
Abstract
Evaluating and managing children with suspected physical abuse is challenging. Few single injuries are pathognomonic for abuse and, as a result, child abuse is easily missed. As such, a healthy bit of skepticism is needed to recognize and protect abused children. The medical history and clinical presentation should guide evaluation. Medical providers must consider the differential diagnosis, epidemiology of injuries, and child development to inform the assessment. In this review, we address evidence-based recommendations to inform child physical abuse evaluations. We also discuss the role of medical providers in communicating with families, mandated reporting and interpreting medical information for investigative agencies and other non-medical colleagues entrusted with protecting children.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Child physical abuse represents a significant public health problem. Recent data from the National Child Abuse and Neglect Data System suggest there is an increasing number of victims of child abuse [1]. In 2018, an estimated 678,000 children were identified as victims of various forms of child maltreatment, more than 10% of whom were known victims of physical abuse; infants younger than 1 year represented nearly half of the 1,770 fatalities [1]. Diagnosing and managing child abuse is difficult and, for a variety of reasons, a diagnosis of child abuse can be missed. Many of the injuries identified in victims of abuse are nonspecific. Because of developmental capabilities, many children — including those younger than 1 year, who are at highest risk — cannot disclose their abuse. Perpetrators are infrequently honest about the events that occurred, and non-offending parents might look the other way, might also be victims of abuse, or might be unaware of the abuse. In many cases, the abuse is not witnessed. Additionally, solutions to child abuse are often elusive — families might struggle with many challenges, child protective services agencies frequently have high turnover, and there is little collaboration between health care professionals and investigative agencies. In the last decade, alternative theories of causation to child abuse have also been offered by physicians, rendering further challenges. Despite these difficulties, a careful evaluation coupled with open-minded skepticism and an evidence-based approach can assist medical providers in identifying and diagnosing children who are at risk.
Clinical evaluation
History
As with any medical evaluation, a comprehensive history is crucial to assessing children presenting with concerns for suspected child abuse. Key aspects of the history include the events leading to presentation, symptomatology and timing. Red flags in the history include lack of history of trauma in a child with clear injury, a changing history, delay in seeking care that is unexpected or unexplained, history incompatible with the child’s development, history that is incompatible with the injuries identified or different histories given by different caregivers [2].
A careful medical history should also be obtained to inform the differential diagnosis, including birth history with focus on gestational age; mode of delivery and need for neonatal intensive care; chronic medical problems that might predispose to injury; prior injury and surgical history; family history with close attention to history of bleeding, bone, genetic or metabolic disorders; medications; as well as a detailed developmental history [2]. A thorough psychosocial assessment to identify risk factors for abuse should also be performed, reviewing household composition, child care, employment status, stressors as well as history of mental health, substance use, intimate partner violence, law enforcement involvement and prior involvement with child protective services agencies [2].
Physical examination
A comprehensive physical examination provides important data in a child abuse evaluation. Anthropometrics including height, weight and head circumference, especially in young children, should be obtained. These measurements might alert physicians to concurrent child neglect. Head circumference can be informative in cases with possible intracranial injury. Providers should examine the head to look for signs of trauma such as scalp swelling or bulging fontanelle. The mouth should be assessed for injuries, especially to the frenula in young infants. Additionally, the skin should be examined thoroughly with attention to patterned injuries as well as areas of the body where bruising is uncommon, including the ears, neck, torso, genitalia and buttocks [2,3,4]. If possible, skin injuries should be measured and photo-documented using a forensic scale (such as the American Board of Forensic Odontology No. 2 scale) [5]. If a scale is not available, an object with a known measurement can be included in the photo-documentation to provide estimated measurement [2].
