
Abstract
Objectives
Compile the largest study to date on the imaging and clinical features of the classic spindle cell/pleomorphic lipoma spectrum and suggest this diagnosis be included in the differential for benign and malignant macroscopic fat-containing soft tissue masses regardless of the mass location or patient demographics.
Materials and methods
An institutional search was performed to identify all available classic-type spindle cell/pleomorphic lipomas with available demographic and imaging data. Images and reports were analyzed by one MSK-trained radiologist and radiographic, anatomic and clinical data were recorded. Additionally, a literature search was performed to identify studies describing the spindle cell lipoma spectrum imaging features and were combined with institutional data.
Results
Forty-two institutional cases were identified, 37 of which had MRIs performed among which 21 had images available (T1- and T2-weighted pulse sequences) for review while the remainder had outside reports detailing the mass imaging features. There was a mean age of 57 with 79% of cases occurring in males. Contrary to prior reports, 57% of masses were subcutaneous, and the neck and back region accounted for 26% of cases. When the institutional cases were combined with available data in the literature, there was a new sample size of 91 masses, 74 of which had MRI and/or CT data. Eighty-seven percent of masses were heterogeneous, 51% were composed of less than 75% fat, 65% were in the back, neck or shoulder region, 27% of masses were deep and 91% demonstrated enhancement. Eighty-two percent of patients were males with a mean age of 58 at excision.
Conclusion
Imaging features, patient demographics and tumor location alone are not enough to differentiate tumors of the spindle cell lipoma spectrum from other macroscopic fat-containing benign and malignant tumors, and these entities should be included in the same imaging differential diagnosis.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Macroscopic fat-containing soft tissue masses are frequently encountered when diagnostic imaging is performed. In addition to determining size and location, one of the primary objectives of MR or CT imaging is to determine whether a fat-containing soft tissue mass is benign or malignant. Several imaging features have been shown to increase the likelihood of a fat-containing sarcoma such as thick septations, size greater than 10 cm, nodular or mass-like regions and a composition of < 75% macroscopic fat [1]. Demographic information such as male gender, age > 60 and location in the lower extremity have also been associated with an increased likelihood of a fat-containing sarcoma [1]. However, in several small case series, these imaging and demographic features overlap with masses in the classic spindle cell/pleomorphic lipoma (SCPL) spectrum [2,3,4,5]. More recently, the cellular angiofibroma has also been described to be on the SCPL spectrum [6,7,8]. Cellular angiofibromas are typically located in the perineal and inguinal regions and may contain various amounts of adipose tissue. These three tumors share genetic similarities such as a loss of the retinoblastoma gene (Rb) and expression of the CD34 marker and are therefore thought to be related [6,7,8]. They also lack overexpression of mouse double minute 2 homolog (MDM2), a finding characteristic of atypical lipomatous tumors (ALTs)/well-differentiated liposarcomas (WDL) [9, 10]. Imaging features combined with mass location and patient demographics have been described as suggestive for SCPLs in prior case series and reports. Specifically, subcutaneous soft tissue masses located in the neck and back region in older male patients containing some degree of adipose tissue has been described as characteristic [2,3,4,5]. A significant number of SCPLs may exhibit a “low-fat” or “fat-free” appearance on imaging that can mimic more aggressive tumors such as myxoid and pleomorphic liposarcomas or non-adipocytic sarcomas [5]. The purpose of this study is to increase the understanding of this tumor family’s imaging and clinical features by combining our institutional data with all previously published case series.
Materials and methods
Institutional review
Case selection and demographic analysis
A waiver of informed consent was obtained from the institutional review board for this HIPAA-compliant retrospective study. The institutional pathology database was queried to identify all histologically proven cases in the SCPL spectrum between January 2010 and March 2017. The search query included the terms “spindle cell lipoma,” “pleomorphic lipoma” and “cellular angiofibroma.” Cases were excluded if there was neither a detailed outside MRI report describing the characteristics of the mass nor preoperative CT or MR images available for review. The pathology and operative reports were also reviewed, and age and gender were recorded. A pathologic diagnosis was made by one of two experienced pathologists sub-specialized in soft tissue and bone. All cases included were those that fit into the classical histologic description of the SCPL spectrum and did not demonstrate atypia.
