous and isoechoic to the liver. B, C On T2-weighted and on fat-suppressed T1-weighted MR imaging, the liver lesion is isointense to the liver and contains a central scar that is hyperintense on T2-weighted and hypointense on T1-weighted MR imaging. D, E On contrast-enhanced T1-weighted MR sequence, the lesion enhances on arterial phase and does not show wash-out on portal venous phase. The central scar enhances on portal venous phase. The congenital portosystemic shunt is between the right portal branch and the inferior vena cava
Hereditary hemorrhagic telangiectasia
Hereditary hemorrhagic telangiectasia (HHT), also known as Rendu–Osler–Weber syndrome, is an autosomal dominant disorder that interferes with angiogenesis and its control mechanisms. Liver involvement is frequently associated with mutations in the ALK1 gene mutations (type 2) and is observed in 67–84% of HHT patients [25]. Vascular abnormalities include microscopic telangiectasia and direct arteriovenous, arterioportal, and portovenous shunts resulting in an increase in hepatic arterial flow. Thus, HHT favors the development of diffuse nodular regenerative hyperplasia and FNH-like lesions [26,27,28]. In one study, the estimated prevalence of FNH-like lesions in HHT was 2.9%. This is significantly higher than in the general population [29]. In that study, most patients with FNH-like lesions had severe hepatic shunts and were women [29]. During follow-up, some FNH-like lesions may increase in size or HHT may be revealed by multiple FNH-like lesions without visible intrahepatic shunts on imaging. The diagnosis of FNH-like lesions in HHT patients is based on traditional imaging. Precontrast and contrast-enhanced MRI with hepatobiliary contrast agents may differentiate FNH-like lesions from large telangiectasia. Liver biopsy is normally contraindicated in HHT because of a higher risk of bleeding. However, it may be considered when imaging is atypical.
Other hepatocellular tumors (HCA and HCC) seem to be extremely uncommon in HHT, and HCA and HCC were not observed in the pathological study by Sempoux et al [15]. Rare cases of HCC associated with HHT have been reported [30] (Fig. 5).

A 16-year-old male with multiple liver lesions. No known disease at diagnosis. A, B On T2- and T1-weighted MR imaging, the liver looks homogeneous. C, D On contrast-enhanced T1-weighted MR sequences, multiple liver lesions enhance on arterial phase and are moderately hyperintense on portal venous phase. E On hepatobiliary phase, all the lesions are hyperintense relative to the liver confirming the diagnosis of FNH-like lesions. The diagnosis of hereditary hemorrhagic telangiectasia was made on the presence of epistaxis in the patient and in the family. Note that contrast-enhanced MR imaging does not show intrahepatic arteriovenous shunts
Cavernous transformation of the portal vein
Cavernous transformation of the portal vein (CTPV) is a compensatory response of portal vein thrombosis that aims to restore portal blood flow in the liver. As CTPV is insufficient to provide substantial portal venous inflow far from the hilum, it is associated with an increase in hepatic arterial flow especially in the peripheral liver segments. These changes in liver hemodynamics alter liver morphology with central liver hypertrophy and peripheral liver atrophy [31].
Case reports have described benign hepatocellular nodules in patients with CTPV [32, 33]. A series of 58 CTPV patients identified 12 (21%) patients with FNH-like lesions and one with HCA. Although most FNH-like lesions were typical on contrast-enhanced CT or MRI, a central scar was often lacking due to their small size. They were scattered throughout the liver and did not predominate in the hyperarterialized segments.
The diagnosis of these lesions is based on imaging. Indeed, the diagnostic value of iso- or hyperintense lesions on hepatobiliary phase MR is good. Like other vascular disorders of the liver, the size and number of FNH-like lesions may increase over time [34]. HCA and HCC are rare in these cases [35].
Other vascular disorders
Certain non-cirrhotic liver diseases leading to severe portal hypertension and/or liver congestion can also induce benign regenerative nodules.
FNH-like lesions have been described in obliterative portal venopathy and congenital hepatic fibrosis [36, 37].
