
Abstract
Objective
Parameniscal cysts have a very high association with meniscal tears in all locations except the anterior horn lateral meniscus (AHLM). The common insertion of the anterior cruciate ligament (ACL) and the AHLM root may provide a pathway for disease. The purpose of our study was to determine if cysts of the ACL are the origin of cysts adjacent to the AHLM.
Materials and methods
Radiology reports of all magnetic resonance (MR) examinations of the knee over a 7-year period were searched for “cyst”, “ganglion”, and “ganglia”. Two fellowship-trained musculoskeletal radiologists independently reviewed those MR examinations reported to have a possible cyst of the AHLM and/or the ACL. The study group consisted of those patients with a cyst located adjacent to the AHLM but no meniscal tear of the adjacent meniscus. The ACL in each of these patients was evaluated for the presence of a cyst. Comparison with age- and gender-matched controls was performed.
Results
Of 708 cases that contained the word “cyst”, “ganglion”, or “ganglia”, 121 reports indicated a possible cyst of the ACL or AHLM. Twelve individuals had a cyst located adjacent to the AHLM with no meniscal tear. Six (50%) of these individuals had a cyst of the ACL; no ACL cysts were identified in the control group (p = 0.014). Interreader agreement for AHLM parameniscal cysts and AHLM tears was substantial.
Conclusions
Our results suggest that cysts adjacent to the AHLM may in part be explained by cysts or ganglia of the ACL.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Parameniscal cysts have been thoroughly described in the literature as having a very high association with meniscal tears [1–4]. The causes of parameniscal cysts is debated, however the predominant theory suggests it is the result of fluid decompression through an articular surface meniscal tear [1, 3–7]. Although this explains the association of parameniscal cysts with meniscal tears, it does not explain the formation of cysts in all meniscal locations.
Cysts adjacent to the anterior horn lateral meniscus (AHLM) lack the strong association with meniscal tears common to other parameniscal cystic lesions [8]. Investigators have hypothesized on the etiology of parameniscal fluid adjacent to the AHLM. De Smet suggested that fluid tracking centrally along the course of the transverse meniscal ligament may be the result of capsular penetration at the junction of the ligament and AHLM [8]. Some have hypothesized that ganglia adjacent to the AHLM may result from degeneration of the transverse meniscal ligament [9]. Still others query that parameniscal cysts may be the result of cystic degeneration of the meniscus decompressing into the adjacent soft tissues [10, 11]. To date, the origin of these cystic lesions remains unknown.
Our anecdotal experience suggests a possible relationship between cysts of the ACL and cysts of the AHLM. A unique feature to the AHLM root attachment is its intimate association with the tibial insertion of the anterior cruciate ligament (ACL) [12]. Ganglion cysts of the ACL are known to distend the ligamentous fibers as well as track outside of the cruciate ligament, specifically near its tibial insertion [13]. We hypothesize ACL cysts or ganglia may lead to the development of AHLM parameniscal cysts.
Materials and methods
This was an IRB-approved retrospective study in which patient consent was waived. A retrospective search of all magnetic resonance (MR) imaging reports of the knee from March 2007 to February 2014 was conducted. Search terms included “cyst”, “ganglia”, or “ganglion”. Two fellowship-trained musculoskeletal radiologists independently reviewed those MR examinations reported to have a possible cyst of the AHLM and/or the ACL (EE, RW). The study group consisted of those patients with a cyst located adjacent to the AHLM but no meniscal tear of the adjacent meniscus. Those patients with prior knee surgery or imaging performed at field strengths less than 1.5 Tesla were excluded.
An age- and gender-matched control group was selected by a continuous review of MR examinations beginning February 2014 in a reverse chronological order to November 2013. Each case was individually matched in this time period with a study case of the same gender and ±2 years of age with the exception of one case that had a 4-year difference in age. Similar technical parameters were used for the study and control group during the different time periods.
MR imaging
All knee MR examinations were performed on either a 3-T clinical scanner (Signa Excite, GE Healthcare) or a 1.5-T clinical scanner (Espree, Siemens Healthcare; Genesis Signa or Signa HDxt, GE Healthcare). Each examination utilized a dedicated knee coil with the patient’s knee placed in a neutral position.