Laboratory evaluation
Evaluation for suspected child abuse often includes obtaining laboratory studies. Liver function tests, amylase and lipase can screen for occult intra-abdominal injury and assist with identifying the need for dedicated abdominal imaging such as CT of the abdomen and pelvis with intravenous contrast agent [6]. Additionally, history, clinical presentation and type of injuries can guide dedicated testing. For instance, the American Academy of Pediatrics provides recommendations for evaluating bleeding diatheses in children when there are concerns for suspected child abuse [7]. For children with bruising or intracranial hemorrhage, this evaluation should include complete blood cell count with platelet count, prothrombin time, activated partial thromboplastin time as well as more advanced bleeding evaluation including Factor VIII and Factor IX. For children with bruising, von Willebrand factor antigen and activity should be checked, whereas for children with intracranial hemorrhage, fibrinogen and D-dimer are recommended. Newborn screen should also be reviewed and, when indicated, additional testing for glutaric aciduria Type 1 should be considered for some children with intracranial hemorrhage [2]. For children presenting with fractures, laboratory studies to evaluate bone health are recommended, including calcium, phosphorus, alkaline phosphatase, parathyroid hormone and 25-hydroxy Vitamin D [8]. Toxicology testing should be performed in children presenting with altered mental status. Universal toxicology screening in asymptomatic children is controversial. Although patient screening can identify occult drug exposure and concerns for neglect, testing asymptomatic children represents environmental exposure and parental screening, raising civil liberties issues for parents [9].
Imaging
The child’s clinical presentation, physical examination, age, developmental capabilities as well as type and severity of injury should guide initial imaging [2]. Occult injury screening is a crucial component of evaluating young children for suspected physical abuse. The American Academy of Pediatrics, the Society for Pediatric Radiology and the American College of Radiology recommend that a skeletal survey be performed in children younger than 2 years when there are concerns for physical abuse, including infants with unexplained bruising or fractures, unexpected sudden death and unexplained intracranial injury [2, 10, 11]. Skeletal surveys have been shown to detect occult injuries in children evaluated for concerns for physical abuse in 11–34% of cases (Fig. 1) [12,13,14,15,16,17,18,19]. Skeletal surveys should follow the protocol recommended by the American College of Radiology [10, 20]. In children older than 2 years, a skeletal survey can be considered in certain clinical situations and dedicated plain radiography can be performed on areas of concern [10]. A follow-up skeletal survey approximately 2–3 weeks from initial skeletal survey is recommended in cases of suspected abuse in children younger than 2 years because it might identify additional injuries, clarify prior injuries, assist in dating an injury, and potentially change clinical impression (Fig. 2) [2, 10, 11, 21,22,23].

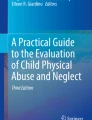
Oblique chest radiograph in an 8-month-old boy with abusive head trauma demonstrates multiple healing rib fractures (arrows)

Leg fractures in a 2-month-old girl with abusive head trauma. a Anteroposterior (AP) radiograph of the left knee demonstrates metaphyseal fractures of the distal femur and proximal tibia (arrows). b Follow-up AP radiograph of the left knee 2 weeks later demonstrates evidence of healing of these fractures with extensive periosteal reaction (arrows)
While there are varying perspectives on when to perform neuroimaging in asymptomatic children and with which imaging modality, neuroimaging should be considered as part of occult injury screening, especially in children younger than 1 year [10, 24,25,26,27]. Head CT without contrast agent should be used to evaluate symptomatic children with concerns for abusive head trauma, including those with neurologic abnormalities, facial injuries or fractures [2, 10, 28]. Advantages of unenhanced head CT include availability, rapidity of the study, especially for unstable patients, and sensitivity for detecting skull fractures and acute intracranial hemorrhage (Fig. 3) [2, 10, 11, 28, 29]. MRI should be considered to further evaluate injuries identified on initial head CT because it has been shown to provide new information in 25% of children (Fig. 3) [30]. MRI is also ideal for evaluating asymptomatic children with concerns for abuse [2, 10]. Note that while US can be performed in young infants for initial evaluation of macrocephaly, it is not appropriate for abuse evaluation.

Abusive head trauma in a 2-month-old girl. a Axial CT head image demonstrates bilateral hyperdense subdural hemorrhages both anteriorly overlying the right frontal lobe and along the occipital lobe posteriorly (solid black arrows). White arrows demonstrate left parietal bone fracture with overlying scalp edema. Dotted black arrow demonstrates left frontal lobe parenchymal cleft, evidence of parenchymal injury. b Axial MRI fluid-attenuated inversion recovery sequence confirms the bilateral subdural hemorrhages (arrows). c Three-dimensional CT viewed from the left posterior demonstrates the left parietal bone fracture (large arrow). It also identifies a fracture of the right parietal bone (small arrow)
Children with abusive head trauma have been found to have concomitant cervical spine injuries including cervical ligamentous injury as well as thoracolumbar subdural hemorrhage (Fig. 4) [31,32,33]. MRI of the cervical spine should be considered, especially when intracranial findings or multiple fractures have been identified. The utility of routine whole-spine imaging is unclear [10].

