
Abstract
The purpose of this article is to focus attention on the abnormalities which the radiologist may encounter in patients presenting with lateral ankle or foot pain outside of the context of acute trauma. These include anterolateral impingement, subfibular impingement, subtalar instability and tarsal sinus syndrome, tarsal coalition, sural neuromas, peroneal tendon abnormalities, calcaneocuboid instability and occult cuboid fractures, and painful accessory ossicles. The expected and unexpected findings on radiographs, CT, US, and MRI are discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The foot provides a stable base for weight-bearing; it is also a flexible construct for locomotion. The 27 foot bones (not including sesamoids) function together to perform complex motions.
There are 3 divisions of the foot from posterior to anterior: hindfoot (talus and calcaneus), midfoot (remaining tarsal bones), and forefoot (metatarsals and phalanges). Locomotion proceeds through the 3 divisions, with heel strike on the calcaneus propelling the limb forward into the MTP joints before the toe off phase of gait.
Another way of understanding the functional anatomy of the foot is by dividing it into 2 or 3 longitudinal columns, which are subject to differing stresses. In the 2-column system, the medial column consists of the talus, navicular, cuneiforms, and the 1st–3rd metatarsals, while the lateral column of the foot is composed of the calcaneus, cuboid, and 4th and 5th metatarsals. In the 3-column system, a middle column is added, consisting of the 2nd and 3rd cuneiforms and corresponding digits. A patient may present with pain in the lateral column because of abnormal alignment, abnormal stresses, missed injury, or overuse. This review will focus on the imaging evaluation of the painful lateral column.
The bones of the foot form longitudinal and transverse arches, both centered in the midfoot, and both higher medially than laterally. The cuneiforms form the medial keystone of both arches, and the cuboid is the lateral keystone. An abnormally high arch (pes cavus) or flattened arch (pes planus) will alter foot biomechanics.
Progressive collapsing foot deformity and the lateral column
Flatfoot or pes planus can be broadly divided into congenital and acquired types. The congenital, flexible flatfoot is a benign condition, while the acquired flatfoot is often associated with pain, posterior tibial tendon dysfunction, and osteoarthritis. The term progressive collapsing foot deformity (PCFD) has been recommended [1] as a replacement for the term acquired flatfoot, in order to emphasize the progressive nature of the deformity and to widen the clinical focus from posterior tibial tendon dysfunction to other abnormalities which are also present. The alignment abnormalities of PCFD include flattening of the longitudinal arch, hindfoot valgus, midfoot or forefoot abduction, and dynamic midfoot varus [2]. Hindfoot valgus is lateral deviation of the calcaneus relative to the tibia. It can be assessed on clinical exam, and with radiographic evaluation, optimally including the hindfoot alignment view [3].
Although the majority of research in PCFD is concerned with abnormalities of the medial column, PCFD will increase stress on the lateral column. Lateral column abnormalities associated with PCFD include impingement on the tarsal sinus, the calcaneus and peroneal tendons [4], stress fractures of the cuboid and fifth metatarsal, and osteoarthritis of the calcaneocuboid and 4th–5th tarsometatarsal joints. Each of these will be discussed separately below.
A variety of osteotomies are performed to counter PCFD [1, 2, 5,6,7]. Hindfoot valgus is often addressed surgically by a medializing osteotomy of the calcaneus. A dorsal opening wedge osteotomy of the medial cuneiform is employed to elevate the medial arch. Forefoot/midfoot abduction is often countered by a lengthening osteotomy of the lateral column at the anterior portion of the calcaneus, or by calcaneocuboid fusion. It is important to note that although calcaneal lengthening is performed to counter forefoot abduction, the length of the lateral column in PCFD is usually normal in this deformity [5, 8]. Surgical lateral column lengthening can unfortunately create lateral column pain, sometimes associated with excessive lengthening [5, 7]. Calcaneal lengthening for treatment of flatfoot in children has been associated with a high prevalence of postoperative calcaneocuboid and talonavicular osteoarthritis [9], but no data are available on the prevalence of this finding in adults.
The cavovarus foot and the lateral column
A cavovarus foot can be due to Charcot-Marie-Tooth disease and other neuromuscular disorders, and leads to increased weightbearing on the lateral column. Lateral column pain in the cavovarus foot may occur due to peroneal tendon abnormalities and stress fractures of the 4th and 5th metatarsals, discussed below.
Painful lateral hindfoot impingement
There are several causes of painful impingement in the lateral hindfoot: anterolateral impingement, subfibular impingement, and tarsal sinus impingement.
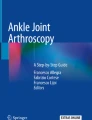
Tears of the anterior talofibular ligament are very common, and often asymptomatic. Occasionally, the torn ligament may form a bulky, triangular scar, called a meniscoid lesion, in the anterolateral ankle joint recess. This causes anterolateral ankle pain and impingement with eversion and dorsiflexion of the ankle [10]. The meniscoid lesion is well seen on axial MRI (Fig. 1). Meniscoid lesions may also develop from a scarred anterior inferior tibiofibular ligament. In addition, debris, loose bodies, and synovitis may cause anterolateral impingement.

