
Abstract
The infrapatellar fat pad of Hoffa is commonly injured but rarely discussed in the radiological literature. Abnormalities within it most commonly are the consequences of trauma and degeneration, but inflammatory and neoplastic diseases of the synovium can be confined to the fat pad. The commonest traumatic lesions follow arthroscopy, but intrinsic signal abnormalities can also be due to posterior and superior impingements syndromes and following patellar dislocation. Infrapatellar plica syndrome may also be traumatic in aetiology. The precise aetiology of ganglion cysts is not understood; the principal differential diagnosis is a meniscal or cruciate cyst. Hoffa’s fat pad contains residual synovial tissue, meaning that primary neoplastic conditions of synovium may originate and be confined to the fat pad. Inflammatory changes along the posterior border of the pad may also be used to help differentiate effusion from acute synovitis on unenhanced MR examinations.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Anatomy and variations
Hoffa’s fat pad is an intracapsular, but extrasynovial structure (Fig. 1). Anteriorly, it is limited by the patella tendon. Its posterior boundary is the (synovial-lined) knee joint. Posteriorly, it projects into the intercondylar notch via two alar synovial folds, which fuse forming the infrapatellar plica. Superiorly, the fat pad attaches to the inferior surface of the patella, and superoposteriorly it extends to the cartilage overlying the anterior aspect of the distal femur. Inferiorly, it is attached to the periosteum of the tibia and the anterior horns of the menisci [1, 2] and it abuts the deep infrapatellar bursa (Fig. 2). A fatty apron extends from the fat pad to partially divide the infrapatellar bursa into anterior and posterior compartments [3]. The fat pad is a flexible, displaceable structure (as evident during arthroscopy) which may increase the synovial area and facilitate the distribution of lubricant in the joint. The volume of the fat pad varies considerably among individuals and is lost only in extreme emaciation. This does not begin to occur until the subcutaneous fat is eliminated, and its preservation under these circumstances has enhanced the belief that the volume of the fat pad is important to knee function [4].

Sagittal T1-weighted sequence demonstrating the boundaries of the predominantly T1 hyperintense Hoffa’s fat pad. Low-signal foci seen within represent fibrous septa

Deep infrapatellar bursitis. Note the intimate relationship to the inferior aspect of the fat pad (arrow)
The fat pad is structurally similar to subcutaneous tissue in that it contains a framework of fibrous cords interspersed among adipose tissue [5] (Fig. 1). In addition there are a number of larger condensations which represent named structures. The aforementioned infrapatellar plica, also known as the ligamentum mucosum, runs from its posterior attachment on the intercondylar notch of the femur [2, 6] (Fig. 3), anteriorly through the fat pad and may even reach the inferior pole of the patella [7]. It is commonly visualised on arthroscopy but rarely identified on MR imaging [8]. This may reflect unfamiliarity with this structure [8], but also because this thin structure is difficult to separate from the anterior cruciate ligament which follows a parallel course. Running in a perpendicular plane to the infrapatellar plica, the anterior intermeniscal ligament traverses the fat pad apex between the anterior horns of both menisci.

Infrapatellar plica. Sagittal T2-weighted image (with fat saturation) showing a normal plica inserting into the apex of the fat pad (arrow)
The vascular supply of Hoffa’s fat pad is an anastomotic network, which is derived from vertically orientated vessels arising from the superior and inferior genicular arteries. These vertical vessels are interconnected by horizontal arteries. Whilst the peripheral aspect of Hoffa’s fat pad is well supplied (Fig. 4), there is a paucity of vascularity in the centre, which is of relevance in determining the choice of arthroscopic portals [9]. Hoffa’s fat pad receives branches of the femoral, common peroneal and saphenous nerves. It is a richly innervated structure containing Type IVa free nerve endings which transmit pain and inflammation and are therefore a source of anterior knee pain [10].