Abusive head trauma in a 2-month-old boy. a Sagittal MRI of the spine (sagittal short tau inversion recovery sequence) demonstrates edema in the region of the sub-occipital musculature including nuchal ligament (arrow), consistent with ligamentous injury. b Sagittal T1-W MR sequence demonstrates spinal subdural hemorrhage in the lumbar spinal canal (arrow)
Additional evaluation
Consultation with a child abuse pediatrician should be considered if available. For children presenting with intracranial injury, a thorough retinal examination should be performed using indirect ophthalmoscopy, preferably by an experienced pediatric ophthalmologist, and ideally within the first 24–72 h of presentation to evaluate for ocular trauma including retinal hemorrhages [34,35,36]. Further consultation from subspecialties such as hematology, endocrinology, genetics or others should be guided by clinical presentation and suspicion for medical causes of the injuries. Furthermore, past medical records relevant to the clinical presentation should be obtained. Communication with the primary care pediatrician is also helpful to obtain medical history and elicit any previous concerns, and can assist with follow-up needs.
Sibling evaluation
In general, siblings, including twins, other household children, and children who are cared for by the possible perpetrator should undergo age-appropriate screening and evaluation for child physical abuse [37,38,39]. This includes a thorough physical examination, a skeletal survey in children younger than 2 years, as well as consideration of neuroimaging based on clinical history and presentation [2].
Clinical pathways and decision tools
Although recommendations and guidelines have been developed by the American Academy of Pediatrics and experts on evaluation of suspected child abuse, adherence to these guidelines is variable [2, 40,41,42,43]. Several studies examining pathways and support tools have shown promise in addressing this concern. Use of a clinical decision support system at a tertiary-care children’s hospital emergency department in a randomized controlled trial that included a trigger system, alerts and an order set for physical abuse demonstrated acceptability by clinicians, and the ordered set resulted in 100% compliance with guidelines [44]. Implementation of a clinical guideline or algorithm was shown to reduce disparity in screening evaluation in other studies [45, 46]. A larger study examining association of skeletal survey performance and presence of a clinical pathway showed that the presence of a clinical pathway was associated with greater odds of obtaining a skeletal survey, though disparities still existed despite pathway presence [47]. With the evolution of electronic health records, these tools might help identify children at risk, ensure appropriate screening and reduce variation and disparity.
Challenges in diagnosis
Diagnosing child physical abuse is challenging and few single injuries are pathognomonic for child abuse. As such, medical providers must take careful consideration of all of the history gathered as well as the epidemiology of injuries and normal child development. Providers must also think through the differential diagnosis and consider medical conditions that can mimic child physical abuse.
Bruising
The differential diagnosis for bruising includes trauma, coagulopathies and other skin conditions. Bruising is rare in young infants and non-ambulatory children; bruising increases in an age-dependent manner concordant with a child’s development [4, 48]. Bruising typically occurs over bony prominences such as the shins and forehead in ambulatory children. The ears, neck, hands, buttocks and genitalia are rarely bruised [4]. Children who present with physical abuse often have more bruises than those who are not physically abused [49]. Additionally, they might have clusters of bruises or patterns of bruises such as the negative imprint of an object such as a hand or a looped wire or cord [2, 49]. Bruising in infants younger than 4 months or bruising of the torso, ears or neck in children younger than 4 years was shown to be predictive of abuse and, as such, bruising with these characteristics should raise concern for physical abuse [3].
Fractures
The majority of fractures in young children are the result of accidental trauma rather than physical abuse and it can be challenging to determine whether any single fracture is the result of inflicted injury [50]. Additional causes of fractures also must be considered in some cases, including birth trauma, genetic causes such as osteogenesis imperfecta, and metabolic bone disease such as osteopenia of prematurity or disuse. Careful consideration should be given to the type of fracture sustained and the mechanism of trauma provided as well as the child’s medical history. Certain fractures have been shown to be highly specific for abuse such as rib fractures, classic metaphyseal lesions, scapular fractures, sternal fractures and spinous process fractures [8, 51]. Physical abuse should be considered when infants and young children present with multiple fractures, rib fractures, fractures to infrequently injured bones, fractures in a non-ambulatory child without a history of trauma or underlying bone fragility, or fractures that are not well-explained by the history [2, 52].