A 40-year old man who developed anterolateral impingement after repeated ankle sprains. He complained of both impingement symptoms and instability. Axial T2W MRI shows a meniscoid lesion (arrow) and lateral gutter ankle osteoarthritis (arrowhead), both confirmed at time of surgery
Subfibular impingement frequently occurs due to hindfoot valgus, which results in impingement of the tip of the fibula against the tarsal sinus, the lateral margin of the calcaneus, the calcaneofibular ligament, or the peroneal tendons. It can also occur due to a malunited calcaneal fracture, due to loss of height of the calcaneus. Radiographs can show bony impingement, subtalar subluxation, and bony remodeling (Fig. 2A–C). MRI characteristically shows bone marrow edema due to impingement, and findings of tarsal sinus syndrome, with amorphous material filling the tarsal sinus (Fig. 2D–F). Tears of the interosseous talocalcaneal ligaments may contribute to impingement on the tarsal sinus [10, 11].

A 60-year old woman presenting with PCFD and chronic lateral ankle pain. Imaging shows subfibular impingement, subtalar subluxation, and tarsal sinus syndrome. A. AP radiograph shows that the tip of the fibula is abutting the lateral margin of the calcaneus (arrow), B. Mortise radiograph, slightly overly rotated, shows that there is subluxation of the subtalar joint (arrows) and subchondral sclerosis at the lateral articular margin of the talus. Note the inferior position of the fibular tip (arrowhead) relative to the calcaneus, C. Lateral radiograph shows severe pes planus. The lateral process of the calcaneus is sclerotic and remodeled (arrow), due to patient’s underlying subtalar instability. Note that a “C” sign, commonly associated with tarsal coalition, is present despite the absence of a coalition. A “C” sign can also occur due to pronation of the foot, D. Sagittal STIR MR shows bone marrow edema (arrows) centered at the lateral process of the talus and the calcaneal angle of Gissane, due to abnormal subtalar motion, E. Coronal T1WI shows amorphous, intermediate signal intensity material (arrow) filling the tarsal sinus, and calcaneal reactive changes (arrowhead), F. Coronal T2WIFS shows increased signal intensity in the material (arrow) filling the tarsal sinus. However, in many cases, this amorphous material remains low signal intensity on fluid-sensitive sequences
Tarsal coalition
Tarsal coalitions are bony, cartilaginous or fibrous bridges between 2 or more tarsal bones [12]. Coalitions cause pain, typically in the dorsal, lateral hindfoot, due to restricted motion. Historically, tarsal coalitions are described as presenting in the 2nd decade of life, but they are often detected later. Patients may present because of repeated ankle sprains. About half of tarsal coalitions are associated with flatfoot deformity. Tarsal coalitions are easily overlooked on radiographs. Plain radiographic signs of tarsal coalition include the anteater sign, elongation of the lateral portion of the navicular, C-sign, and talar beak [12, 13].
Missed hindfoot fractures
A review of major injuries to the foot is beyond the scope of this review, but 2 fractures should be considered which are sometimes overlooked and may have a delayed presentation and nonunion, and present with chronic lateral hindfoot pain: lateral process talus and anterior process calcaneus fractures. Fractures of the lateral process of the talus occur due to an inversion injury, which results in incongruity of the subtalar joint and compresses the lateral process between the fibula and calcaneus. They may be extra-articular or may involve both the posterior subtalar joint and the talofibular portion of the ankle joint. Lateral process fractures are difficult to see on radiographs, and often visible on the lateral view of the ankle only. They are readily seen on CT or MRI (Fig. 3). If missed, intra-articular lateral process fractures have a high risk of rapidly developing subtalar osteoarthritis.