Sagittal T2-weighted image with fat saturation. Note the large vessel in the lateral aspect of the fat pad (arrow)
On MR imaging the fat pad may demonstrate two clefts, one vertical and one horizontal [1, 11, 12]. These are readily identified in the presence of an effusion or other pathology. The vertical cleft lies in the superior aspect of the fat pad (Fig. 5).The horizontal cleft is found in the posterior-inferior aspect of the fat pad, just below the insertion of the infrapatellar plica. Its prevalence has been variously reported as between 14% and 90%; however, this is dependent on the definition of cleft used. If any linear abnormality is considered, the prevalence is high, as these represent the normal alar folds. Frank fluid-filled, globular defects occur in approximately 10–14% of patients [5, 12] (Fig. 6). It has been suggested that variability of the embryological regression process of the infrapatellar membrane into the infrapatellar plica may account for the horizontal cleft [5]. The horizontal cleft is much more commonly seen than the vertical cleft. Both clefts are synovial-lined and may communicate with one another and the synovial cavity of the knee joint [11, 12] (Fig. 7). Given their synovial lining it is not surprising, therefore, that synovial-based pathology may occur de novo within Hoffa’s fat pad and not always represent an extension from the synovial-lined knee joint.

Sagittal T1-weighted sequence with fat saturation following intra-articular gadolinium injection. Note the vertical cleft (arrow)

Sagittal T1-weighted sequence with fat saturation following intra-articular gadolinium injection. Arrow indicates the horizontal cleft

Sagittal gradient echo sequence showing communication between the vertical and horizontal clefts
Hoffa’s ganglion
Fluid-filled globular clefts need to be distinguished from ganglia and other cysts that can occur in the posterior aspect of the fat pad. Ganglia are common fluid-filled lesions that are most often located adjacent to the anterior horn of the lateral meniscus [13] (Fig. 8). The reason for this predilection is unknown [13, 14] but we suggest that they may originate from degeneration of the intertransverse ligament. It has also been speculated that the pathogenesis may relate to a compressive injury to the meniscal periphery and resultant degenerative change extending into the soft tissue rather than into the meniscus [15, 16].In common with ganglia elsewhere, a communication with the joint is not readily seen on MR imaging and they have no synovial lining. They may be uni- or multilocular [17]. In a review of 1,767 cases of patients referred for MR imaging of the knee, 23 had intra-articular ganglia, three of which were identified within the fat pad; two were palpable [18]. The authors’ experience would suggest that Hoffa’s ganglia are more common than reported in this study, so regional variations may exist. Ganglia can leak or rupture producing ill-defined oedema in the fat pad.

Sagittal gradient echo image demonstrates a ganglion cyst intimately related to the anterior horn of the lateral meniscus
On MR imaging, ganglion cysts demonstrate hypo- or isointensity on T1-weighted images and hyperintensity relative to skeletal muscle on T2-weighted images. The differentiation between fluid in the horizontal cleft and a ganglion is not usually difficult as a fluid-filled cleft has a large posterior defect where there is clear communication with a knee effusion with which it is usually associated. Parameniscal cysts are usually secondary to a horizontal (or complex tear) of the meniscus with resultant escape of fluid into the parameniscal tissues. They may extend anteriorly into Hoffa’s fat pad [17] (Figs. 9, 10). Pathologically, meniscal cysts and ganglion cysts both contain fluid with high protein content that is similar to synovial fluid [19, 20]. Meniscal cysts are differentiated from ganglion cysts on MR imaging in that the former are associated with a tear, whilst the latter are not. The differentiation is important as it can influence treatment. Whilst both may need cyst drainage or excision, the presence of a tear frequently requires partial meniscectomy [15, 19]. In addition, in the absence of a tear, ganglion cysts may not be appreciated at arthroscopy and may require an extra-articular rather than an arthroscopic approach for decompression [21].