Head trauma
As with other injuries, the clinical findings and history guide a diagnosis of abusive head trauma. Subdural hemorrhages are the most common finding in abusive head trauma [53]. Mechanisms of abusive head trauma are multifactorial and include shaking, impact or a combination of both [54]. The differential diagnosis for head trauma might include birth trauma, accidental trauma, abusive head trauma or medical conditions such as bleeding diatheses or glutaric aciduria Type 1. It is of note that while a history of accidental trauma such as a short fall should be considered, short falls rarely cause death in young children [55]. The child’s clinical presentation such as seizures, apnea, vomiting or increasing head circumference as well as other findings such as fractures, bruising or retinal hemorrhages might provide further clarity on the etiology of the injury. The presence and pattern of retinal hemorrhages in children can aid in diagnosis of abusive head trauma; retinal hemorrhages characterized as severe, too numerous to count, and as multi-layer retinal hemorrhages with or without retinoschisis are associated with child physical abuse [53, 56, 57]. Additionally, Maguire et al. [58] found that the presence of three or more of six characteristics (bruising, seizure, apnea, long bone fracture, retinal hemorrhage or rib fractures) was highly predictive of abusive head trauma. As such, when these characteristics are present, child physical abuse should be high on the differential diagnosis.
Addressing alternative theories
In recent years, a number of alternative theories to child abuse diagnoses have been proffered by a small group of physicians that are not grounded in sound data or research methodology. These include Ehlers–Danlos Type III to explain fractures in infants, dysphagic choking as an explanation for infant death, infant Vitamin D deficiency as a cause of subdural hemorrhage, and a rebuke of shaken baby as a cause of infant injury [59,60,61,62]. Often, these unproven and sometimes dishonest diagnoses are offered in legal hearings in both civil and criminal trials [63]. Physicians who care for children have a responsibility to work objectively, recognize legitimate areas of uncertainty, testify honestly, and stand up for science by challenging those who offer false diagnoses and unsupported theories in legal and medical settings.
Role of the medical provider
Medical providers play an essential role in multiple aspects of child abuse evaluations — from recognizing an injury, completing a thorough medical evaluation, and making a diagnosis to reporting and communicating with investigators. The first and foremost responsibility of medical providers is to ensure the child’s safety pending further medical evaluation. In some cases, especially young infants, this might require referral to an emergency department for further evaluation and treatment. Physicians are mandated reporters and as such must report any reasonable suspicion for child abuse or neglect to the appropriate child protective services agency and interpret medical information for investigators.
Communication with families
It is difficult to inform families that a report to a child protective services agency is warranted. Prior to communicating these concerns, providers should first ensure the safety of the child, the caregivers and the staff. For young infants, it is possible to discuss the concern for abuse in the presence of the child. For older children, it is more appropriate to discuss concerns for child maltreatment privately with the caregivers. When medical providers talk to families about concerns for child maltreatment, it is crucial to be open, honest and direct as well as non-judgmental. Physicians should focus the conversation on the need to ensure the child’s safety and well-being, without apportioning blame for the injury. Although families might be upset or angry, medical providers should remain calm and avoid confrontation. Emphasis should be placed on the fact that the caregivers and medical providers are unified in the goal of ensuring the best interests of the child. Once concerns are communicated, providers should be clear about recommendations and educate families on next steps.
Mandated reporting
In 1974, the first federal law addressing child maltreatment, the Child Abuse Prevention and Treatment Act (CAPTA), was enacted. Currently, CAPTA creates a minimum federal definition for child abuse. Every state creates its own definition of child abuse and neglect that expands on this federal definition [64]. Crimes related to child maltreatment are also determined by state laws. While reporting systems and mandated reporting laws vary by state, physicians are mandated reporters in every state. As mandated reporters, physicians are obligated to report a reasonable suspicion for child abuse or neglect; certainty of a diagnosis of abuse is not required. Reporting should be performed even if care is transferred to another medical provider. All states have some provisions for immunity for reporting in good faith, while failure to report can lead to criminal charges, medical licensing or malpractice issues, as well as continued risk to the child [2, 65].
Communication with investigative agencies
In addition to identifying and reporting concerns for child maltreatment, medical providers should communicate the medical facts and interpretation to investigators in accordance with their respective state laws. This can be challenging because investigators might be unfamiliar with medical terminology. Thus, clear documentation as well as communication is essential.
