
Abstract
Background
Many image-intensifier fluoroscopy systems have been replaced by flat-panel detectors in recent years.
Objective
To compare the level of contrast, image resolution and radiation dose between an image-intensifier and a newer-generation flat-panel detector system in a pediatric radiology unit.
Materials and methods
We compared two systems — a conventional image intensifier and a newer-generation flat-panel system. We measured image quality and radiation dose using a technical phantom. Additionally, we retrospectively compared age-matched fluoroscopic pediatric voiding cystourethrography (n = 15) and upper gastrointestinal investigations (n = 25).
Results
In phantom studies image contrast was equal while image resolution was higher and mean radiation dose lower using the flat-panel system (P < 0.0001). In pediatric investigations, mean dose area product was significantly reduced on the flat-panel system for upper gastrointestinal investigation (45 ± 38 μGy*m2 vs. 11 ± 9 μGy*m2; P < 0.0001) and for voiding cystourethrography (18 ± 20 μGy*m2 vs. 10 ± 12 μGy*m2; P = 0.04).
Conclusion
The newer flat-panel system performs at lower dose levels with equal to better image quality and therefore seems to be the more suitable technique for pediatric fluoroscopy in comparison to image-intensifier systems.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Flat-panel detector systems have increasingly replaced image-intensifier systems in recent years in several areas such as cardiac and angiographic procedures [1]. Some advantages of flat-panel detectors are obvious, such as the absence of geometric distortion and vignetting, the insensitivity to magnetic fields, the smaller size, the longer lifetime and the wider dynamic range [2]. With regard to radiation dose, some authors have demonstrated better image quality with lower doses using flat-panel detectors. Although fluoroscopic devices perform at low-dose levels compared to CT, and although it has been demonstrated that postnatal exposure to diagnostic radiography does not increase the incidence of malignancies [3], pediatric radiologists should try to perform diagnostic imaging at the lowest achievable dose levels to reduce cumulative dose [4]. Some children are exposed to many fluoroscopic investigations, such as upper gastrointestinal or voiding cystourethrography studies, for example, in the diagnosis and care of reflux diseases [5–9].
Nevertheless, literature concerning dose-comparison of image-intensifier with flat-panel systems is discordant. Some studies conclude that flat-panel detectors are superior to image-intensifier systems with regard to dose, and others conclude the superiority of image intensifiers. Hatakeyama et al. [10] demonstrated dose reduction associated with a higher image quality when using a flat-panel detector in a neuro-angiographic phantom, whereas other authors found a dose increase with equal image-quality in an angiographic phantom [11]. These studies were performed in adults at relatively high exposure rates. Investigations in pediatric radiology are rare because, first, table-side-controlled flat-panel detector devices are relatively rare and, second, first-generation flat-panel detector systems showed low performance in low-dose fluoroscopy. Miraglia et al. [12] demonstrated that in children with biliary interventions, a newer-generation flat-panel detector system was superior to an image-intensifier system in the question of dose [12]. Recently, the same group confirmed its results in a study in which authors compared both fluoroscopic devices in the field of venous catheter placement [13].
The controversy in the literature and the lack of pediatric-focused studies attest to the need for further phantom-based studies that directly compare image quality and dose between the two technologies at low exposure levels. We therefore used a technical phantom supplemented by an ion-chamber to compare two systems that are used for pediatric radiology in our department, an image-intensifier and a newer-generation flat-panel detector system. Additionally, we retrospectively performed a matched-pair analysis of fluoroscopic investigations that have been performed at our institution to test the hypothesis that the replacement of an older image-intensifier system by a flat-panel detector system leads to a dose reduction at equal to better image quality in pediatric fluoroscopy.
Materials and methods
Imaging systems and image parameters
We compared two radiographic and fluoroscopic imaging systems of our pediatric radiology department — one image intensifier and one flat-panel detector. The image-intensifier system was the EasyDiagnost Eleva (Philips Healthcare, Best, The Netherlands). This system offers a maximum field of view (FOV) of 36 cm with two magnification steps (FOV 23 cm and 17 cm). The flat-panel detector system was the new Luminos Agile (Siemens Healthcare, Forchheim, Germany). This system has at maximum an FOV of 42 cm with three magnification modes of 30 cm, 22 cm and 15 cm. Both systems are under-couch systems.