A 9-year-old with lateral knee pain. A meniscal cyst (large arrow) extending into the fat pad arising from a tear of the lateral discoid meniscus is seen on sequential images (not shown)

Sagittal T2-weighted image with fat saturation. This patient had a tear of both the posterior horn and body of the lateral meniscus. Oedema is seen in the fat pad adjacent to the torn meniscus
Trauma
Hoffa’s fat pad can be traumatised during acute injury following a variety of different mechanisms. Major ligamentous injury, injury to the patellar tendon and in particular anterior cruciate ligament (ACL) injury with anterior displacement of the stump can all involve Hoffa’s fat pad [22]. This review will focus more on the differential diagnosis of post-traumatic changes that are confined to the fat pad, in particular following patellar dislocation, post-arthroscopy or by repetitive impingement. Impingement takes two forms: the more common is impingement of the apex of the fat pad against the lateral femoral condyle, the better known is posterior or Hoffa’s impingement syndrome.
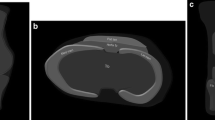
Changes in the fat pad have been noted as an indirect sign of occult traumatic patellar dislocation. In a study of 18 patients with this condition, all were found on MR imaging to have changes in the fat pad. These changes included signal alteration, (extra-anatomical) cleft formation and fragmentation. In all patients the superior border (at the attachment to the inferior pole of the patella) demonstrated signal change (particularly in the medial half of the fat pad) (Fig. 11) [23]. On MR imaging, it can be difficult to differentiate fragmented fat from loose intra-articular bodies, and plain films and CT may be required [23].

Axial T2-weighted image with fat saturation in a patient with a history of transient patellar subluxation. Note the oedema in the fat pad (long arrow) and a trabecular microfracture in the lateral femoral condyle (short arrow)
Fat pad impingement and infrapatellar plica syndromes
Inflammatory changes within Hoffa’s fat pad take three main forms. The most commonly described is Hoffa’s disease. Hoffa’s disease (also known as a syndrome of infrapatellar fat pad impingement) is a condition described by Albert Hoffa in 1904, in which acute trauma or repetitive microtrauma to the fat pad causes haemorrhage and inflammation. The trauma may take the form of repetitive hyperextension or rotational strain [24]. The fat pad hypertrophies and becomes impinged between the femur and tibia (Fig. 12). This results in further inflammation, and fibrin and haemosiderin are deposited with macrophage infiltration and degenerate lipocytes noted. In the chronic phase a fibroblastic cell response occurs which replaces the fibrocytes and causes fibrosis. This can transform to fibrocartilaginous tissue and rarely may undergo ossification [1, 24, 25, 26, 27].

Hoffa’s disease in a 25-year-old gym instructor with anterior knee pain. Clinically the fat pad felt enlarged and was tender. Sagittal T2-weighted image with fat saturation demonstrates an enlarged oedematous fat pad
Clinically, in the acute phase (corresponding histologically to haemorrhage and oedema), anterior knee pain and loss of motion may be the presenting symptoms. On physical examination, the fat pad may be prominent, tender and firm, and “Hoffa’s sign” may be elicited [26, 27]. This sign refers to a test whereby the patient is supine and their knee and hip are flexed at a 90° angle. The medial and lateral borders of the patella tendon are then palpated whilst pressure is placed on the fat pad and pain results [28]. In the chronic phase (corresponding histologically to fibroblasts and scar tissue), anterior knee pain is believed to be due to impingement of fibrous tissue on the articular cartilage, on the soft tissue capsule or both [25, 27].
The precise relationship of Hoffa’s impingement and infrapatellar plica syndrome is unclear and the two may be difficult to differentiate on clinical and imaging criteria. As mentioned in the anatomical section above, the infrapatellar plica may be identified on MR imaging. It runs a course from its femoral origin parallel and anterior to the ACL towards the anterior intermeniscal ligament. From there it turns to run through Hoffa’s fat pad towards the inferior pole of the patella. If oedema or fibrotic thickening within the fat pad follows this pattern (Fig. 13) then infrapatellar plica syndrome may be a preferred diagnosis over Hoffa’s impingement. More diffuse and widespread abnormalities involving the posterior aspect of the fat pad would favour a diagnosis of Hoffa’s impingement. It is likely that there is some overlap and oedema at the apex (intercondylar notch) of the fat pad, close to the insertion of the infrapatellar plica, may be secondary to inflammatory change within the plica (Fig. 14) or due to early impingement. This is currently a subject of investigation (correlating MR and arthroscopic findings) at one of our institutions. We are unaware of any particular injury which may predispose to one or other entity though an increasing recognition of these separate phenomenon may improve their clinical differentiation in the future.