Imaging analysis
A single musculoskeletal (MSK) fellowship-trained radiologist (ADS, 6 years of experience) reviewed all available MRI and CT imaging and radiology reports. In an effort to simplify data acquisition and reduce the risk of bias, the majority of items were categorized in a binary fashion (Table 1). Percentage of fatty composition was determined subjectively by density with CT images and by a combination of T1-weighted and fat-suppressed fluid-sensitive pulse sequences. Tumors were analyzed for heterogeneity, the presence of septations or solid/nodular tissue, enhancement patterns and T2 signal intensity. The location of the mass was determined to be subcutaneous or deep to the muscle fascia by means of imaging and reports. If both CT and MRI images were available for the same lesion, the mass was only counted once.
Combined data review
Search method
A Boolean search of PubMed was performed on 15 April 2017 for the following diagnostic entities: “spindle cell lipoma,” “pleomorphic lipoma,” “cellular angiofibroma” AND “MRI” OR “radiology.” Studies included were those with at least three reported cases of masses on the SCPL spectrum and a description of imaging and demographic information. Case reports were therefore excluded. References within included articles were also reviewed for additional studies suitable for inclusion. The papers were reviewed for data regarding mass location, MR characteristics, patient age and gender. Attempts were made to categorize MRI data from these studies in a manner similar to that of the institutional review. For example, differences in reporting of fatty grading were noted between authors, but the 75% threshold allowed for relatively uniform classification of masses across the studies.
Results
Institutional data
Demographics
A total of 42 cases were identified including 34 spindle cell lipomas, 7 pleomorphic lipomas and 1 cellular angiofibroma. There was a mean age of 57.4 (median age 57; range 23–87 years), and males accounted for 79% of cases. Masses were distributed throughout the body, but 52% of masses were located in the neck, back or shoulder regions (Fig. 1). The neck and back region accounted for 26% of cases. Twenty cases were located in the extremities and other locations.

Frequency of SCPLs by anatomic location in the body for the institutional case series
Imaging findings
Thirty-seven cases had MR images or detailed imaging reports from outside MRIs (Table 2). Among those, 16 had outside MRI reports only, 2 of which had CT images available for review that confirmed findings regarding tissue composition and enhancement patterns described on the outside MRI reports. Intravenous contrast agents were administered in 26 cases (combined MR and CT data for contrast descriptions). Among the five cases without MR images/reports, all were neck masses with CT images. Twenty-four masses were subcutaneous (57%), and 18 were deep (43%).
When all available data were combined (excluding 2 reports with missing data), 40% of tumors were comprised of < 75% fat. Among the masses with CT scans only, 60% were composed of more than 75% fat (Fig. 2). Among those with available MR images, 57% were composed of more than 75% fat (Fig. 3). When combined with detailed outside MR reports, 57% were composed of more than 75% fat, 38% with less than 75% fat (Fig. 4), and 5% had reports that were not specific enough to reliably determine the fat composition. When CT and MR images and reports were combined, 57% were composed of more than 75% fat, 38% with less than 75% fat and 5% with a fat composition that could not be determined (Table 3).

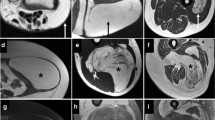
A 65-year-old male with SCPL spectrum mass in the neck region with a circular region of interest drawn showing a mean attenuation value of −99 HU, consistent with fat. The fat does not appear simple, and there are several mildly thickened septations, but the mass is composed of more than 75% fat

A 65-year-old male with SCPL spectrum mass in the shoulder region with more than 75% of the mass following signal intensity consistent with macroscopic fat (short white arrows) as seen on the proton density fat-suppressed image (left panel) and T1 (right panel). There are also linear and slightly nodular, non-fatty regions at the periphery of the mass (long gray arrows)

A 65-year-old male with SCPL spectrum mass in the thigh (lower extremity) with less than 75% fat. This deep thigh mass demonstrates predominantly non-fatty signal (long gray arrows) on the T1 image (left panel) and predominantly T2 hyperintensity on the T2 fat-suppressed image (right panel). There are tiny foci of macroscopic fat (small white arrows)
Areas of increased T2 signal (not following fat signal) were commonly seen in the form of hyperintense septations or soft tissue (33/37) (Fig. 5). Among these cases, one report did not sufficiently detail T2 signal characteristics to enable analysis. Only three cases lacked T2 hyperintense regions. Contrast enhancement was also commonly seen (24/26 contrast-enhanced studies). Septal enhancement alone was seen in 9/26 cases. Solid enhancement was seen in 16/26 cases (Fig. 6). There was overlap between septal and solid enhancements in some of these masses. Among the MR images, masses were usually heterogeneous (34/37, Fig. 7). Only three were homogeneous in that they lacked soft tissue, non-fatty areas or many septations.