Outcomes of investigations
Child protective services agencies investigate cases of child abuse or neglect to determine whether a case meets the individual state definitions for child abuse or neglect. Child protective services are also responsible for the future protection of abused children and, therefore, are responsible for the ongoing safety and appropriate placement of the child during the abuse investigation. In some circumstances, services are placed in the home to support and help families. In other circumstances, children might be removed from the home and placed in kinship or foster care. Law enforcement investigations determine whether a crime was committed and who was responsible for committing the crime. In a law enforcement investigation, an alleged perpetrator might be charged with a crime. In cases of abuse, medical providers might be asked to provide expert opinion or documentation regarding concerns for maltreatment. Medical providers might also be subpoenaed to testify in court in criminal or civil trials. The American Academy of Pediatrics provides guidance on court testimony [66].
Summary
Medical providers play a key role in recognizing, evaluating, diagnosing and managing child physical abuse. While it is challenging, evidence-based guidelines exist to aid in assessment and providers should adhere to these recommendations as able. In addition to clinical management, open and honest communication with families as well as collaboration with non-medical professionals are vital to the ultimate protection of abused infants and children.
References
U.S. Department of Health and Human Services, Administration for Children and Families, Administration on Children et al (2020) Child maltreatment 2018. U.S. Department of Health and Human Services, Washington, DC
Christian CW, Committee on Child Abuse and Neglect, American Academy of Pediatrics (2015) The evaluation of suspected child physical abuse. Pediatrics 135:e1337–e1354
Pierce MC, Kaczor K, Aldridge S et al (2010) Bruising characteristics discriminating physical child abuse from accidental trauma. Pediatrics 125:67–74
Kemp AM, Dunstan F, Nuttall D et al (2015) Patterns of bruising in preschool children — a longitudinal study. Arch Dis Child 100:426–431
Hyzer WG, Krauss TC (1988) The bite mark standard reference scale — ABFO No. 2. J Forensic Sci 33:498–506
Lindberg D, Makoroff K, Harper N et al (2009) Utility of hepatic transaminases to recognize abuse in children. Pediatrics 124:509–516
Anderst JD, Carpenter SL, Abshire TC (2013) Evaluation for bleeding disorders in suspected child abuse. Pediatrics 131:e1314–e1322
Flaherty EG, Perez-Rossello JM, Levine MA, Hennrikus WL (2014) Evaluating children with fractures for child physical abuse. Pediatrics 133:e477–e489
Petska HW, Porada K, Nugent M et al (2019) Occult drug exposure in young children evaluated for physical abuse: an opportunity for intervention. Child Abuse Negl 88:412–419
Wootton-Gorges SL, Soares BP, Alazraki AL et al (2017) ACR appropriateness criteria: suspected physical abuse — child. J Am Coll Radiol 14:S338–s349
Section on Radiology, American Academy of Pediatrics (2009) Diagnostic imaging of child abuse. Pediatrics 123:1430–1435
Wood JN, Henry MK, Berger RP et al (2019) Use and utility of skeletal surveys to evaluate for occult fractures in young injured children. Acad Pediatr 19:428–437
Lindberg DM, Berger RP, Reynolds MS et al (2014) Yield of skeletal survey by age in children referred to abuse specialists. J Pediatr 164:1268–1273
Belfer RA, Klein BL, Orr L (2001) Use of the skeletal survey in the evaluation of child maltreatment. Am J Emerg Med 19:122–124
Duffy SO, Squires J, Fromkin JB, Berger RP (2011) Use of skeletal surveys to evaluate for physical abuse: analysis of 703 consecutive skeletal surveys. Pediatrics 127:e47–e52
Day F, Clegg S, McPhillips M, Mok J (2006) A retrospective case series of skeletal surveys in children with suspected non-accidental injury. J Clin Forensic Med 13:55–59
Merten DF, Radkowski MA, Leonidas JC (1983) The abused child: a radiological reappraisal. Radiology 146:377–381