A 50-year-old with anterior knee pain. A Sagittal proton density image and B sagittal T2-weighted image with fat saturation. Arrows indicate a presumed thickened oedematous infrapatellar plica which traverses the fat pad

A 43-year-old with a medial meniscal tear (not shown). Sequential sagittal T2 images with fat saturation. A Arrow points to a thickened infrapatellar plica. B Arrow indicates oedema in the apex of the fat pad. C Arthroscopic image. This demonstrates the thickened plica (long arrow) and oedema in the apex of the fat pad (short arrow)
A third condition is impingement of the superolateral aspect of the fat pad, which is more common though less often reported as the changes can be rather subtle. When present, increased signal on T2-weighted or preferably fat-saturated images are noted in the superolateral aspect of the fat pad. The typical case is associated with a laterally lying extensor mechanism, loss of the normal fat plane between the patellar tendon and the lateral femoral condyle and patella alta (Figs. 15, 16) [29]. The oedema can extend into the central superior aspect of the fat pad. As the oedematous fat blends with high signal from the adjacent femoral condyle, the normal three bands of tissue (from anterior to posterior: patellar tendon, Hoffa’s fat, femoral condylar cartilage) become two (patellar tendon and oedematous fat blending with high-signal cartilage). An association with patellar maltracking is postulated, with impingement occurring between the lateral aspect of the patellar tendon and the lateral femoral condyle. Although increasingly recognised, it is more common but less reported than the classic variant described by Hoffa, and is frequently overlooked and underreported in several radiology texts [1, 17, 19, 29, 30].

Sagittal T2-weighted image with fat saturation demonstrates oedema in the superolateral aspect of the fat pad (arrow adjacent to the patellar tendon

A 20-year-old patient with anterior knee pain. Sagittal T2-weighted image with fat saturation shows oedema in the superolateral aspect of the fat pad (short arrow), patellar tendinosis (thin arrow) and subchondral marrow oedema related to chondromalacia patellae
More significantly, more needs to be done to establish the clinical importance of these entities to ensure that they are not simply radiological diagnoses. In a study in which one of the authors was an awake patient, bilateral arthroscopies revealed that the fat pad was exquisitely sensitive [31]. The clinical importance of the fat pad was examined in a retrospective review of 53 patients by Duri et al. These patients were all felt to have pain originating within the fat pad from a variety of causes including extensor mechanism disease, meniscal surgery or cruciate surgery. Clinical features including pain and stiffness responded, albeit transiently, to an injection into the fat pad of local anaesthetic and steroid. The authors concluded that, if not correctly treated, pain produced by the fat pad may impair knee joint function [24]. Though guided injection therapy and arthroscopic resection of fat have been reported to reduce symptoms, there are no systematic outcome studies in either type of Hoffa’s impingement. In the authors’ experience direct compression of these areas of inflammation does not always reproduce symptoms; therefore, clinical correlation is important in their assessment and many are not the cause of patient’s symptoms.
Postoperative changes
Postoperative changes affecting the fat pad can be divided into three groups: postsurgical fibrosis, post-arthroscopic fibrosis and the “cyclops” lesion seen in ACL reconstruction. Post-surgical fibrosis can be seen in the post-patellectomy patient (Fig. 17). It is usually ill defined or confluent. Post-arthroscopic fibrosis usually manifests as discrete bands coursing horizontally through the fat pad (Fig. 18). The portals used that traverse the fat pad are the anterolateral, anteromedial and central portals [1]. (The posterior aspect of the fat pad may also be shaved to aid entry into the joint.) The fibrosis tends to be accentuated at the portal. In one study the fibrous scar occurred and peaked within 6 months of arthroscopy. It then reduced and by 18 months post-arthroscopy had disappeared in nearly half the patients [32]. Metallic fragments can also be identified in the fat pad and are particularly prominent on gradient-echo imaging due to susceptibility artefact, where their resemblance to a division sign (÷) aids the differential diagnosis from loose bodies.