Technical phantom — data acquisition
Dose measurements were based on the DIN 6868-4 guideline http://www.gaa.baden-wuerttemberg.de/servlet/is/16510/5_09.pdf. We used the technical phantom Primus DL (IBA Dosimetry GmbH, Schwarzenbruck, Germany) (Fig. 1). With this phantom image contrast can be measured by evaluating the visible gray range and the number of low-contrast objects (circles). Additionally, image resolution can be measured by comparing the number of line pairs per mm (lp/mm). Radiation dose was recorded by the dose area product (DAP) on the one hand and an ion chamber integrated in the center of the technical phantom on the other hand.

Technical phantom. With the technical phantom several features can be measured, including contrast detection with a maximum of 17 steps (A), detection of low-contrast objects with a maximum of eight circles (B) and spatial resolution as line pairs/mm (C)
For both systems a typical pediatric pulse rate of 3 pulses per second was chosen in fluoroscopic mode. Both systems were used in the fluoroscopic and radiographic mode (digital fluoro-radiography) with all magnification steps. For dose evaluation in fluoroscopy, a radiation time of 20 s was chosen for each magnification step on both systems. Measurements with the full field of view were repeated five times to check inter-measurement dose variances. In fluoroscopy mode, the tube voltage range for the flat-panel system was 70–73 kVp and for the image intensifier it was 61–72 kVp. In the radiographic mode, tube voltage of the flat-panel system was 70 kVp and for the image intensifier it was 70–77 kVp (Table 1). For both systems focus-table distance was 60 cm, focus-ionizing chamber distance 62 cm and focus-phantom distance 100 cm. The phantom-detector distance for the flat-panel system was 4 cm, and it was 13 cm for the image-intensifier system. For both systems an additional filtering of 1 mm aluminum (Al) plus 0.2 mm copper (Cu) was applied. The anti-scatter grid was not used for either system.
Pediatric study, matched-pair analysis
Twenty-five consecutive upper gastrointestinal passage investigations were performed on the flat-panel detector system. For each investigation, we selected the best age-matched patient who had been investigated on the image-intensifier system in the last 2 years. We retrospectively compared investigations by the dose area product and the investigation time.
Correspondingly, 15 consecutive voiding cystourethrography investigations were analyzed by a matched-pair analysis concerning dose and investigation time. These parameters were available in the dose data protocol of our picture archiving system. Magnification mode, anti-scatter grid and radiographic mode were not used in pediatric fluoroscopic investigations. For image storage, last-image-hold was applied. All investigations were performed by a single radiologist (T.D.) with 30 years of experience in pediatric radiology. Range of tube voltage was similar between both systems, namely 80–95 kVp in upper gastrointestinal series and 75–85 kVp in voiding cystourethrography examinations. Focal spot size was 0.6 mm for the flat-panel system and 0.4 mm for the image-intensifier system. For both systems an additional filtering of 1 mm Al and 0.2 mm Cu was applied.
The retrospective analysis of patient parameters was approved by the institutional research ethics committee.
Statistical analysis
Image resolution was evaluated by two readers in consensus (K.W.N.: >20 years of experience in radiology, M.W.: 3 years of experience in radiology). Values of both systems were compared using visual and graphical analysis. A Shapiro–Wilk normality test confirmed normal distribution of data and a two-sampled t-test was used to compare absolute dose value.
A Wilcoxon matched pair test was used to compare absolute dose values of the retrospective matched-pair patient analysis when data were not normally distributed. The Fisher exact test was applied to evaluate the gender distribution of both groups.
Results
Technical phantom
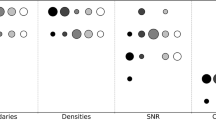
Contrast resolution was similar for both systems, especially in the fluoroscopic mode. With both systems in the maximum field of view 16 gray-scale values could be detected, and in the magnification modes all 17 gray-scale values were visible. In the radiographic mode it became obvious that the image-intensifier system overexposed the image at a high magnification mode, which resulted in the limited differentiation of only seven gray-scale values. The detection of low-contrast objects was comparable between systems.
Spatial resolution was better for the flat-panel system than for the image-intensifier system, especially in the radiographic mode (Fig. 2). In detail, spatial resolution for the flat-panel system was in the mean 1.5 lp/mm in the fluoroscopic mode vs. 1.3 lp/mm for the image-intensifier system. In the radiographic mode, the spatial resolution of the flat-panel system was in the mean 1.9 lp/mm in comparison to 1.3 lp/mm for the image-intensifier system.