Benign liver lesions seem to be more common in patients with sinusoidal obstruction syndrome [38] and have been reported in children with malignant tumors receiving high-dose chemotherapy or undergoing hematopoietic stem cell transplantation (Fig. 6). They are considered to be a late manifestation of sinusoidal obstruction syndrome [39]. One case report and one series have described FNH-like lesions in adult patients with colorectal cancer following oxaliplatin-based chemotherapy [39, 40]. All lesions in that series either had typical imaging patterns or were histologically confirmed as FNH. It is interesting to note that the average time between the end of oxaliplatin treatment and the identification of these lesions on imaging was 4 years. Most patients presented with new lesions or the growth of existing lesions at imaging follow-up.

A 41-year-old male who had nephrectomy for nephroblastoma in childhood. During follow-up, a liver lesion was depicted on imaging (arrow). A, B On contrast-enhanced CT, the lesion is strongly hypervascular on arterial phase and nearly iso-attenuating on portal venous phase. C, D The liver lesion is isointense to the liver on T2-weighted and slightly hypointense on fat-suppressed T1-weighted MR imaging. E Contrast-enhanced T1-weighted MR sequence during the arterial phase showing strong lesion enhancement. The lesion becomes isointense on portal venous phase (not shown). F On hepatobiliary phase, marked enhancement in the periphery of the lesion characteristic of benign hepatocellular lesion is observed. A biopsy confirms the diagnosis of FNH-like lesion, probably secondary to undiagnosed sinusoidal obstruction syndrome related to chemotherapy in the childhood
Hepatocellular lesions may also develop in patients with long-term right cardiac insufficiency or chronic constrictive pericarditis.
Liver nodules have also been described in patients after the Fontan surgical procedure. This procedure provides definitive palliation for patients with single-ventricle resulting in an anastomosis between the vena cava or right atrium and the pulmonary arteries and causing chronic passive liver congestion. Complex liver involvement is common following this procedure, from passive venous congestion to hepatic ischemia and chronic congestive hepatopathy (previously known as cardiac cirrhosis) [41]. HCC is a late complication of the Fontan Procedure usually in the presence of cirrhosis, and thus regular screening should be performed [42, 43]. However, FNH-like lesions are especially frequent in patients with high Fontan pressures [44]. In these cases, like BCS, the diagnosis of FNH-like lesions compared to HCC is difficult, especially in the presence of cirrhosis. A diagnosis requires knowledge of the liver underlying disease, careful analysis of the liver lesions, and serum AFP. Certain patients with a cardiac pacemaker or implantable defibrillator may have contra-indications for MRI and biopsy is recommended in case of doubt.
In conclusion, numerous vascular disorders of the liver are associated with hepatocellular tumors. FNH-like lesions are the most common but other benign tumors may also be found, including focal nodular regenerative hyperplasia and HCA. Imaging, and especially MRI, plays a major role in the diagnosis, which can still be more difficult than in normal livers. A histopathological examination may be required. The size and number of these benign lesions may increase over time, while HCC is rare except in patients with BCS or following a Fontan procedure.