Post-patellectomy. Sagittal gradient echo image shows diffuse (low signal) scarring in the fat pad (arrow)

Sagittal proton density image. Post-arthroscopy discrete area of scarring (arrow)
Prior to ACL reconstruction, an ACL stump may be seen in the fat pad apex (Fig. 19). The cyclops lesion seen in ACL reconstruction is a nodular soft tissue mass which extends into the intercondylar region and apex of the infrapatellar fat pad. It typically manifests as loss of full knee extension. The origin of this lesion is not well understood but a reaction to exposed ACL graft material, from the residual ACL stump, infrapatellar fat pad metaplasia or intercondylar fibrosis, have all been postulated [33, 34, 35, 36]. Histologically, the cyclops lesion may contain fibrous tissue, fibrocartilage, bone, synovium and fat from the infrapatellar fat pad. In view of this, the term “anterior metaplasia” has been used to describe the various contributions to the cyclops lesion [33]. On MR imaging it demonstrates T2 hypointensity (Fig. 20) consistent with its fibrous nature. MR imaging is sensitive, specific and accurate in diagnosing this condition [33]. Given that this condition does not respond to physical therapy, MR imaging is useful in triaging these patients to surgery.

Ruptured anterior cruciate ligament. Residual ligament is sited in the apex of the fat pad (arrow). A Sagittal proton density and B axial proton density images

Cyclops lesion following anterior cruciate ligament reconstruction. Sagittal T2-weighted image. Note the predominant T2 hypointense mass in the apex of the fat pad (arrow)
Synovial abnormalities
As previously mentioned, the clefts within Hoffa’s fat pad have a synovial lining. It is not surprising, therefore, that synovial-based pathology may occur de novo within Hoffa’s fat pad and does not always represent an extension from the synovial-lined knee joint. A synovitis and its associated joint effusion can be associated with focal or diffuse oedema of the fat pad. As a joint effusion can obscure a synovial proliferative disorder, the appearances of the fat pad can be helpful in distinguishing those patients who have a proliferative effusion from those who do not [17, 37]. Defects and displacement of the fat pad were shown to have a sensitivity of 57% and a specificity of 99% for identifying a synovial proliferative from a non-proliferative disorder [37] (Fig. 21). The differential diagnosis of a solid, non-cystic mass within the fat pad is between pigmented villonodular synovitis (PVNS), synovial osteochondromatosis, synovial haemangioma, extraskeletal chondroma and gouty tophus. Glomus tumour [38] and fibroma of the tendon sheath of the fat pad [39] have been described in Hoffa’s fat pad but are rare.

Rheumatoid arthritis. Sagittal T1-weighted image with fat saturation following intravenous gadolinium injection demonstrates scalloping of the inferior aspect of the fat pad
Primary (idiopathic) synovial osteochondromatosis is a condition characterised by synovial metaplasia with resultant intrasynovial cartilaginous formation [15, 40, 41, 42]. Calcified loose bodies are hypointense on T1- and T2-weighted imaging, both centrally and peripherally. Ossified bodies, in comparison, have a centre that is hyperintense on T1-weighted imaging (follows marrow) and a periphery that is hypointense on T1-weighted imaging (cortical margin).
Extraskeletal chondroma is a benign cartilaginous soft tissue tumour that is uncommon and rarely involves the fat pad. Histologically, it usually consists of mature hyaline cartilage and may have foci of calcification, fibrosis and metaplastic ossification within it [43]. Metaplastic ossification is also evident in end-stage Hoffa’s disease. In view of this, it has been postulated that extraskeletal chondroma and end-stage Hoffa’s disease are the same entity [25]. Cartilage and other solid masses may be difficult to differentiate from synovial fluid. Intravenous gadolinium may have a role in this setting [21, 44] (Fig. 22).