A 21-year old man who flipped his go cart and suffered a lateral process talus fracture, A. Lateral radiograph only faintly shows the fracture (arrow), although it is usually best seen on this view, B. AP radiograph shows fracture line and bony prominence (arrow) inferior to the fibular tip, consistent with lateral process talus fracture, C. Coronal CT shows that the fracture (arrow) involves the posterior subtalar joint and is comminuted
Anterior process calcaneus fracture can occur due to compression of the process during an eversion injury, or to avulsion by the bifurcate calcaneo-cuboid-navicular ligament during inversion. They are best seen on lateral or oblique views of the hindfoot (Fig. 4). If missed, the patient may present with a painful nonunion. Fractures of the extensor digitorum brevis origin are often also missed, but they appear to reliably heal and there is no literature to suggest that they go on to painful nonunion. They can be distinguished from anterior process fractures because they are located further laterally, along the dorsum of the calcaneus, slightly proximal to the articular surface.

A 23-year old woman who suffered an inversion injury of the ankle, and sustained an anterior process calcaneus fracture, A. Lateral radiograph shows fracture (arrow) which is easily missed due to overlying structures, B. Sagittal CT confirms the fracture (arrow)
Peroneal tendon disorders
Peroneal tendon disorders are often associated not only with PCFD, but also with chronic ankle instability [14], or with an enlarged peroneal tubercle [15], which separates the peroneus brevis from the peroneus longus inferior to it (Fig. 5). They have also been associated with pes cavovarus [16]. A peroneus quartus muscle is a normal variant which may cause pain by increasing pressure on the peroneal tendons as they course beneath the peronal retinaculum.

A 30-year old woman with a prominent peroneal tubercle of the calcaneus, asymptomatic in this area, A. Coronal PD MR shows the normal peroneus brevis (arrowhead) superior to the tubercle, and the normal peroneus longus (arrow) inferior to it. Signal intensity in the tendons is slightly higher than expected, due to magic angle phenomenon, B. T2FS image confirms normal signal intensity in the tendons. Magic angle artifact decreases with increasing TE
Abnormalities of the peroneal tendons range from tenosynovitis to tendinopathy and partial or complete tear. The peroneal tendons are well evaluated on both ultrasound and MRI [17, 18]. A limitation of ultrasound is that it is difficult to evaluate the peroneus longus distal to the cuboid sulcus. In chronic tenosynovitis, adhesions may develop between the tendon and the tendon sheath, limiting motion; this phenomenon is designated stenosing tenosynovitis.
Injuries of the peroneus brevis usually present clinically with retromalleolar pain or pain inferior to the tip of the fibula. It is common to develop splitting of the peroneus brevis (Fig. 6), and minor splitting may be asymptomatic.

A 45-year old female with subfibular ankle pain and a split tear of the peroneus brevis tendon. Short axis US through the peroneal tendons adjacent to the calcaneus shows fluid in the tendon sheath. There is longitudinal splitting of the peroneus brevis (arrowhead), creating the appearance of a duplicated tendon on this image, and heterogeneity in the peroneus longus (arrow)
Injuries of the peroneus longus tend to occur at the level of the cuboid sulcus or distal to it, as the tendon extends obliquely across the plantar surface of the foot. Tears usually present with pain at the peroneal tubercle or cuboid sulcus. Distal tears are easily missed on MRI because of the oblique course of the tendon; careful cross referencing of different MRI planes is needed to distinguish between tendinosis and tear (Fig. 7).

A 48-year old runner with a complete tear of the plantar portion of the peroneus longus tendon, A. Oblique radiograph shows that the os peroneum (arrow) is displaced proximal to the calcaneocuboid joint. This is an uncommon but specific sign of peroneus longus tendon tear, B. Axial T2FS MR shows the peroneal tendon is thickened and wavy prior to entering the cuboid groove (arrow), and has a frayed appearance (arrowhead) more distally, C. Coronal T2FS MR confirms absence of the distal peroneal tendon, with fluid filling its bed (arrow)
The os peroneum is present in the peroneus longus tendon in 20% of the population. A fibrocartiliginous nodule may be present in the same region, perhaps an anlage to an ossicle. When an os peroneum is present, displacement proximal to the calcaneocuboid joint is a reliable sign of peroneus longus tear (Fig. 7) [15, 19]. The os peroneum may fracture, due to acute injury. This must be distinguished from a bipartite or multipartite ossicle. When patients have peroneal tenosynovitis, the os peroneum may develop painful periostitis; asymptomatic periosteal reaction can also occur in patients with diffuse idiopathic skeletal hyperostosis (DISH).
The painful os peroneum syndrome (POPS) refers to a variety of conditions causing pain in the region of the os peroneum [20]. These include ossicular fracture, impingement of the ossicle against the cuboid (peroneocuboid joint, Fig. 8) or against a prominent peroneal tubercle, and peroneus tendon rupture adjacent to an os peroneum.