References
Itai Y, Matsui O (1997) Blood flow and liver imaging. Radiology 202:306–314
Weinbren K, Washington SL (1976) Hyperplastic nodules after portacaval anastomosis in rats. Nature 264:440–442
Rasenack U (1981) Changes in the liver and brain after portacaval and modified portacaval end-to-side anastomosis: histology, autoradiography and clinical studies. Fortschr Med 99:107–112
Guerin F, Porras J, Fabre M, et al. (2009) Liver nodules after portal systemic shunt surgery for extrahepatic portal vein obstruction in children. J Pediatr Surg 44:1337–1343
Valla DC (2008) Budd-Chiari syndrome and veno-occlusive disease/sinusoidal obstruction syndrome. Gut 57:1469–1478
Kim H, Nahm JH, Park YN (2015) Budd-Chiari syndrome with multiple large regenerative nodules. Clin Mol Hepatol 21:89–94
Tanju S, Erden A, Ceyhan K, et al. (2004) Contrast-enhanced MR angiography of benign regenerative nodules following TIPS shunt procedure in Budd-Chiari syndrome. Turk J Gastroenterol 15:173–177
Vilgrain V, Lewin M, Vons C, et al. (1999) Hepatic nodules in Budd-Chiari syndrome: imaging features. Radiology 210:443–450
Maetani Y, Itoh K, Egawa H, et al. (2002) Benign hepatic nodules in Budd-Chiari syndrome: radiologic-pathologic correlation with emphasis on the central scar. AJR Am J Roentgenol 178:869–875
Moucari R, Rautou PE, Cazals-Hatem D, et al. (2008) Hepatocellular carcinoma in Budd-Chiari syndrome: characteristics and risk factors. Gut 57:828–835
Sakr M, Abdelhakam SM, Dabbous H, et al. (2017) Characteristics of hepatocellular carcinoma in Egyptian patients with primary Budd-Chiari syndrome. Liver Int 37:415–422
Gwon D 2nd, Ko GY, Yoon HK, et al. (2010) Hepatocellular carcinoma associated with membranous obstruction of the inferior vena cava: incidence, characteristics, and risk factors and clinical efficacy of TACE. Radiology 254:617–626
Zhang R, Qin S, Zhou Y, Song Y, Sun L (2012) Comparison of imaging characteristics between hepatic benign regenerative nodules and hepatocellular carcinomas associated with Budd-Chiari syndrome by contrast enhanced ultrasound. Eur J Radiol 81:2984–2989
Flor N, Zuin M, Brovelli F, et al. (2010) Regenerative nodules in patients with chronic Budd-Chiari syndrome: a longitudinal study using multiphase contrast-enhanced multidetector CT. Eur J Radiol 73:588–593
Sempoux C, Paradis V, Komuta M, et al. (2015) Hepatocellular nodules expressing markers of hepatocellular adenomas in Budd-Chiari syndrome and other rare hepatic vascular disorders. J Hepatol 63:1173–1180
Paul SB, Shalimar Sreenivas V, et al. (2015) Incidence and risk factors of hepatocellular carcinoma in patients with hepatic venous outflow tract obstruction. Aliment Pharmacol Ther 41:961–971
Renzulli M, Lucidi V, Mosconi C, et al. (2011) Large regenerative nodules in a patient with Budd-Chiari syndrome after TIPS positioning while on the liver transplantation list diagnosed by Gd-EOB-DTPA MRI. Hepatobiliary Pancreat Dis Int 10:439–442
Brancatelli G, Federle MP, Grazioli L, Golfieri R, Lencioni R (2002) Benign regenerative nodules in Budd-Chiari syndrome and other vascular disorders of the liver: radiologic-pathologic and clinical correlation. Radiographics 22:847–862
Blanc T, Guerin F, Franchi-Abella S, et al. (2014) Congenital portosystemic shunts in children: a new anatomical classification correlated with surgical strategy. Ann Surg 260:188–198
Pupulim LF, Vullierme MP, Paradis V, et al. (2013) Congenital portosystemic shunts associated with liver tumours. Clin Radiol 68:e362–369
Franchi-Abella S, Branchereau S, Lambert V, et al. (2010) Complications of congenital portosystemic shunts in children: therapeutic options and outcomes. J Pediatr Gastroenterol Nutr 51:322–330
Sanada Y, Mizuta K, Niki T, et al. (2015) Hepatocellular nodules resulting from congenital extrahepatic portosystemic shunts can differentiate into potentially malignant hepatocellular adenomas. J Hepatobiliary Pancreat Sci 22:746–756
Kim T, Murakami T, Sugihara E, et al. (2004) Hepatic nodular lesions associated with abnormal development of the portal vein. AJR Am J Roentgenol 183:1333–1338
