
Abstract
Children account for nearly half the population of Nigeria yet the capacity for effective imaging of children is unknown. In order to determine clinical resources for and challenges of paediatric radiology in Nigeria, certified radiologists at an exit examination in radiology for resident doctors, and resident doctors in radiology attending an update course, completed a semi-structured questionnaire detailing personal information, radiology training, practice and perceived priorities of paediatric radiology in Nigeria. Of 100 questionnaires, 80 were returned, completed (80%) by 46 (58%) certified radiologists, 14 (18%) senior and 20 (25%) junior radiology residents. Only 1 (2.2%) certified radiologist received dedicated albeit short training in paediatric radiology. Nine (20.0%) certified radiologists and 1 (2.9%) resident doctor target their practice to paediatric imaging. Only 2 (4.4%) certified radiologists devote at least half of their time to paediatric radiology. Forty-two (91%) of the certified radiologists are not aware of any radiologist primarily affiliated with a dedicated children’s hospital or who practices in a dedicated paediatric unit of a mixed hospital. Eight (19%) radiologists work in a facility with a consultant who has some training in paediatric radiology. Surgeons (64%), neonatologists (53%) and neurologists (45%) were the other paediatric specialties usually available where the respondent works. Fourteen (4.9%), 4 (2.1%), and 1 (1.3%) ultrasound, X-ray and magnetic resonance imaging (MRI) units, respectively, were reserved for paediatric imaging while no fluoroscopy or computed tomography (CT) unit was dedicated to children. Lack of dedicated equipment (44%) and trained paediatric radiologists (24%) were the main challenges to paediatric imaging as perceived by the respondents. Substantial deficits in human and material resources require informed investment in dedicated equipment and training to boost capacity for paediatric radiology in Nigeria.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Paediatric radiology is an emerging radiology subspecialty in Nigeria. Unlike the developed world with an aging population and sophisticated paediatric radiology practice, many developing nations have rapidly growing young populations but are nascent in paediatric radiology. About half of the estimated 193 million people in Nigeria, a typical developing nation, are younger than 14 years of age and the country has one of the highest population growth rates in the world with a projected population of 410 million people by 2050. In absolute terms, the under-15 population of Nigeria is more than 80 million children, which represents about 42% of all Nigerians, a number most likely understated given a high non-registration rate of children born in Nigeria [1, 2].
There are about 600 physicians dedicated to the medical and surgical care of children in Nigeria for a ready mix of consumers of paediatric radiology services [3, 4]. These services are provided by about 300 certified radiologists who are registered members of the Association of Radiologists in Nigeria supported by 12,545 radiographers represented by the Association of Radiographers of Nigeria. Nigeria has 35 university teaching hospitals, 20 tertiary-level federal medical centers, and many more public (including military) and private (including faith-based) hospitals with large paediatric wards where services are provided to children [5,6,7]. There are also no fewer than 10 dedicated children’s hospitals of varying capacities in the country, often privately owned and clustered in the Tier 1 cities of Lagos and Port-Harcourt. Therefore, the demand for paediatric radiology services in Nigeria is huge. Despite this demand for paediatric radiologists, there is a paucity of data quantifying existing medical personnel providing paediatric imaging services in Nigeria. Such data could be useful to policy makers, foreign development partners and other agencies interested in health services for Nigerian children.
The aim of this study was to profile the resources available for paediatric radiology in Nigeria in order to identify gaps and areas for improvement.
Materials and methods
This is a descriptive cross-sectional survey of Nigerian-based certified and trainee radiologists (resident doctors) between October 2017 and April 2018. The certified radiologists were examiners at the Nigerian centre of the West African regional radiology board examinations while the trainee radiologists participated in an update course in clinical radiology. The study instrument was a self-administered semi-structured questionnaire that was pretested on 10 radiologists composed equally of 5 randomly selected radiology trainees and 5 trainers at a teaching hospital in Southwest Nigeria. The four sections of the questionnaire captured anonymous personal information on respondents’ professional training and practice, respondents’ professional affiliations, personnel audit and equipment audit. The responses were entered into a secure electronic database. Data were analysed by descriptive statistical methods using the Statistical Package for Social Sciences (SPSS), version 20.