35 yo woman with os peroneum impingement, complaining of chronic, worsening lateral midfoot pain after starting a power walking program 1 year prior to imaging, A. Oblique radiograph shows os peroneum (arrowhead) which has developed a facet medially, articulating with a similar adventitious facet of the cuboid (arrow), B. Axial T2WFS MR shows the articulation of the ossicle (arrowhead) with the cuboid, and the extensive bone marrow edema in the cuboid (arrow)
Cuboid fractures and cuboid pulley lesion
Disruptions of the longitudinal arch often affect the cuboid and may lead to stress fractures. Cuboid stress fractures are reportedly uncommon [21,22,23], and for that reason, there is limited data about predisposing factors. Stress fractures of the cuboid have been associated with abnormalities of the plantar fascia and the posterior tibial tendon, both of which contribute to maintenance of the longitudinal arch of the foot. A study of 10 patients with isolated cuboid stress fracture found that 9 showed abnormal plantar fascia, 7 showed abnormal peroneal tendons, and 4 showed abnormal posterior tibial tendon [23].
A cuboid stress fracture is distinguished from the cuboid pulley lesion, which is reactive bone marrow edema related to abnormalities of the peroneus longus as it passes through the cuboid tunnel, sometimes seen in the setting of inflammatory arthritis [24].
Isolated traumatic cuboid fractures are often not apparent on radiographs, and for that reason may have a delayed presentation when an MRI is performed for persistent lateral column pain (Fig. 9) [25].

A 36-year old man with an osteochondral cuboid fracture due to landing hard during a basketball game, A. Oblique radiograph shows the area of the fracture, which was not detected prospectively, but can be seen in hindsight (arrow), B. Axial T2WFS MR shows bone marrow edema surrounding a crescentic subchondral fracture (arrow) characteristic of osteochondral fracture
Calcaneocuboid instability
Calcaneocuboid joint instability may develop in dancers and other athletes, due to inversion and plantar flexion, but the prevalence is not known [26]. It has been associated with ankle sprains, and with chronic or acute injury to the bifurcate ligament or calcaneocuboid ligaments [27]. Patients complain of lateral hindfoot pain that limits activity. Physical examination will elicit pain when a dorsal force is applied to the plantar aspect of the cuboid. Stress radiographs are sometimes used for diagnosis [28], but defined criteria are not yet published. Radiographs rarely show a bony avulsion of the dorsal capsular ligament. It must be remembered that weightbearing radiographs of the normal foot often show slight incongruity of the calcaneocuboid joint, and this tends to increase on nonweightbearing radiographs, so this should not be mistaken for instability. MRI may show disruption of the joint capsule/dorsal calcaneocuboid ligament or bifurcate ligament (Fig. 10).

A 13-year old avid athlete with calcaneocuboid instability, presenting as chronic lateral midfoot pain and difficulty running or dancing. Patient was treated with ligament reconstruction, and had returned to sports with minimal discomfort at 1-year follow-up, A. Axial T2FS MR shows focal tear of the dorsal calcaneocuboid ligament (arrow) and extravasation of joint fluid through the tear, B. Coronal T2FS MR at the calcaneocuboid joint shows extracapsular fluid (arrow) from ligament tear
Sural neuropathy
The sural nerve is a small sensory nerve to the lower lateral leg, lateral heel, and dorsal lateral foot. The nerve may be injured with fractures of the fibula or 5th metatarsal, or Achilles or gastrocnemius injury. It also may be affected by postsurgical scarring. Patients with sural neuropathy may have burning pain or loss of sensation. Because of the oblique plane of the nerve, neuromas are easily overlooked on MRI, but easily seen on ultrasound [29] (Fig. 11).