Proven case of synovial osteochondromatosis. A Sagittal T1-weighted and B sagittal gradient echo images. Note the confluent involvement of the fat pad and a discrete low-signal body associated with it (arrows)
Synovial haemangioma is a rare benign vascular soft tissue tumour which frequently involves the knee [40, 41, 45, 46] and may be focal. The prefemoral fat pad is more frequently involved than Hoffa’s fat pad [21, 45] and a careful search for extension to this area can help make the differentiation. Radiographs are an insensitive means of making this diagnosis, particularly in view of the fact that phleboliths are rare unless there is extra-articular extension [41, 47, 48]. MR imaging demonstrates T1-weighted signal hypo- or isointense to muscle, and there is frequently a lobulated margin which should suggest this condition. A useful differential feature is the presence of enlargement and abundance of surrounding vessels[41, 49] (Fig. 23).

Synovial haemangioma in an 11-year-old patient who initially presented with anterior knee pain and a haemarthrosis and later re-presented with locking. A Sagittal T1-weighted and B sagittal T2-weighted images demonstrate a diffuse process both involving the fat pad and extending into the suprapatellar pouch. Note among the areas of confluent T2 hyperintensity the more discrete foci of T2 hypointensity consistent with vessels and fibrofatty septa (arrows). C Sagittal gradient echo image illustrating the locked knee which occurred at the second presentation
PVNS is a condition characterised histologically by proliferation of synovial cells (resulting in a villonodular appearance), and hyperplasia of lipid-laden or haemosiderin-laden macrophages as well as multinucleated giant cells [40, 50]. The disease may also be diffuse or focal and, when focal, Hoffa’s fat pad is a common location. On MR imaging it manifests as a low signal mass on T2-weighted imaging (Fig. 24) which, when present, should prompt a careful search elsewhere in the joint for further evidence of synovial involvement. T2-weighted signal hypointensity is also dependent on the proportion of fat and fibrovascular elements present and may not always be low. Signal intensity is usually low to intermediate on T1-weighted images. The presence of haemosiderin becomes more obvious on high field strength and gradient-echo images due to susceptibility artefact manifesting as greater signal drop-out [51, 52]. This is of importance in the postsurgical follow-up of this condition as metallic artefact can mimic haemosiderin deposition. Fast spin-echo imaging is useful to decrease this artefact [41, 51]. Low-signal material within Hoffa’s fat pad has also to be distinguished from synovial haemangioma, haemophilia, synovial osteochondromatosis, rheumatoid arthritis, gout and amyloidosis.