Fat-suppressed fast spin-echo (FSE) T2-weighted images were obtained in the axial, coronal, or sagittal planes in all patients. Proton density images were also obtained in the sagittal plane. The TR range/TE range was 1,110-6,300/11-52, and the echo train length was between 1 and 13. The slice thickness ranged between 3 and 4 mm with an interslice gap of 1 mm. The number of excitations was either 1 or 2 and a flip angle of 90 degrees was used. A 16-cm field of view was utilized for all sequences with matrix size ranges of 256–640 × 216–640.
Image interpretation
All MR knee exams reported to have a possible cyst of the ACL or AHLM were independently reviewed by two fellowship-trained musculoskeletal radiologists (EE, RW) with 2 and 15 years of experience, respectively. An AHLM parameniscal cyst was defined as a high T2 signal mass with a track to the margin of the meniscus or being directly adjacent to the AHLM (Figs. 1, 2 and 3). The anterior horn was defined by dividing the lateral meniscus into thirds on the axial view as defined by De Smet (Fig. 1) [8]. The most medial extent of the AHLM was considered to terminate at the most lateral insertion of the ACL. All joint recesses and completely intrameniscal cysts were excluded. An ACL cyst was defined as fluid signal on T2-weighted sequences within the substance of the ligament with indistinctness of the normal ligamentous striation but not necessarily significant expansion of the overall ligament (Figs. 1, 2, and 3). An AHLM tear was defined as increased linear signal within the meniscus extending to an articular surface on one or more slices or abnormal meniscal morphology. Although the “two-slice-touch” rule has a higher positive predictive value for the diagnosis of a meniscal tear than a single-slice-touch, the goal of the study was to be as sensitive as possible for identifying AHLM tears [14]. The control group was selected by a third fellowship-trained musculoskeletal radiologist (KM) with 3 years of clinical experience. The inclusion criteria for the control patients were the same as the study group however with no parameniscal cyst or tear of the AHLM (Fig. 4).

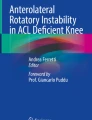
A 16-year-old male with knee pain. a, b Axial and coronal T2-weighted FSE fat-saturated images demonstrate an ACL cyst (white arrows). c Axial image demonstrates the demarcation of the meniscus into thirds, anterior horn, body, and posterior horn (dashed white line). c, d Axial and sagittal T2-weighted FSE fat-saturated images demonstrate a parameniscal cyst adjacent to the anterior horn of the lateral meniscus but no meniscal tear (dashed white arrows)

A 65-year-old male with knee pain. a, b Axial and coronal T2-weighted FSE fat-saturated images demonstrate an ACL cyst (white arrows). c, d Axial and sagittal T2-weighted FSE fat-saturated images demonstrate a parameniscal cyst adjacent to the anterior horn of the lateral meniscus but no meniscal tear (dashed white arrows)

A 20-year-old male collegiate football player with concern for a medial collateral ligament injury. a, b Coronal and axial T2-weighted fat-saturated images demonstrate an ACL cyst (white arrows). c, d Axial and sagittal T2-weighted fat-saturated images demonstrate a parameniscal cyst (dashed white arrows)

A 34-year-old male who is part of our control group. a, b Coronal and axial T2-weighted fat-saturated images demonstrate a normal ACL (white arrows). c, d Axial and sagittal T2-weighted fat-saturated images demonstrate a normal AHLM with no parameniscal cyst (dashed white arrows)
Statistical analysis
Categorical variables of AHLM parameniscal cyst were assessed for their association with an ACL cyst using Fisher’s exact test. Kappa values were calculated to determine interreader agreement from individual data for AHLM parameniscal cysts and tears. All p values were obtained using two-sided tests of significance and a p value <0.05 was considered statistically significant. Statistical analysis was performed by using software (SPSS Version 22.0. IBM Corp., Armonk, NY, USA).
Results
Of 708 reports that matched “cyst”, “ganglia”, or “ganglion”, 122 suggested a possible AHLM parameniscal cyst and/or an ACL cyst (55 suggested a possible AHLM parameniscal cysts, 57 suggested a possible ACL cyst, and ten possibly suggested possibly both). Twelve individuals (eight men, four women; age range, 16–65 years; mean, 40 years) had a cyst located adjacent to the AHLM with no meniscal tear. The control group consisted of 12 patients individually matched (eight men, four women; age range, 16–61; mean, 40 years) with a normal AHLM and no parameniscal cyst (Table 1). Six (50%) individuals in the study group had a cyst of the ACL; no ACL cysts were identified in the control group (p = 0.014). Interreader agreement was substantial for both AHLM parameniscal cysts (κ = .64, p < 0.001, 95 % CI [0.48, 0.80]) and AHLM tears (κ = .725, p < 0.001, 95 % CI [0.592, 0.858]. There was independent interreader agreement for the presence or absence of an ACL cyst in all study patients with the exception of two individuals in which consensus was required.