A 61-year old woman with a postsurgical sural neuroma, presenting with burning lateral hindfoot pain after gastrocnemius recession, A. Axial T1W MR shows a sural neuroma (arrow). Despite the presence of a marker at the patient’s site of maximum pain, the neuroma was not noticed. It was not visible in other planes due to the obliquity of the nerve relative to standard imaging planes, B. Ultrasound along the course of the sural nerve in the posterior hindfoot shows the normal nerve (arrowhead) with focal fusiform enlargement (arrow) indicating neuroma. Palpation of the neuroma reproduced the patient’s pain
Lateral midfoot osteoarthritis
The most common patterns for osteoarthritis of the midfoot involve both the talonavicular and calcaneocuboid joints (the Chopart joint), or the 1st–3rd tarsometatarsal joints. However, isolated lateral column osteoarthritis may develop due either to midfoot abduction or to excessive surgical lengthening of the lateral column.
Painful 4th and 5th metatarsals
Metatarsal stress fractures most commonly affect the 2nd and 3rd metatarsals. A stress fracture of the 4th or 5th metatarsal may be due to abnormal alignment. A small study of 11 patients with metatarsus adductus found stress fractures in the 4th and 5th metatarsals in that group [30].
Fractures of the proximal 5th metatarsal are divided into 3 zones: the tuberosity is zone 1; zone 2 is the metaphyseal–diaphyseal junction, and includes the intermetatarsal joint (Jones fracture); and zone 3 is the diaphysis up to 1.5 cm distal to the tuberosity [31]. Both zone 2 and zone 3 fractures are associated with a high risk of nonunion. Jones fractures are associated with pes cavovarus [32, 33].
The Jones fracture, a transverse fracture of the proximal shaft of the 5th metatarsal, is often seen in soccer and American football players. The acute fracture is often preceded by 1–2 months of aching pain over the metatarsal [34], indicating that these are most likely stress fractures which go on to completion. Jones fractures have a high nonunion rate when treated with casting and immobilization, and for that reason are often treated with screw fixation. The Jones fracture has been correlated to forefoot adduction [35], as well as to a high medial longitudinal arch, and a more proximal styloid process [34].
The os vesalianum (Fig. 12) is an accessory ossicle at the styloid process of the 5th metatarsal base, at the site of attachment of the peroneus brevis tendon. Pain related to the ossicle is rarely reported, and is often but not always due to overuse [36]. The most reliable way to distinguish an os vesalianum from a nonunited fracture of the 5th metatarsal tuberosity is by size. The os vesalianum is larger and extends further proximally than a nonunited fracture. The ossicle will be expected to have rounded margins, while the fracture shows acute margins (Fig. 13). However, this distinction may not hold in chronic, nonunited fractures.

A. Oblique radiograph shows that the ossicle (arrow) has rounded, sclerotic margins and extends further posteriorly than the normal styloid process. These are both key points in distinguishing an os vesalianum from a fractured styloid process. There are small cysts at the synchondrosis between the ossicle and the 5th metatarsal. These are commonly seen and suggests some degree of motion at the synchondrosis. Note that the patient has a peroneal tubercle (arrowhead), B. Sagittal CT shows the rounded, sclerotic contour of the ossicle distinguishing it from acute fracture