Pigmented villonodular synovitis. A Sagittal T1-weighted sequence showing a hypointense mass in the fat pad (arrow). B Axial T2-weighted sequence showing a hypointense mass in the fat pad (long arrow). Effusion surrounds it. A Baker’s cyst is present (short arrow)
References
Jacobson JA, Lenchik L, Ruhoy MK, Schweitzer ME, Resnick D. MR imaging of the infrapatellar fat pad of Hoffa. Radiographics 1997; 17:675–691.
Williams P, Warwick R, Dyson M, et al. Gray’s anatomy, 37th edn. New York: Churchill Livingstone, 1989.
La Prade RF. The anatomy of the deep infrapatellar bursa of the knee. Am J Sports Med 1998; 26:129–132.
Smillie IS. Disease of the knee joint, 1st edn. London: Churchill Livingstone, 1974.
Vahlensieck M, Linneborn G, Schild H, Schmidt HM. Hoffa’s recess: incidence, morphology and differential diagnosis of the globular-shaped cleft in the infrapatellar fat pad of the knee on MRI and cadaver dissections. Eur Radiol 2002; 12:90–93.
Dupont JY. Synovial plicae of the knee. Controversies and review. Clin Sports Med. 1997; 16:87–122.
Kim SJ, Min BH, Kim HK. Arthroscopic anatomy of the infrapatellar plica. Arthroscopy 1996; 12:561–564.
Kosarek FJ, Helms CA. The MR appearance of the infrapatellar plica. AJR Am J Roentgenol 1999; 172:481–484.
Kohn D, Deiler S, Rudert M. Arterial blood supply of the infrapatellar fat pad. Anatomy and clinical consequences. Arch Orthop Trauma Surg 1995; 114:72–75.
Biedert RM, Sanchis-Alfonso V. Sources of anterior knee pain. Clin Sports Med 2002; 21:335–347.
Schweitzer ME, Falk A, Berthoty D, Mitchell M, Resnick D. Knee effusion: normal distribution of fluid. AJR Am J Roentgenol 1992; 159:361–363.
Patel SJ, Kaplan PA, Dussault RG, Kahler DM. Anatomy and clinical significance of the horizontal cleft in the infrapatellar fat pad of the knee. MR imaging. AJR Am J Roentgenol 1998; 170:1551–1555.
Kim MG, Kim BH, Choi JA, Lee NJ, Chung KB, Choi YS, Cho SB, Lim HC. Intra-articular ganglion cysts of the knee: clinical and MR features. Eur Radiol 2001; 11:834–840.
Stabler A, Glaser C, Reiser M. Musculoskeletal MR: knee. Eur Radiol 2000; 10:230–241.
Pedowitz RA, Feagin JA, Rajagopalan S. A surgical algorithm for treatment of cystic degeneration of the meniscus. Arthroscopy 1996; 12:209–212.
Lantz B, Singer KM. Meniscal cysts. Clin Sports Med 1990; 9:707–725.
Stoller D. Magnetic resonance imaging in orthopedics and sports medicine, 2nd edn. Philadelphia: Lippincott-Raven, 1997.
Bui-Mansfield LT, Youngberg RA. Intraarticular ganglia of the knee: prevalence, presentation, etiology, and management. AJR Am J Roentgenol 1997; 168:123–127.
Resnick D, Kang HS. Internal derangement of joints, 1st edn. Pennsylvania: WB Saunders, 1997.
Parisien JS. Arthroscopic treatment of cysts of the menisci. A preliminary report. Clin Orthop 1990; 257:154–158.
Kaplan P, Helms C, Dussault R, et al. Musculoskeletal MRI, 1st edn. Pennsylvania: WB Saunders, 2001.
Guo-Shu H, Chian-Her L, Wing CP, Herng-Sheng L, Cheng-Yu C, Yu JS. Acute anterior cruciate ligament stump entrapment in anterior cruciate ligament tears: MR imaging appearance. Radiology 2002; 225:537–540.
Apostolaki E, Cassar-Pullicino VN, Tyrrell PN, McCall IW. MRI appearances of the infrapatellar fat pad in occult traumatic patellar dislocation. Clin Radiol 1999; 54:743–747.
Duri ZA, Aichroth PM, Dowd G. The fat pad. Clinical observations. Am J Knee Surg 1996; 9:55–66.
Krebs VE, Parker RD. Arthroscopic resection of an extrasynovial ossifying chondroma of the infrapatellar fat pad: end-stage Hoffa’s disease? Arthroscopy 1994; 10:301–304.
Hoffa A. Influence of adipose tissue with regard to the pathology of the knee joint. JAMA 1904; 43:795–796.
Magi M, Branca A, Bucca C, LangerameV. Hoffa disease. Ital J Orthop Traumatol 1991; 17:211–216.
Boomgarden C. Differential diagnosis for anterior knee pain. Strength Conditioning J 1999; 21:3.