Results
Out of 100 questionnaires administered to certified radiologists and radiology residents, 80 were returned completed (80%). There were 51 (64%) male respondents and 54 (69%) of the study participants were between 30 years and 50 years old. Forty-six (58%) certified radiologists, 14 (18%) senior and 20 (25%) junior radiology residents completed the questionnaires. Certified radiologists from the Northeast (6 [13%]), North-Central (11 [23.9%]), Northwest (10 [22%]), Southeast (6 [13%]), South-South (2 [4.4%]) and Southwest (11 [23.9%]) geopolitical zones of Nigeria participated in the survey. Only 2 (4.4%) of the 46 certified radiologists were certified within the past 5 years. Seventy-three (91%) of the respondents practiced radiology in tertiary public health facilities.
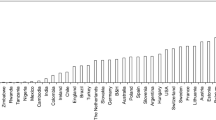
Among the certified radiologists, 10 (21.7%) affirmed that their practice was focused on paediatric imaging and 1 (2.9%) of the trainees had a strong interest in paediatric imaging. Two (4.4%) certified radiologists devoted at least half of their work time to paediatric radiology (Fig. 1). Twenty-two (48%) of the certified radiologists were exposed to some form of subspecialty training abroad, of whom 7 (32%) had the training for at least 6 months. Only one (2.2%) of the certified radiologists received 3 months of training in paediatric radiology overseas. The respondents indicated the presence of other specialist medical staff dedicated to the care of children in their facility. Surgeons (64%), neonatologists (53%) and neurologists (45%) were the top three paediatric specialist medical staff available in the facilities of the respondents. Only 5 (11%) certified radiologists work in facilities where not more than 5 certified radiologists are employed. Forty-two (91%) of the certified radiologists did not know of any colleague who practices in a children-only hospital or dedicated paediatric unit of a mixed hospital. There are at least 5 radiographers in the radiology departments to which 78% of the certified radiologists are affiliated, but no known radiographer with additional training in paediatric radiography. Fewer than 5 nurses also work in the radiology departments with 98% of the certified radiologists.

Proportion of practice time spent in paediatric imaging by the respondents
Pooling the reported numbers by the respondents, the respective functional units for ultrasound (US), X-ray, fluoroscopy, computed tomography (CT), and magnetic resonance imaging (MRI) machines were 286, 188, 33, 49, and 38. Of these numbers, 14 US units (4.9%), 4 X-ray units (2.1%) and 1 MRI unit (1.3%) were reserved for paediatric imaging while no fluoroscopy or CT unit was dedicated to children (Fig. 2).

Pooled numbers of all functional equipment (black) and equipment reserved for children imaging (grey)
A lack of dedicated equipment (44%) and trained paediatric radiologists (24%) were the main challenges to paediatric imaging perceived by the respondents (Fig. 3). The most popular view of the respondents to improve paediatric imaging in Nigeria was to provide dedicated equipment and training (57%).

Perceived challenges of paediatric imaging in Nigeria
Discussion
This cross-sectional survey of senior certified radiologists and radiology residents revealed an acute shortage of radiologists and requisite facilities needed to provide optimal paediatric radiology services in Nigeria. The demand for paediatric imaging, though significant, is not met due to very few dedicated equipment units and inadequate training in paediatric radiology.
Approximately 20% of the certified radiologists are interested in paediatric radiology while less than 5% are actively involved in clinical paediatric radiology. There is also apathy towards paediatric radiology among the radiology residents in this survey, which may be related to the paucity of dedicated trainers and equipment. Other reasons cited in literature for poor interest in paediatric radiology include the perceived difficulty of working with children and inadequate monetary compensation [8]. A previous study also showed that paediatric radiology was not a favourite subspecialty among radiology trainees in Nigeria [9]. Despite being the first radiology subspecialty historically, the paediatric radiology workforce continues to decline globally [10, 11]. Regardless, the young demography of Nigeria calls for homegrown innovative interventions to attract and retain competent radiologists for paediatric imaging.