A 22-year old woman presenting with a styloid process 5th metatarsal fracture after an inversion injury, A. Oblique radiograph shows the normal size of the styloid process, and an oblique fracture line (arrow). Unlike the rounded margins of the os vesalianum, the fracture margins are angular. Since the fracture is acute, the margins are not corticated, but a chronic, nonunited fracture will have corticated margins similar to those of an os vesalinum, B. Sagittal T1W MR confirms the acute fracture line (arrow)
The 5th metatarsal is the most mobile metatarsal, with varus–valgus mobility of 10–20° [37]. The bunionnette is a bony prominence of the lateral margin of the 5th metatarsal head. It may reflect an angle of more than 5° between the 4th and 5th metatarsals, a laterally bowed 5th metatarsal, or pes planus or hindfoot varus [37]. Bunionnetes are rarely painful, but may cause pain due to tightly fitting shoes. An adventitious bursa may form over the head of the 5th metatarsal.
Painful 4th–5th MTP joints
The 4th and 5th metatarsophalangeal joints are often the first joints in the foot to be affected by rheumatoid arthritis. The clinical picture of rheumatoid arthritis has changed dramatically since the advent of disease modifying medications, and it is uncommon today to see patients present with the classic radiographic findings of marginal erosions and joint subluxations. Occasionally, however, a patient will still present with those findings due either to a lack of medical care or to resistance to medications. If only a single MTP joint is involved, infection is the most likely cause of an erosive arthropathy. However, since the 4th and 5th metatarsals occupy different compartments, if both are involved, rheumatoid arthritis or other inflammatory arthropathy should be considered.
Conclusion
This review covers bony and soft tissue abnormalities of the lateral column from back to front. It is the author’s hope that this method of organizing the imaging approach to lateral foot pain will be useful.
References
Myerson MS, Thordarson DB, Johnson JE, Hintermann B, Sangeorzan BJ, Deland JT, et al. Classification and nomenclature: progressive collapsing foot deformity. Foot Ankle Int. 2020;41(10):1271–6.
Thordarson DB, Schon LC, de Cesar NC, Deland JT, Ellis SJ, Johnson JE, et al. Consensus for the indication of lateral column lengthening in the treatment of progressive collapsing foot deformity. Foot Ankle Int. 2020;41(10):1286–8.
Saltzman CL, El-Khoury GY. The hindfoot alignment view. Foot Ankle Int. 1995;16(9):572–6.
Lalevee M, Barbachan Mansur NS, Rojas EO, Lee HY, Ahrenholz SJ, Dibbern KN, et al (2021) Prevalence and pattern of lateral impingements in the progressive collapsing foot deformity. Arch Orthop Trauma Surg
Ellis SJ, Johnson JE, Day J, de Cesar NC, Deland JT, Hintermann B, et al. Titrating the amount of bony correction in progressive collapsing foot deformity. Foot Ankle Int. 2020;41(10):1292–5.
L CS, de Cesar Netto C, Day J, Deland JT, Hintermann B, Johnson JE, et al (2020) Consensus for the indication of a medializing displacement calcaneal osteotomy in the treatment of progressive collapsing foot deformity. Foot Ankle Int 41(10):1282–1285
Modha RK, Kilmartin TE (2021) Lateral column lengthening for flexible adult acquired flatfoot: systematic review and meta-analysis. J Foot Ankle Surg
Kang S, Charlton TP, Thordarson DB. Lateral column length in adult flatfoot deformity. Foot Ankle Int. 2013;34(3):392–7.
Sung KH, Kwon SS, Chung CY, Lee KM, Park MS. Radiographic changes of the mid-tarsal joint after calcaneal lengthening for planovalgus foot deformity. Foot Ankle Surg. 2020;26(1):110–5.
Donovan A, Rosenberg ZS. MRI of ankle and lateral hindfoot impingement syndromes. AJR Am J Roentgenol. 2010;195(3):595–604.
Lektrakul N, Chung CB, Lai Y, Theodorou DJ, Yu J, Haghighi P, et al. Tarsal sinus: arthrographic, MR imaging, MR arthrographic, and pathologic findings in cadavers and retrospective study data in patients with sinus tarsi syndrome. Radiology. 2001;219(3):802–10.
Crim J. Imaging of tarsal coalition. Radiol Clin North Am. 2008;46(6):1017-1026.vi.
BF DI, Fraga CJ, Cohen BE, Shereff MJ (2000) Associated injuries found in chronic lateral ankle instability. Foot Ankle Int 21(10):809–815
van Dijk PAD, Kerkhoffs G, Chiodo C, DiGiovanni CW. Chronic disorders of the peroneal tendons: current concepts review of the literature. J Am Acad Orthop Surg. 2019;27(16):590–8.