Discussion
Our retrospective review has shown that when a parameniscal cyst is seen without evidence of a meniscal tear, there is a strong association (50%) with cysts within the ACL. De Smet reported a positive association of parameniscal cysts with AHLM tears in only 64% of cases; therefore, another theory of parameniscal cyst formation other than meniscal tears needs to be considered to account for this discrepancy.
We hypothesize that in addition to AHLM tears, the ACL is another source for parameniscal cyst formation. The AHLM root inserts adjacent to and parallel to the anterior half of the ACL footprint [12]. This intimate association could serve as a pathway for cystic migration. An association between cruciate ligament pathology and intrameniscal and parameniscal cysts has already been suggested. A recent article by McMonagle notes an increased incidence of parameniscal cysts in those patients with PCL mucoid degeneration [15]. Additionally, a recent abstract by Tafur et al. concluded that there was a significant association between ACL pathology and AHLM root ligament abnormalities [16].
Our study supports the hypothesis that a different mechanism of parameniscal cyst formation may be fluid from an ACL cyst dissecting through the common insertion with the AHLM. Similar to parameniscal cysts, ACL cysts are referred to in the literature under different monikers, which include “mucinous degeneration of the ACL,” “mucoid degeneration of the ACL,” and “ACL ganglia” [17, 18]. Some studies have attempted to differentiate a “cyst” and “mucinous degeneration” through MRI criteria, but Bergin concluded that, “anterior cruciate ligament ganglia” may be part of a degenerative process and that these two entities may represent different manifestations of this continuum” [18]. These two entities are also not readily discernable at arthroscopy; for these reasons, we elected not to make a distinction between these two conditions and to term these lesions as ACL cysts [18].
For our study, we defined an ACL cyst as fluid signal on T2-weighted sequences within the substance of the ligament and indistinctness of the normal ligamentous striation. This criteria is similar to a prior MR study that sought to define both ACL ganglia and mucinous degeneration with histologic correlation [18]. Other criteria in the literature for diagnosing ACL ganglia include significant mass effect on the anterior cruciate ligament fibers, but we suspect that cysts may at least partially decompress through the common insertion with the AHLM and therefore would not necessarily have as significant of mass effect on the ligament [18].
Cysts of the cruciate ligaments are rare entities with a prevalence of 0.29–0.9% [17, 19]. Clinically, these may be asymptomatic but can also cause pain, sensations of fullness during motion, joint line tenderness, and limited range of motion [20]. Secondary findings of ACL cysts include intraosseous ganglion formation, predominantly at the tibial insertion [20, 21]. McLauren postulated that stresses at the cruciate ligament insertions may result in focal necrosis of the bone that then liquefies and forms an intraosseous ganglion [19]. However, similar to our proposed mechanism of AHLM parameniscal cyst formation, McLauren also suggested that intraosseous ganglia arise as extensions from parosteal ganglia that can migrate along a ligament toward insertion sites [19].
There were several limitations to this study. We could not blind the reviewers to the presence or absence of an ACL cyst. This may have introduced bias into our study results. This was a retrospective study with a small study group; the results of a larger study may differ from our results. A search for ACL cysts and ganglia in addition to AHLM cyst may have introduced selection bias into our study, however we believe this was justified for several reasons. Cysts adjacent to the AHLM are exceedingly rare with a prevalence of only 0.21% [8]. In addition, we suspected many smaller cysts near the AHLM were not mentioned in the radiology reports. Therefore, a retrospective review of parameniscal cysts alone would have identified too few patients for a viable study. Our anecdotal experience of a relationship between ACL cysts and AHLM parameniscal cysts drove the decision to conduct the study as we did.
Although our findings support an association between ACL cysts and AHLM parameniscal cysts, this association does not imply causality. However, the intimate association of the ACL and AHLM root insertion would provide a pathway of disease. It is our hope that future studies with a larger study group may be able to confirm our hypothesis.