Karmazyn B, Lewis ME, Jennings SG et al (2011) The prevalence of uncommon fractures on skeletal surveys performed to evaluate for suspected abuse in 930 children: should practice guidelines change? AJR Am J Roentgenol 197:W159–W163
Paine CW, Wood JN (2018) Skeletal surveys in young, injured children: a systematic review. Child Abuse Negl 76:237–249
American College of Radiology (2016) ACR–SPR practice parameter for the performance and interpretation of skeletal surveys in children. Online document. https://www.acr.org/-/media/ACR/Files/Practice-Parameters/Skeletal-Survey.pdf. Accessed 12 Oct 2020
Harper NS, Eddleman S, Lindberg DM (2013) The utility of follow-up skeletal surveys in child abuse. Pediatrics 131:e672–e678
Harper NS, Lewis T, Eddleman S, Lindberg DM (2016) Follow-up skeletal survey use by child abuse pediatricians. Child Abuse Negl 51:336–342
Zimmerman S, Makoroff K, Care M et al (2005) Utility of follow-up skeletal surveys in suspected child physical abuse evaluations. Child Abuse Negl 29:1075–1083
Fingarson A, Fortin K (2019) Yield of neuroimaging in infant physical abuse evaluations: do infant age and injury type matter? J Emerg Med 57:195–202
Wilson PM, Chua M, Care M et al (2014) Utility of head computed tomography in children with a single extremity fracture. J Pediatr 164:1274–1279
Rubin DM, Christian CW, Bilaniuk LT et al (2003) Occult head injury in high-risk abused children. Pediatrics 111:1382–1386
Laskey AL, Holsti M, Runyan DK, Socolar RR (2004) Occult head trauma in young suspected victims of physical abuse. J Pediatr 144:719–722
Hedlund GL, Frasier LD (2009) Neuroimaging of abusive head trauma. Forensic Sci Med Pathol 5:280–290
Prabhu SP, Newton AW, Perez-Rossello JM, Kleinman PK (2013) Three-dimensional skull models as a problem-solving tool in suspected child abuse. Pediatr Radiol 43:575–581
Kemp AM, Rajaram S, Mann M et al (2009) What neuroimaging should be performed in children in whom inflicted brain injury (iBI) is suspected? A systematic review. Clin Radiol 64:473–483
Kadom N, Khademian Z, Vezina G et al (2014) Usefulness of MRI detection of cervical spine and brain injuries in the evaluation of abusive head trauma. Pediatr Radiol 44:839–848
Choudhary AK, Ishak R, Zacharia TT, Dias MS (2014) Imaging of spinal injury in abusive head trauma: a retrospective study. Pediatr Radiol 44:1130–1140
Choudhary AK, Bradford RK, Dias MS et al (2012) Spinal subdural hemorrhage in abusive head trauma: a retrospective study. Radiology 262:216–223
Christian CW, Levin AV, Council on Child Abuse and Neglect et al (2018) The eye examination in the evaluation of child abuse. Pediatrics 142:e20181411
Levin AV (2010) Retinal hemorrhage in abusive head trauma. Pediatrics 126:961–970
Thackeray JD, Scribano PV, Lindberg DM (2010) Yield of retinal examination in suspected physical abuse with normal neuroimaging. Pediatrics 125:e1066–e1071
Campbell KA, Bogen DL, Berger RP (2006) The other children: a survey of child abuse physicians on the medical evaluation of children living with a physically abused child. Arch Pediatr Adolesc Med 160:1241–1246
Lindberg DM, Blood EA, Campbell KA et al (2013) Predictors of screening and injury in contacts of physically abused children. J Pediatr 163:730–735
Lindberg DM, Shapiro RA, Laskey AL et al (2012) Prevalence of abusive injuries in siblings and household contacts of physically abused children. Pediatrics 130:193–201
Wood JN, Fakeye O, Mondestin V et al (2015) Development of hospital-based guidelines for skeletal survey in young children with bruises. Pediatrics 135:e312–e320
Paine CW, Scribano PV, Localio R, Wood JN (2016) Development of guidelines for skeletal survey in young children with intracranial hemorrhage. Pediatrics 137:e20153024
Wood JN, Fakeye O, Feudtner C et al (2014) Development of guidelines for skeletal survey in young children with fractures. Pediatrics 134:45–53
Wood JN, Feudtner C, Medina SP et al (2012) Variation in occult injury screening for children with suspected abuse in selected US children's hospitals. Pediatrics 130:853–860
Suresh S, Saladino RA, Fromkin J et al (2018) Integration of physical abuse clinical decision support into the electronic health record at a tertiary care children’s hospital. J Am Med Inform Assoc 25:833–840