Taniguchi A, Alejandro SF, Kane JM, Daoud Y, Tanaka Y, Ford SE, et al. Association of cavovarus foot alignment with peroneal tendon tears. Foot Ankle Int. 2021;42(6):750–6.
Taljanovic MS, Alcala JN, Gimber LH, Rieke JD, Chilvers MM, Latt LD. High-resolution US and MR imaging of peroneal tendon injuries. Radiographics. 2015;35(1):179–99.
Molini L, Bianchi S. US in peroneal tendon tear. J Ultrasound. 2014;17(2):125–34.
Hallinan J, Wang W, Pathria MN, Smitaman E, Huang BK. The peroneus longus muscle and tendon: a review of its anatomy and pathology. Skeletal Radiol. 2019;48(9):1329–44.
Sobel M, Pavlov H, Geppert MJ, Thompson FM, DiCarlo EF, Davis WH. Painful os peroneum syndrome: a spectrum of conditions responsible for plantar lateral foot pain. Foot Ankle Int. 1994;15(3):112–24.
Franco M, Albano L, Kacso I, Gaid H, Jaeger P. An uncommon cause of foot pain: the cuboid insufficiency stress fracture. Joint Bone Spine. 2005;72(1):76–8.
Mandell JC, Khurana B, Smith SE. Stress fractures of the foot and ankle, part 2: site-specific etiology, imaging, and treatment, and differential diagnosis. Skeletal Radiol. 2017;46(9):1165–86.
Yu SM, Dardani M, Yu JS. MRI of isolated cuboid stress fractures in adults. AJR Am J Roentgenol. 2013;201(6):1325–30.
Chang MY, Hong SH, Yoo HJ, Choi JY, Chae HD, Moon SJ. MRI of Cuboid Pulley Lesion. AJR Am J Roentgenol. 2018;211(4):867–71.
O’Dell MC, Chauvin NA, Jaramillo D, Biko DM. MR imaging features of cuboid fractures in children. Pediatr Radiol. 2018;48(5):680–5.
Patterson SM. Cuboid syndrome: a review of the literature. J Sports Sci Med. 2006;5(4):597–606.
Traister E, Simons S. Diagnostic considerations of lateral column foot pain in athletes. Curr Sports Med Rep. 2014;13(6):370–6.
Lohrer H, Arentz S. Calcaneocuboid joint instability: a novel operative technique for anatomic reconstruction. Foot Ankle Int. 2004;25(5):349–56.
Bianchi S, Droz L, Lups Deplaine C, Dubois-Ferriere V, Delmi M. Ultrasonography of the sural nerve: normal and pathologic appearances. J Ultrasound Med. 2018;37(5):1257–65.
Theodorou DJ, Theodorou SJ, Boutin RD, Chung C, Fliszar E, Kakitsubata Y, et al. Stress fractures of the lateral metatarsal bones in metatarsus adductus foot deformity: a previously unrecognized association. Skeletal Radiol. 1999;28(12):679–84.
Lawrence SJ, Botte MJ. Jones’ fractures and related fractures of the proximal fifth metatarsal. Foot Ankle. 1993;14(6):358–65.
Raikin SM, Slenker N, Ratigan B. The association of a varus hindfoot and fracture of the fifth metatarsal metaphyseal-diaphyseal junction: the Jones fracture. Am J Sports Med. 2008;36(7):1367–72.
Jones CP. Cavovarus: Fifth metatarsal fractures and revision open reduction internal fixation. Clin Sports Med. 2020;39(4):793–9.
Porter DA. Fifth metatarsal jones fractures in the athlete. Foot Ankle Int. 2018;39(2):250–8.
Karnovsky SC, Rosenbaum AJ, DeSandis B, Johnson C, Murphy CI, Warren RF, et al. Radiographic analysis of national football league players’ fifth metatarsal morphology relationship to proximal fifth metatarsal fracture risk. Foot Ankle Int. 2019;40(3):318–22.
Fujitaka K, Tanaka Y, Taniguchi A, Ogawa M, Isomoto S, Otuki S, et al. Pathoanatomy of the Jones fracture in male university soccer players. Am J Sports Med. 2020;48(2):424–31.
Aykanat F, Vincenten C, Cankus MC, Kose O, Sindel M. Lateral foot pain due to os vesalianum pedis in a young football player; a case report and review of the current literature. Skeletal Radiol. 2019;48(11):1821–8.
Koti M, Maffulli N. Bunionette. J Bone Joint Surg Am. 2001;83(7):1076–82.
Author information
Authors and Affiliations
Contributions
Julia Crim: I attest that I am the sole author of this article, and responsible for its entirety.
Corresponding author
Ethics declarations
The author has nothing to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
IRB: The article is exempt from IRB review at the author’s institution. All data is HIPAA compliant, and histories have been changed to ensure anonymity.
Rights and permissions
About this article

Cite this article
Crim, J. The painful lateral column of the foot: from back to front. Skeletal Radiol 51, 1115–1125 (2022). https://doi.org/10.1007/s00256-021-03936-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-021-03936-z