In conclusion, there is a significant association between ACL cysts and AHLM parameniscal cysts. We suggest an alternate etiology for the formation of AHLM parameniscal cysts from ACL cysts dissecting along the common insertion with the root attachment of the AHLM. This may partially explain the source of parameniscal cysts in this location.
References
Schuldt DR, Wolfe RD. Clinical and arthographic findings in meniscal cysts. Radiology. 1980;134:49–52.
Tasker AD, Ostlere SJ. Relative incidence and morphology of lateral and medial meniscal cysts detected by magnetic resonance imaging. Clin Radiol. 1995;50:778–81.
Parisien JS. Arthroscopic treatment of cysts of the menisci. a preliminary report. Clin Orthop Relat Res. 1990;257:154–8.
Campbell SE, Sanders TG, Morrison WB. MR imaging of meniscal cysts: incidence, location, and clinical significance. AJR. 2001;177:409–13.
Barrie HJ. The pathogenesis and significance of meniscal cysts. J Bone Joint Surg (Br). 1979;61-B(2):184–9.
Howe TS, Koh JS. Arthoscopic internal marsupialization of meniscal cysts. Knee. 2007;14(5):408–10.
Anderson JJ, Connor GF, Helms CA. New observations on meniscal cysts. Skeletal Radiol. 2010;39:1187–91.
De Smet AA, Graf BK, del Rio MA. Association of parameniscal cysts with underlying meniscal tears as identified on MRI and arthroscopy. AJR. 2011;196:180–6.
Saddik D, McNally EG, Richardson M. MRI of Hoffa’s fat pad. Skeletal Radiol. 2004;33:433–44.
Pedowitz RA, Feagin JA, Rajagopalan S. A surgical algorithm for treatment of cystic degeneration of the meniscus. Arthroscopy. 1996;12:209–12.
Lantz B, Singer KM. Meniscal cysts. Clin Sports Med. 1990;9:707–25.
Johnson DL, Swenson TM, Livesay GA, et al. Insertion-site anatomy of the human menisci: gross, arthroscopic, and topographical anatomy as a basis for meniscal transplantation. Arthroscopy. 1995;11(4):386–94.
Krudwig WK, Schulte KK, Heinemann C. Intra-articular ganglion cysts of the knee joint: a report of 85 cases and review of the literature. Knee Surg Sports Traumatol Arthrosc. 2004;12:123–9.
De Smet AA, Tuite MJ. Use of the “two-slice-touch” rule for the MRI diagnosis of meniscal tears. AJR. 2006;187:911–4.
McMonagle JS, Helms CA, Garrett WE, Vinson EN. Tram-track appearance of the posterior cruciate ligament (PCL): correlations with mucoid degeneration, ligamentous stability, and differentiation from PCL tears. AJR. 2013;201:394–9.
Tafur M, Cunha GM, Choi JY et al. Association of ACL and Anterior Horn Lateral Meniscus Root Ligament Anatomy and Pathology: 11.7 T MRI Anatomic Study with Retrospective Review of 500 Knee MRIs. Poster session presented at: International Skeletal Society; 2013 Sep 30; Philadelphia, PA.
Huang GS, Lee CH, Chan WP, et al. Ganglion cysts of the cruciate ligaments. Acta Radiol. 2002;43(4):419–24.
Bergin D, Morrison WB, Carrino JA, Nallamshetty SN, Bartolozzi AR. Anterior cruciate ligament ganglia and mucoid degeneration: coexistence and clinical correlation. AJR. 2004;182:1283–7.
McLaren DB, Buckwalter KA, Vahey TN. The prevalence and significance of cyst-like changes at the cruciate ligament attachments in the knee. Skeletal Radiol. 1992;21:365.
Kim MG, Kim BH, Choi JA, et al. Intra-articular ganglion cysts of the knee: clinical and MR imaging features. Eur Radiol. 2001;11:834–40.
Recht MP, Applegate G, Kaplan P. The MR appearance of cruciate ganglion cysts. a report of 16 cases. Skeletal Radiol. 1994;23:597.
Conflict of interest
The authors have no financial interests to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
England, E., Wissman, R.D., Mehta, K. et al. Cysts of the anterior horn lateral meniscus and the ACL: is there a relationship?. Skeletal Radiol 44, 369–373 (2015). https://doi.org/10.1007/s00256-014-2043-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-014-2043-y