A 54-year-old male with SCPL spectrum mass in the shoulder region with more than 75% fat (when scanning through the rest of the mass), but there are areas of linear low and amorphous low T1 (left panel, gray arrow) and high T2FS signal (right panel, gray arrow)

An 87-year-old male with a deep pelvic SCPL spectrum mass without discernible fat demonstrates avid solid contrast enhancement (gray arrows) between the T1 fat-suppressed pre-contrast (left panel) and post-contrast (right panel) images

A 44-year-old male with SCPL spectrum mass around the knee (lower extremity) with heterogeneous appearance on T1 image. There is a large area of the mass composed of T1 isointense signal (relative to muscle, long gray arrow) and a smaller more cranial area of tissue isointense to fat (small white arrow)
Combined data
A total of four studies meeting the inclusion criteria were identified [2,3,4,5]. When combined with the institutional data, there were 91 SCPL spectrum masses including 74 with MRI data and 54 that were contrast enhanced (Table 4). Among the masses that had reliable descriptions of fatty composition (2 cases were excluded from the 37 institutional cases as described above), 37/72 (51%) were composed of less than 75% fat. T2 hyperintense regions were seen in 64/73 (86%) cases. Among those with sufficient data regarding the presence of septations (46 total), septations were seen in 28 masses. Sixty-two of 74 (84%) masses were heterogeneous, and 27% of masses were deep. Allowing for limitations of missing anatomic location data (14 of 19 accounted for in Khashper’s study and lumping the neck, shoulder and back together in Kirwadi’s study), 56/86 (65%) of masses occurred in the neck, back or shoulder region, 26% occurred in the upper or lower extremities, and 9% occurred elsewhere. Ninety-one percent of masses demonstrated some degree of contrast enhancement, and masses occurred in male patients in 82% of cases. At excision, the mean age from each study was 58 (range 54–65) although when including individual age extremes from all four studies the range extended from 23 to 87.
Discussion
Investigators have advocated for using ancillary cytogenetic testing in problematic cases when traditional macroscopic imaging and standard histologic assessment are insufficient [11]. As the role of ancillary cytogenetic testing has become increasingly important in these tumors’ classification, it has become apparent that imaging characteristics such as fat composition, size, nodularity and septations may be inadequate to accurately distinguish between ALT/WDLs from simple lipomas and lipoma variants [1, 10]. Moreover, recent pathologic studies have suggested a re-characterization of macroscopic fat-containing soft tissue masses to include a group of spindle cell lipomatous tumors with atypia. Fletcher and colleagues reported that this group of tumors lacks MDM2 and CDK4 amplification typical of ALT/WDL, and 57% had a loss of Rb as is often seen in the traditional SCPL spectrum [12]. However, this is a heterogeneous group of tumors, and the reported differential diagnosis includes spindle cell lipoma, diffuse neurofibroma, mammary-type myofibroblastoma, dermatofibrosarcoma protuberans, fat-forming solitary fibrous tumor and morphologically low-grade malignant peripheral nerve sheath tumor [12]. Similarly, Weiss and colleagues described a category of lipotamous tumors that were genetically different from those on the SCPL spectrum and the ALT/WDL as a fibrosarcoma-like lipomatous neoplasm [13]. Like in Fletcher’s study, in this series, these tumors also did not show metastatic potential. Therefore, it is plausible that there may be overlap between tumors types in Weiss and Fletcher’s studies. As further genetic studies continue to expand the knowledge about macroscopic fat-containing tumors, it is becoming increasingly clear that the imaging differential diagnosis of lipoma versus liposarcoma is a gross oversimplification. Currently, the World Health Organization has not formally recognized the group of tumors proposed by Fletcher or Weiss [14]. Therefore, the current study only focuses on those meeting the classical histologic criteria for the SCPL spectrum.
Prior studies have suggested substantial overlap of imaging features between tumors of the SCPL spectrum and ALT/WDLs (and other tumors) [10]. There is also overlap between these two categories in terms of patient demographics. While male gender, older age, lower extremity and deep location have been associated with an increased probability of an ALT/WDL, this study shows that SCPLs also occur in these patients and in these locations. Although there is a predilection for the head, neck and shoulder region and a superficial location, in our institutional series, these tumors occurred in other locations in 48% of cases and in locations deep to the subcutaneous plane in 43% of cases. When data from all studies are combined, 27% of cases were deep and 35% presented in locations other than the neck, back or shoulders. This finding contrasts with previous teachings on the subject and the statement in the 2013 World Health Organization blue book [14] on soft tissue tumors, which indicates that SCPLs in the lower extremity are “distinctly rare.”