Spatial resolution: comparison of newer flat-panel detector with image intensifier. a, b For the flat-panel system a higher spatial resolution was achieved for both the fluoroscopic mode (a) and the radiographic mode (b). FOV field of view, lp line pairs
The standard deviation of repeated entrance dose rate (EDR) measurements in full field of view was less than 0.1%. EDR was reduced by the flat-panel system in fluoroscopic mode (2.8 mGy/min vs. 8.0 mGy/min, P < 0.0001; Fig. 3) and in radiographic mode (21.3 mGy/min vs. 112.4 mGy/min). Radiation dose reduction measured by the dose area product (DAP) was equivalent (mean DAP 9.0 mGy*m2 vs. 20.2 mGy*m2; Table 1). As expected, dose increased proportionally to a quadratic curve for the image-intensifier system and linearly for the flat-panel system. Therefore dose differences were biggest in the highest magnification mode.

Entrance dose rate measured by ion chamber — comparison of newer flat-panel detector with image intensifier. a, b Radiation dose was higher with the image-intensifier system in comparison to the flat-panel detector in both fluoroscopic (a) and radiographic (b) modes. FOV field of view
Pediatric study, matched-pair analysis
For both investigation types — gastrointestinal and voiding cystourethrography — patient age was similar between the groups after matching (Table 2).
For the gastrointestinal passage the dose area product was less for the flat-panel detector (10.9 ± 8.7 μGy*m2) in comparison to the image intensifier (44.6 ± 37.8 μGy*m2; P < 0.001). Investigation time was similar between the systems (P = 0.4; Table 2).
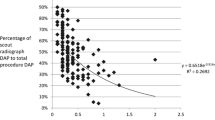
In voiding cystourethrography investigations, radiation dose was also statistically significantly reduced for the flat-panel detector (10.0 ± 12.2 μGy*m2) in comparison to the image intensifier (17.7 ± 19.7 μGy*m2; P = 0.04). Examination time was similar between the systems (P = 0.9; Table 2). With regard to age-dependency of dose, it became obvious that the biggest dose differences between the systems were present in older children (Fig. 4).

Dose dependency on age in fluoroscopic investigations. a, b For both investigation types — gastrointestinal passage (a) and voiding cystourethrography (b) — the radiation dose increased with increasing patient age. The biggest difference in dose between the image intensifier and the flat-panel detector system (FPD) is seen in older children
Discussion
The newer-generation flat-panel system generated better image quality at a lower radiation dose in comparison to the image-intensifier system, when using a technical phantom and typical image parameters for the pediatric patient. Additionally, the retrospective evaluation of pediatric investigations showed that the flat-panel detector system performed at a lower radiation dose.
Our results are supported by Hatakeyama et al. [10], who investigated a neuroangiographic phantom with two systems. They concluded that the flat-panel detector achieved a considerable dose reduction without a loss of image quality. Tsapaki and colleagues [14] came to a similar conclusion when they compared a flat-panel detector system and an image-intensifier system in cardiac procedures. They found that a dose reduction is possible with the newer flat-panel device.
Nevertheless, literature is discordant. Other authors conclude that skin dose is not significantly reduced by the flat-panel detector [15]. Bogaert et al. [16] showed that image quality was increased with the use of a flat-panel device because of its intrinsic better performance but radiation dose was the same in cardiac procedures. Some authors even measured a dose increase at the same image quality when using the flat-panel detector in comparison to the image intensifier [11, 17]. Such unfavorable results for the flat-panel system are in contrast to the better physical properties of flat-panel detectors, such as lack of geometric distortion, excellent image uniformity, and lack of veiling glare or vignetting. As with image-intensifier systems, flat-panels have a rectangular FOV and wide dynamic range response [2]. All of these studies were performed in adults and at relatively high exposure rates. In pediatric radiology, low frame-rates (3 pulses/s) are used and therefore the comparison of studies here is difficult. Only very few studies have investigated the performance of flat-panel-based fluoroscopy in children, for a couple reasons: table-side-controlled flat-panel detector devices have been rarely used until recently, and first-generation flat-panel systems have shown low performance in the low-dose area. The reason for low performance in low-dose investigation was that signal amplification, which is always necessary in low-dose images, introduced image noise that decreased image quality [2]. The manufacturers worked to overcome those problems and now investigations at low exposure rates are possible and have to be evaluated in children in future studies.