The quality of training received by practitioners of paediatric radiology in Nigeria is also poor. In our survey, only one (2.2%) of the certified radiologists had at least 3 months of basic training in paediatric radiology. There was no fellowship-trained paediatric radiologist in Nigeria at the time of the survey. Both the national and the West African regional postgraduate bodies that regulate the training of Nigerian radiologists must evolve a need-based mechanism that could supply adequately trained manpower for medical imaging of children. Nigeria could also emulate the approach of other developing economies like Ethiopia and India with similar young populations. A paediatric radiology fellowship is thriving in Ethiopia supported by the Children’s Hospital of Philadelphia, PA [12]. India has a couple of institutions offering paediatric radiology fellowships that enjoy robust support from Indian radiologists in the diaspora [8]. Making paediatric radiology training a priority is nonnegotiable given the current and projected demographics of Nigeria in which children constitute the single largest population group. In this regard, general radiologists who provide nearly all paediatric imaging services in Nigeria can also benefit from periodic refresher courses facilitated by large imaging organizations such as the Radiological Society of North America (RSNA) or European Society of Radiology (ESR); free electronic learning from credible sources like the World Federation of Paediatric Imaging, and local packages including boot camps and continuing medical education sessions led by the Society for Paediatric Imaging in Nigeria (SPIN).
Furthermore, the case for upgrading radiology practice in Nigeria to a subspecialist level is particularly true for paediatric radiology. Our data showed an impressive spread of other medical and surgical specialties primarily involved in the care of Nigeria children. Besides general paediatrics, the respondents serve paediatric specialists, including paediatric surgeons, neonatologists and neurologists among others. These other paediatric specialties are growing in Nigeria despite the general shortage of physicians. SPIN is actively advocating subspecialty practice as a medium- to long-term panacea so paediatric radiology is not left behind other clinical specialties in child health [13]. The dearth of competent paediatric radiologists ultimately contributes to suboptimal clinical outcomes and may even expose children to danger in the hands of dated ad hoc paediatric radiologists or outright quacks.
The methods utilized for the medical imaging of children in Nigeria are largely inappropriate. Our respondents reported widespread paucity of dedicated equipment for the practice of paediatric radiology. It could be inferred that Nigerian children are routinely imaged on equipment unsuitable from the perspectives of image quality, radiation safety and clinical comfort. Therefore, there is an urgent need to escalate the Image Gently campaign in Nigeria to reach policy and decision makers. The requirements of children should be considered when decisions on procurement of radiology equipment are made at various levels of the Nigerian health system to align with global best practices [14]. Radiology departments in Nigeria should also be aware of alternative sources of acquiring appropriate imaging equipment, which are not limited to philanthropic entities like RAD-AID International or Rotary International. There should also be more emphasis on improving the capacity of local biomedical technical staff for preventive maintenance of sourced imaging equipment while holding vendors to a higher degree of responsibility when supplying equipment that could be used on children. In addition, the lack of training in paediatric radiography needs to be jointly addressed by local and external partners to prevent the exacerbation of an already overwhelming cancer burden in Nigeria.
This present attempt at documenting the capacity of paediatric radiology in Nigeria draws its strength from the impeccable credibility of the respondents. The 46 board-certified radiologists who participated in the survey represent approximately 15–18% of the estimated 250–300 certified radiologists in Nigeria [5]. The West African board examinations in radiology are a meeting point of examiners, radiologists with more than 5 years of post-qualification clinical and teaching experience selected from all parts of the country [15]. Therefore, the data from this survey fairly depict the situation across Nigeria, especially at the public tertiary health facilities where 91% of respondents were employed.