Given the significant overlap between the SCPL spectrum and the ALT/WLD, it seems reasonable to assume that MR imaging features and patient demographics may not be sufficient to differentiate these two tumors. This differentiation is important as the tumors of the SCPL spectrum will be resected and have no significant probability of recurrence or metastasis, while ALT/WDL can recur locally and requires ongoing surveillance [10, 15, 16]. However, Fletcher reports a 13% rate of recurrence among tumors grouped as atypical spindle cell lipomatous tumors [12]. The authors propose that the differential diagnosis of a fat-containing mass with features atypical for a simple lipoma include ALT/WDL and the SCPL spectrum tumors as their overlap is significant, and reliable differentiation by imaging and demographics alone is challenging. Moreover, it is reasonable to include the possibility of other low-grade spindle cell lipomatous tumors in the differential diagnosis as these lesions become further classified. In ambiguous cases, cytogenetic testing of resection specimen will become important.
Even more important is whether cross-sectional imaging and patient demographics can help differentiate “low-fat” and “fat-free” SCPLs from more aggressive liposarcoma subtypes and non-adipocytic sarcomas. While marginal excisions may be acceptable for ALT/WDLs and SCPLs, a wide excision would be preferred for more aggressive sarcomas [10]. Future studies into the ability to accurately differentiate among SCPLs, ALT/WDL and more aggressive sarcomas by means of cross-sectional imaging and patient demographics are needed.
This study has several weaknesses. First, although the institutional series has a larger number of cases than any previous study, data from a significant number of cases were only based on outside reports (16/37). However, the authors excluded any cases when report descriptions were missing or ambiguous. Use of binary descriptors also helped to remove some of the potential subjectivity in the assessment of images and reports. Second, review of previously published case series also does not allow for direct imaging assessment and instead relies on the descriptions provided by the authors. However, using a binary description system and a 75% cutoff for fat composition allowed for a relative uniformity of categorizations of masses between the different studies. The 75% cutoff for fat composition was also selected as a composition below this point was associated with a significantly increased (p < 0.001) probability of an ALT/WDL in a previous landmark study [1]. Next, tumor prevalence should be taken into account when trying to determine whether a mass with features atypical for a lipoma is encountered at cross-sectional imaging. Though the true prevalence of tumors of the SCPL spectrum is not known, in a study of 301 fatty tumor resections, 17% were of the SCPL spectrum, 47% were simple lipomas, and 36% were ALT/WDLs [11]. If this represents the true prevalence, it could be reasonable to assume that fatty masses with atypical features are more likely to represent ALT/WDLs than SCPLs. However, a subanalysis comparing all atypical features between ALT/WDLs and SCPLs was not performed. Finally, a description of the cytogenetics of each mass is not included in the other case series for each mass. In the institutional case series, cytogenetic descriptions of the masses were also not included in every case. Standard histology techniques are often sufficient to make the correct diagnosis, but when in question, the pathologist will then rely on ancillary cytogenetic tests [17].
In summary, this is the largest case series to date describing the imaging and demographic data associated with masses of the classical SCPL spectrum. Moreover, an additional analysis was performed to combine all available data from previous case series. The results of these analyses indicate that although there is a predilection for these masses to occur in older male patients and in the head, neck and shoulder region, these masses can occur in other locations, in a wide age range and in female patients. While prior studies have indicated that most are subcutaneous, a significant proportion of these masses will be deep to the muscle fascia plane. More importantly, masses of the SCPL spectrum frequently are associated with cross-sectional imaging features atypical for a simple lipoma, and when considering an ALT/WDL in the imaging differential diagnosis, tumors of the SCPL spectrum should also be included. As the categorization of atypical spindle cell lipomatous tumors expands in the pathology literature, it will be important to determine the ability to reliably differentiate these tumors by macroscopic imaging. Ultimately, biopsy with ancillary testing may be necessary.
References
Kransdorf MJ, Bancroft LW, Peterson JJ, Murphey MD, Foster WC, Temple HT. Imaging of fatty tumors: distinction of lipoma and well-differentiated liposarcoma. Radiology. 2002;224(1):99–104.
Choi JW, Kim HJ, Kim J, Kim HJ, Cha JH, Kim ST. Spindle cell lipoma of the head and neck: CT and MR imaging findings. Neuroradiology. 2013;55(1):101–6.
Kirwadi A, Abdul-Halim R, Fernando M, Highland A, Kotnis N. MR imaging features of spindle cell lipoma. Skelet Radiol. 2014;43(2):191–6.
Bancroft L, Kransdorf MJ, Peterson JJ, Sundaram M, Murphey MD, O'Connor MI. Imaging characteristics of spindle cell lipoma. AJR Am J Roentgenol. 2003;181(5):1251–4.