Miraglia et al. [12] performed biliary procedures in pediatric patients after liver-transplantation on two different imaging systems — one an image intensifier and one a flat-panel detector. They demonstrated that for all subgroups of procedures, the dose area product was significantly reduced using the flat-panel system [12]. These results are in good accordance to the results of the present study; we also demonstrated a significantly decreased radiation dose for the flat-panel detector device in pediatric gastrointestinal and voiding cystourethrography investigations. Those differences were even more obvious for older children. Older children are mostly heavier and therefore one explanation for the age-dependency of dose might be that the image-intensifier systems had to increase dose to a higher degree than the flat-panel detector devices to maintain the same image quality. More studies are needed to evaluate the use of newer flat-panel detector systems in pediatric radiology.
In pediatric radiology the question of dose has gained public awareness [18]. Campaigns such as “Image Gently, Step Lightly” have increased the awareness of dose in pediatric interventional radiology [19, 20]. This is of special importance because there are still many indications for pediatric fluoroscopic exams [21]. For example, recurring bladder infection in infants is a well-known and a widely accepted indication for voiding cystourethrography [22, 23]. Additionally, upper gastrointestinal passage investigations are often needed to evaluate gastrointestinal symptoms to exclude, for example, reflux disease [8, 24, 25]. A big intra- and inter-institution variance has been demonstrated in pediatric fluoroscopic dose values, which underlines the need for more standardized investigation protocols [26]. This becomes even more important against the background that diagnostic dose reference values are a poor guide for inexperienced radiologists because much lower doses can be achieved [27]. To exclude variances in investigation protocols in our study, a single investigator with about 30 years of experience in pediatric radiology performed all pediatric examinations.
The main limitation of the present study is that a technical phantom, which does not fully reflect the physiological properties of a real patient, was used for objective image-quality comparison. The clinical translation to pediatric radiology is therefore difficult. Nevertheless we could compare objective image parameters by means of this technical phantom. Additionally, dose measurements with the technical phantom are clearly supported by the results of the retrospective matched-pair analysis of pediatric investigations. Because of device-specific properties, absolute kVp was slightly different between image-intensifier and flat-panel systems in the technical phantom part, which could have influenced results. But because tube voltage was in similar ranges and the differences are caused by intrinsic properties of image-intensifiers and flat-panel detectors themselves, in our opinion a comparison is suitable. Another limitation of our study is that the matched-pair analysis is based on patient age. Of course patient diameter or patient body weight would have been more appropriate parameters. But as neither diameter nor weight was available, and because body weight and age are strongly correlated in children, age seemed to be a suitable approach.
Conclusion
When using a technical phantom and typical image parameters for children the newer flat-panel detector-based system reaches a better image quality with lower radiation dose when compared to a conventional image-intensifier system. Clinical fluoroscopic examinations were performed with less radiation dose on the flat-panel detector device. The flat-panel system therefore seems better suited for pediatric radiology, but further investigation is needed.
References
Partridge J, McGahan G, Causton S et al (2006) Radiation dose reduction without compromise of image quality in cardiac angiography and intervention with the use of a flat panel detector without an antiscatter grid. Heart 92:507–510
Seibert JA (2006) Flat-panel detectors: how much better are they? Pediatr Radiol 36:173–181
Hammer GP, Seidenbusch MC, Schneider K et al (2009) A cohort study of childhood cancer incidence after postnatal diagnostic X-ray exposure. Radiat Res 171:504–512
Justino H (2006) The ALARA concept in pediatric cardiac catheterization: techniques and tactics for managing radiation dose. Pediatr Radiol 36:146–153
Darling S, Sammer M, Chapman T et al (2011) Physician documentation of fluoroscopy time in voiding cystourethrography reports correlates with lower fluoroscopy times: a surrogate marker of patient radiation exposure. AJR Am J Roentgenol 196:W777–W780
Malekzadeh M, Bahreyni Toossi MT, Alamdaran SA et al (2012) Comparison between patient dose arising from photofluorographic and standard fluoroscopic voiding cystourethrography in children with urinary tract infection [corrected]. Nephrourol Mon 4:541–544