Higginbotham N, Lawson KA, Gettig K et al (2014) Utility of a child abuse screening guideline in an urban pediatric emergency department. J Trauma Acute Care Surg 76:871–877
Rangel EL, Cook BS, Bennett BL et al (2009) Eliminating disparity in evaluation for abuse in infants with head injury: use of a screening guideline. J Pediatr Surg 44:1229–1234
Stavas N, Paine C, Song L et al (2020) Impact of child abuse clinical pathways on skeletal survey performance in high-risk infants. Acad Pediatr 20:39–45
Sugar NF, Taylor JA, Feldman KW (1999) Bruises in infants and toddlers: those who don't cruise rarely bruise. Puget Sound Pediatric Research Network. Arch Pediatr Adolesc Med 153:399–403
Kemp AM, Maguire SA, Nuttall D et al (2014) Bruising in children who are assessed for suspected physical abuse. Arch Dis Childhood 99:108–113
Leventhal JM, Martin KD, Asnes AG (2008) Incidence of fractures attributable to abuse in young hospitalized children: results from analysis of a United States database. Pediatrics 122:599–604
Kleinman P (2015) Diagnostic imaging of child abuse. Cambridge University Press, Cambridge
Kemp AM, Dunstan F, Harrison S et al (2008) Patterns of skeletal fractures in child abuse: systematic review. BMJ 337:a1518
Vinchon M, de Foort-Dhellemmes S, Desurmont M, Delestret I (2010) Confessed abuse versus witnessed accidents in infants: comparison of clinical, radiological, and ophthalmological data in corroborated cases. Childs Nerv Syst 26:637–645
Choudhary AK, Servaes S, Slovis TL et al (2018) Consensus statement on abusive head trauma in infants and young children. Pediatr Radiol 48:1048–1065
Chadwick DL, Bertocci G, Castillo E et al (2008) Annual risk of death resulting from short falls among young children: less than 1 in 1 million. Pediatrics 121:1213–1224
Binenbaum G, Mirza-George N, Christian CW, Forbes BJ (2009) Odds of abuse associated with retinal hemorrhages in children suspected of child abuse. J AAPOS 13:268–272
Morad Y, Kim YM, Armstrong DC et al (2002) Correlation between retinal abnormalities and intracranial abnormalities in the shaken baby syndrome. Am J Ophthalmol 134:354–359
Maguire SA, Kemp AM, Lumb RC, Farewell DM (2011) Estimating the probability of abusive head trauma: a pooled analysis. Pediatrics 128:e550–e564
Holick MF, Hossein-Nezhad A, Tabatabaei F (2017) Multiple fractures in infants who have Ehlers-Danlos/hypermobility syndrome and or vitamin D deficiency: a case series of 72 infants whose parents were accused of child abuse and neglect. Dermatoendocrinol 9:e1279768
Barnes PD, Galaznik J, Gardner H, Shuman M (2010) Infant acute life-threatening event — dysphagic choking versus nonaccidental injury. Semin Pediatr Neurol 17:7–11
Squier W (2011) The “shaken baby” syndrome: pathology and mechanisms. Acta Neuropathol 122:519
Lynøe N, Elinder G, Hallberg B et al (2017) Insufficient evidence for ‘shaken baby syndrome’ — a systematic review. Acta Paediatr 106:1021–1027
Edwards GA (2015) Mimics of child abuse: can choking explain abusive head trauma? J Forensic Legal Med 35:33–37
Child Welfare Information Gateway (2019) About CAPTA: a legislative history. U.S. Department of Health & Human Services website. https://www.childwelfare.gov/pubs/factsheets/about/. Accessed 12 Oct 2020
Schilling S, Christian CW (2014) Child physical abuse and neglect. Child Adolesc Psychiatr Clin N Am 23:309–319
Paul SR, Narang SK (2017) Expert witness participation in civil and criminal proceedings. Pediatrics 139:e20163862
Acknowledgments
We thank Dr. Arabinda Choudhary for contributing radiology images for this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The Children’s Hospital of Philadelphia has received payment for Dr. Bennett’s expert testimony following subpoenas in cases of suspected child abuse. Dr. Christian provides expert medical-legal work in child abuse cases.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Bennett, C.E., Christian, C.W. Clinical evaluation and management of children with suspected physical abuse. Pediatr Radiol 51, 853–860 (2021). https://doi.org/10.1007/s00247-020-04864-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-020-04864-1