Khashper A, Zheng J, Nahal A, Discepola F. Imaging characteristics of spindle cell lipoma and its variants. Skelet Radiol. 2014;43(5):591–7.
Panagopoulos I, Gorunova L, Bjerkehagen B, Andersen K, Lund-Iversen M, Heim S. Loss of chromosome 13 material in cellular angiofibromas indicates pathogenetic similarity with spindle cell lipomas. Diagn Pathol. 2017;12(1):17.
Ntorkou AA, Tsili AC, Giannakis D, Batistatou A, Stavrou S, Sofikitis N, et al. Magnetic resonance imaging findings of cellular angiofibroma of the tunica vaginalis of the testis: a case report. J Med Case Rep. 2016;10:71.
Shintaku M, Naitou M, Nakashima Y. Angiomyofibroblastoma-like tumor (lipomatous variant) of the inguinal region of a male patient. Pathol Int. 2002;52(9):619–22.
Brisson M, Kashima T, Delaney D, Tirabosco R, Clarke A, Cro S, et al. MRI characteristics of lipoma and atypical lipomatous tumor/well-differentiated liposarcoma: retrospective comparison with histology and MDM2 gene amplification. Skelet Radiol. 2013;42(5):635–47.
Rizer M, Singer AD, Edgar M, Jose J, Subhawong TK. The histological variants of liposarcoma: predictive MRI findings with prognostic implications, management, follow-up, and differential diagnosis. Skelet Radiol. 2016;45(9):1193–204.
Clay MR, Martinez AP, Weiss SW, Edgar MA. MDM2 amplification in problematic Lipomatous tumors: analysis of FISH testing criteria. Am J Surg Pathol. 2015;39(10):1433–9.
Mariño-Enriquez A, Nascimento AF, Ligon AH, Liang C, Fletcher CD. Atypical spindle cell Lipomatous tumor: Clinicopathologic characterization of 232 cases demonstrating a morphologic Spectrum. Am J Surg Pathol. 2017;41(2):234–44.
Deyrup AT, Chibon F, Guillou L, Lagarde P, Coindre JM, Weiss SW. Fibrosarcoma-like lipomatous neoplasm: a reappraisal of so-called spindle cell liposarcoma defining a unique lipomatous tumor unrelated to other liposarcomas. Am J Surg Pathol. 2013;37(9):1373–8.
Fletcher CDM, Bridge JA, Hogendoorn PCW, Mertens F. WHO classification of tumours of soft tissue and bone. Pathology and genetics of tumours of soft tissue and bone. 4th ed. Lyon: IARC Press; 2013.
Weiss SW, Rao VK. Well-differentiated liposarcoma (atypical lipoma) of deep soft tissue of the extremities, retroperitoneum, and miscellaneous sites. A follow-up study of 92 cases with analysis of the incidence of “dedifferentiation”. Am J Surg Pathol. 1992;16(11):1051–8.
Lucas DR, Nascimento AG, Sanjay BK, Rock MG. Well-differentiated liposarcoma. The Mayo Clinic experience with 58 cases. Am J Clin Pathol. 1994;102(5):677–83.
Zhang H, Erickson-Johnson M, Wang X, Oliveira JL, Nascimento AG, et al. Molecular testing for lipomatous tumors: critical analysis and test recommendations based on the analysis of 405 extremity-based tumors. Am J Surg Pathol. 2010;34(9):1304–11.
Author information
Authors and Affiliations
Contributions
Guarantors of the integrity of the entire study, all authors; study concepts/study design or data acquisition or data analysis/interpretation, Y.Y., A.M., M.E., M.U., F.G., T.K.S, A.D.S.; manuscript drafting or manuscript revision for important intellectual content, all authors; approval of final version of submitted manuscript, all authors; agree to ensure any questions related to the work are appropriately resolved, all authors; literature research, Y.Y., A.M., M.E., A.D.S.; clinical studies, N.R., M.E., A.M., M.U.; statistical analysis, Y.Y., T.K.S, A.D.S.; manuscript editing, all authors.
Corresponding author
Ethics declarations
Disclosures
The authors have no relevant conflicts to disclose.
Consent
Approved by the IRB with waiver of informed consent.
Rights and permissions
About this article

Cite this article
Younan, Y., Martinez, A., Reimer, N. et al. Combined classical spindle cell/pleomorphic lipoma spectrum imaging and clinical data. Skeletal Radiol 47, 51–59 (2018). https://doi.org/10.1007/s00256-017-2751-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-017-2751-1