Nel ED, Ellis A (2012) Swallowing abnormalities in HIV infected children: an important cause of morbidity. BMC Pediatr 12:68
Rommel N, Selleslagh M, Hoffman I et al (2014) Objective assessment of swallow function in children with suspected aspiration using pharyngeal automated impedance manometry. J Pediatr Gastroenterol Nutr 58:789–794
Baijens L, Barikroo A, Pilz W (2013) Intrarater and interrater reliability for measurements in videofluoroscopy of swallowing. Eur J Radiol 82:1683–1695
Hatakeyama Y, Kakeda S, Ohnari N et al (2007) Reduction of radiation dose for cerebral angiography using flat panel detector of direct conversion type: a vascular phantom study. AJNR Am J Neuroradiol 28:645–650
Wiesinger B, Stutz A, Schmehl J et al (2012) Comparison of digital flat-panel detector and conventional angiography machines: evaluation of stent detection rates, visibility scores, and dose-area products. AJR Am J Roentgenol 198:946–954
Miraglia R, Maruzzelli L, Tuzzolino F et al (2013) Radiation exposure in biliary procedures performed to manage anastomotic strictures in pediatric liver transplant recipients: comparison between radiation exposure levels using an image intensifier and a flat-panel detector-based system. Cardiovasc Intervent Radiol 36:1670–1676
Miraglia R, Maruzzelli L, Cortis K et al (2015) Comparison between radiation exposure levels using an image intensifier and a flat-panel detector-based system in image-guided central venous catheter placement in children weighing less than 10 kg. Pediatr Radiol 45:235–240
Tsapaki V, Kottou S, Kollaros N et al (2004) Comparison of a conventional and a flat-panel digital system in interventional cardiology procedures. Br J Radiol 77:562–567
Chida K, Inaba Y, Saito H et al (2009) Radiation dose of interventional radiology system using a flat-panel detector. AJR Am J Roentgenol 193:1680–1685
Bogaert E, Bacher K, Lapere R et al (2009) Does digital flat detector technology tip the scale towards better image quality or reduced patient dose in interventional cardiology? Eur J Radiol 72:348–353
Wiesinger B, Kirchner S, Blumenstock G et al (2013) Difference in dose area product between analog image intensifier and digital flat panel detector in peripheral angiography and the effect of BMI. Röfo 185:153–159
Cohen M (2007) Are we doing enough to minimize fluoroscopic radiation exposure in children? Pediatr Radiol 37:1020–1024
Sidhu M, Coley BD, Goske MJ et al (2009) Image Gently, Step Lightly: increasing radiation dose awareness in pediatric interventional radiology. Pediatr Radiol 39:1135–1138
Sidhu M, Goske MJ, Connolly B et al (2010) Image Gently, Step Lightly: promoting radiation safety in pediatric interventional radiology. AJR Am J Roentgenol 195:W299–W301
Schneider K, Krüger-Stollfuss I, Ernst G et al (2001) Paediatric fluoroscopy — a survey of children’s hospitals in Europe. I. Staffing, frequency of fluoroscopic procedures and investigation technique. Pediatr Radiol 31:238–246
Hsi RS, Dearn J, Dean M et al (2013) Effective and organ specific radiation doses from videourodynamics in children. J Urol 190:1364–1369
Riccabona M, Lobo ML, Willi U et al (2014) ESPR uroradiology task force and ESUR Paediatric Work Group — Imaging recommendations in paediatric uroradiology, part VI: childhood renal biopsy and imaging of neonatal and infant genital tract: minutes from the task force session at the annual ESPR Meeting 2012 in Athens on childhood renal biopsy and imaging neonatal genitalia. Pediatr Radiol 44:496–502
Tompane T, Leong CW, Bush R et al (2013) Appropriateness of radiology procedures performed in children with gastrointestinal symptoms and conditions. Clin Gastroenterol Hepatol 12:970–977
Hiorns MP, Ryan MM (2006) Current practice in paediatric videofluoroscopy. Pediatr Radiol 36:911–919
Schneider K, Perlmutter N, Arthur R et al (2000) Micturition cystourethrography in paediatric patients in selected children’s hospitals in Europe: evaluation of fluoroscopy technique, image quality criteria and dose. Radiat Prot Dosim 90:197–201
Hiorns MP, Saini A, Marsden PJ (2006) A review of current local dose-area product levels for paediatric fluoroscopy in a tertiary referral centre compared with national standards. Why are they so different? Br J Radiol 79:326–330
Conflicts of interest
The Institute of Clinical Radiology and Nuclear Medicine Mannheim has research agreements with Siemens Healthcare Sector.
The study received financial funding from Siemens. None of the authors of the study was employee of Siemens. Measurements and data evaluation were not supported by Siemens.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Weis, M., Hagelstein, C., Diehm, T. et al. Comparison of image quality and radiation dose between an image-intensifier system and a newer-generation flat-panel detector system — technical phantom measurements and evaluation of clinical imaging in children. Pediatr Radiol 46, 286–292 (2016). https://doi.org/10.1007/s00247-015-3456-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-015-3456-z