It is difficult to interpret or compare our data in the context of similar developing economies, which was the focus of the study. Reasons for this limitation include a paucity of similar works and the lack of international standards on the minimum acceptable practice of paediatric radiology (workforce, training, facilities, radiation protection measures, funding) in low- and middle-income countries. Paediatric radiology is not alone in this dire situation, but it can adapt good global initiatives addressing similar challenges such as that of paediatric surgery [16, 17]. We acknowledge that there may be some recall bias due to the study method. However, the high functional status of the majority of the respondents would have minimized any effect of recall bias on the interpretation of our results. Lastly, other important personnel involved in safe medical imaging of children, such as physicists and biomedical engineers, were not included in this personnel audit, which focused on clinical staff.
Conclusion
There is a substantial deficit of human and material resources for paediatric imaging in Nigeria despite a predominantly young population. Paediatric radiology is not a favourite subspecialty among certified radiologists in Nigeria. Informed investment in dedicated equipment and innovative training are necessary to boost the capacity for paediatric radiology in this developing nation.
References
National Bureau of Statistics (2016) National population estimates 2006–2016. http://www.nigerianstat.gov.ng/download/474. Accessed 8 Jan 2019
UNICEF Nigeria (2019) Situation of women and children in Nigeria. https://www.unicef.org/nigeria/situation-women-and-children-nigeria. Accessed 21 Aug 2019
Ekure EN, Esezobor CI, Balogun MR et al (2013) Paediatrician workforce in Nigeria and impact on child health. Niger J Paed 40:112–118
Ekure EN, Sadoh WE, Bode-Thomas F et al (2017) Audit of availability and distribution of paediatric cardiology services and facilities in Nigeria. Cardiovasc J Afr 28:54–59
Soroosh G, Ninalowo H, Hutchens A, Khan S (2015) Nigeria country report. https://www.rad-aid.org/wp-content/uploads/Nigeria-Country-Report-Final.pdf. Accessed 5 Jan 2019
The Association of Radiographers of Nigeria (2019) All about membership. http://www.arn.org.ng/members/. Accessed 20 Aug 2019
Medical and Dental Council of Nigeria (2019) Teaching hospitals approved by the medical and dental council of Nigeria for internship training. https://www.mdcn.gov.ng/public/storage/documents/document/_812954199.pdf. Accessed 13 Aug 2019
Therakathu J, Yadav VK, Keshava SN et al (2017) The current status of pediatric radiology in India: a conference-based survey. Indian J Radiol Imaging 27:73–77
Atalabi OM, Adekanmi AJ, Bamgboye EA (2013) The state of radiology subspecialty training in the west African subregion: the residents’ perspective. West Afr J Radiol 20:69–73
Griscom NT (1995) History of pediatric radiology in the United States and Canada: images and trends. Radiographics 15:1399–1422
Merewitz L, Sunshine JH (2006) A portrait of pediatric radiologists in the United States. AJR Am J Roentgenol 186:12–22
Darge K, Gorfu Y, Jaramillo D (2014) Ethiopia: who to educate, how to educate and what to teach. Pediatr Radiol 44:642
Atalabi OM, Omidiji O (2014) Radiologists join to implement pediatric imaging training, education and outreach in Nigeria. Pediatr Radiol 44:669
International Atomic Energy Agency (2012) Considerations in the equipment procurement and immobilization of patients. In: IAEA (ed) Radiation protection in paediatric radiology. IAEA, Vienna, pp 18–19
Idowu BM (2018) Postgraduate radiology education in Nigeria: looking backward and forward. SA J Radiol 22:1362
Global Initiative for Children’s Surgery (2019) Global initiative for children’s surgery: a model of global collaboration to advance the surgical care of children. World J Surg 43:1416–1425
Toobaie A, Emil S, Ozgediz D et al (2017) Pediatric surgical capacity in Africa: current status and future needs. J Pediatr Surg 52:843–848
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Olatunji, R.B., Akinmoladun, J.A. & Atalabi, O.M. Capacity for paediatric radiology in Nigeria: a survey of radiologists. Pediatr Radiol 51, 587–591 (2021). https://doi.org/10.1007/s00247-019-04610-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-019-04610-2