Lisovsky M, Konstas AA, Misdraji J (2011) Congenital extrahepatic portosystemic shunts (Abernethy malformation): a histopathologic evaluation. Am J Surg Pathol 35:1381–1390
Sabba C, Pompili M (2008) Review article: the hepatic manifestations of hereditary haemorrhagic telangiectasia. Aliment Pharmacol Ther 28:523–533
Wanless IR, Gryfe A (1986) Nodular transformation of the liver in hereditary hemorrhagic telangiectasia. Arch Pathol Lab Med 110:331–335
Scardapane A, Ficco M, Sabba C, et al. (2013) Hepatic nodular regenerative lesions in patients with hereditary haemorrhagic telangiectasia: computed tomography and magnetic resonance findings. Radiol Med 118:1–13
Brenard R, Chapaux X, Deltenre P, et al. (2010) Large spectrum of liver vascular lesions including high prevalence of focal nodular hyperplasia in patients with hereditary haemorrhagic telangiectasia: the Belgian Registry based on 30 patients. Eur J Gastroenterol Hepatol 22:1253–1259
Buscarini E, Danesino C, Plauchu H, et al. (2004) High prevalence of hepatic focal nodular hyperplasia in subjects with hereditary hemorrhagic telangiectasia. Ultrasound Med Biol 30:1089–1097
Lee JH, Lee YS, Kim PN, et al. (2011) Osler-Weber-Rendu disease presenting with hepatocellular carcinoma: radiologic and genetic findings. Korean J Hepatol 17:313–318
Vilgrain V, Condat B, Bureau C, et al. (2006) Atrophy-hypertrophy complex in patients with cavernous transformation of the portal vein: CT evaluation. Radiology 241:149–155
Ribera Cano A, Debette-Gratien M, Descottes B, Languepin J (2007) Focal nodular hyperplasia involving portal cavernoma. Arch Pediatr 14:1315–1317
Bureau C, Peron JM, Sirach E, et al. (2004) Liver nodules ressembling focal nodular hyperplasia after portal vein thrombosis. J Hepatol 41:499–500
Marin D, Galluzzo A, Plessier A, et al. (2011) Focal nodular hyperplasia-like lesions in patients with cavernous transformation of the portal vein: prevalence, MR findings and natural history. Eur Radiol 21:2074–2082
Amarapurkar P, Bhatt N, Patel N, Amarapurkar D (2014) Primary extrahepatic portal vein obstruction in adults: a single center experience. Indian J Gastroenterol 33:19–22
Zeitoun D, Brancatelli G, Colombat M, et al. (2004) Congenital hepatic fibrosis: CT findings in 18 adults. Radiology 231:109–116
Glatard AS, Hillaire S, d’Assignies G, et al. (2012) Obliterative portal venopathy: findings at CT imaging. Radiology 263:741–750
Sudour H, Mainard L, Baumann C, et al. (2009) Focal nodular hyperplasia of the liver following hematopoietic SCT. Bone Marrow Transplant 43:127–132
Furlan A, Brancatelli G, Dioguardi Burgio M, et al. (2017) Focal nodular hyperplasia after treatment with oxaliplatin: a multi-institutionnel series of cases diagnosed on MR imaging. AJR Am J Roentgenol (in press)
Donadon M, Di Tommaso L, Roncalli M, Torzilli G (2013) Multiple focal nodular hyperplasias induced by oxaliplatin-based chemotherapy. World J Hepatol 5:340–344
Hilscher MB, Johnson JN, Cetta F, et al. (2017) Surveillance for liver complications after the Fontan procedure. Congenit Heart Dis 12:124–132
Josephus Jitta D, Wagenaar LJ, Mulder BJ, et al. (2016) Three cases of hepatocellular carcinoma in Fontan patients: Review of the literature and suggestions for hepatic screening. Int J Cardiol 206:21–26
Wells ML, Hough DM, Fidler JL, et al. (2017) Benign nodules in post-Fontan livers can show imaging features considered diagnostic for hepatocellular carcinoma. Abdom Radiol (NY) 42:2623–2631
Bryant T, Ahmad Z, Millward-Sadler H, et al. (2011) Arterialised hepatic nodules in the Fontan circulation: hepatico-cardiac interactions. Int J Cardiol 151:268–272
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No funding.
Conflict of interest
None of the authors have any conflict of interest.
Rights and permissions
About this article

Cite this article
Vilgrain, V., Paradis, V., Van Wettere, M. et al. Benign and malignant hepatocellular lesions in patients with vascular liver diseases. Abdom Radiol 43, 1968–1977 (2018). https://doi.org/10.1007/s00261-018-1502-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-018-1502-7