Chung BC, Skaf A, Roger B, Campos J, Stump X, Resnick D. Patellar tendon–lateral femoral condyle friction syndrome: MR imaging in 42 patients. Skeletal Radiol 2001; 30:694–697.
Faletti C, De Stefano N, Giudice G, Larciprete M. Knee impingement syndromes. Eur J Radiol 1998; 27(Suppl 1):S60–69.
Dye SF, Vaupel GL, Dye CC. Conscious neurosensory mapping of the internal structures of the human knee without intra-articular anesthesia. Am J Sports Med 1998; 26:773–777.
Tang G, Niitsu M, Ikeda K, Endo H, Itai Y. Fibrous scar in the infrapatellar fat pad after arthroscopy: MR imaging. Radiat Med 2000; 18:1–5.
Bradley DM, Bergman AG, Dillingham MF. MR imaging of cyclops lesions. AJR Am J Roentgenol 2000; 174:719–726.
Jackson DW, Schaefer RK. Cyclops syndrome: loss of extension following intra-articular anterior cruciate ligament reconstruction. Arthroscopy 1990; 6:171–178.
Marzo JM, Bowen MK, Warren RF, Wickiewicz TL, Altchek DW. Intraarticular fibrous nodule as a cause of loss of extension following anterior cruciate ligament reconstruction. Arthroscopy 1992; 8:10–8.
Mariani PP, Ferretti A, Conteduca F, Tudisco C. Arthroscopic treatment of flexion deformity after ACL reconstruction. Arthroscopy 1992; 8:517–521.
Schweitzer ME, Falk A, Pathria M, Brahme S, Hodler J, Resnick D. MR imaging of the knee: can changes in the intracapsular fat pads be used as a sign of synovial proliferation in the presence of an effusion? AJR Am J Roentgenol 1993; 160:823–826.
Hardy P, Muller GP, Got C, Lortat-Jacob A, Benoit J. Glomus tumor of the fat pad. Arthroscopy 1998; 14:325–328.
Hur J, Damron TA, Vermont AI, Mathur SC. Fibroma of tendon sheath of the infrapatellar fat pad. Skeletal Radiol 1999; 28:407–410.
Dahnert W. Radiology review manual, 3rd edn. Baltimore: Williams and Wilkins, 1996.
Pomeranz SJ. Gamuts and pearls in orthopedics, 1st edn. Cincinnati: MRI-EFI Publications, 1997.
Narvaez JA, Narvaez J, Aguilera C, De Lama E, Portabella F. MR imaging of synovial tumors and tumor-like lesions. Eur Radiol 2001; 11:2549–2560.
Enzinger F, Weiss S. Soft tissue tumors, 3rd edn. Chicago: Mosby, 1995.
Kramer J, Recht M, Deely DM, Schweitzer M, Pathria MN, Gentili A, Greenway G, Resnick D. MR appearance of idiopathic synovial osteochondromatosis. [AUTHOR: PLEASE COMPLETE]
Resnick D. Bone and joint imaging, 2nd edn. Philadelphia: WB Saunders, 1996.
Devaney K, Vinh TN, Sweet DE. Synovial hemangioma: a report of 20 cases with differential diagnostic considerations. Hum Pathol 1993; 24:737–745.
Kamineni S, O’Driscoll SW, Morrey BF. Synovial osteochondromatosis of the elbow. J Bone Joint Surg Br 2002; 84:961–966.
Cotton A, Flipo RM, Herbaux B, Gougeon F, Lecomte-Houcke M, Chastanet P. Synovial haemangioma of the knee: a frequently misdiagnosed lesion. Skeletal Radiol 1995; 24:257–261.
Greenspan A, Azouz EM, Matthews J 2nd, Decarie JC. Synovial hemangioma: imaging features in eight histologically proven cases, review of the literature, and differential diagnosis. Skeletal Radiol 1995; 24:583–590..
Layfield L. Malignant giant cell tumor of synovium (malignant pigmented villonodular synovitis): a histopathologic and fluorescence in situ hybridisation analysis of 2 cases with review of the literature. Arch Pathol Lab Med 2000; 124:1636–1642.
Bravo SM, Winalski CS, Weissman B. Pigmented villonodular synovitis (review). Radiol Clin North Am 1996; 34:311–326.
Jelinek JS, Krasnsdorf MJ, Utz JA, Berrey BH Jr, Thomson JD, Heekin RD, Radowich MS. Imaging of pigmented villonodular synovitis with emphasis on MR imaging. AJR Am J Roentgenol 1989; 152:337–342.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Saddik, D., McNally, E.G. & Richardson, M. MRI of Hoffa’s fat pad. Skeletal Radiol 33, 433–444 (2004). https://doi.org/10.1007/s00256-003-0724-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-003-0724-z