
Abstract
Purpose
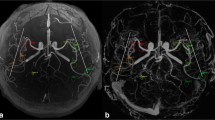
3D multi-echo gradient-recalled echo (ME-GRE) can simultaneously generate time-of-flight magnetic resonance angiography (pTOF) in addition to T2*-based susceptibility-weighted images (SWI). We assessed the clinical performance of pTOF generated from a 3D ME-GRE acquisition compared with conventional TOF-MRA (cTOF).
Methods
Eighty consecutive children were retrospectively identified who obtained 3D ME-GRE alongside cTOF. Two blinded readers independently assessed pTOF derived from 3D ME-GRE and compared them with cTOF. A 5-point Likert scale was used to rank lesion conspicuity and to assess for diagnostic confidence.
Results
Across 80 pediatric neurovascular pathologies, a similar number of lesions were reported on pTOF and cTOF (43–40%, respectively, p > 0.05). Rating of lesion conspicuity was higher with cTOF (4.5 ± 1.0) as compared with pTOF (4.0 ± 0.7), but this was not significantly different (p = 0.06). Diagnostic confidence was rated higher with cTOF (4.8 ± 0.5) than that of pTOF (3.7 ± 0.6; p < 0.001). Overall, the inter-rater agreement between two readers for lesion count on pTOF was classified as almost perfect (κ = 0.98, 96% CI 0.8–1.0).
Conclusions
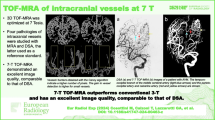
In this study, TOF-MRA simultaneously generated in addition to SWI from 3D MR-GRE can serve as a diagnostic adjunct, particularly for proximal vessel disease and when conventional TOF-MRA images are absent.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Gradient recalled echo (GRE) MRI techniques have wide applications in clinical MRI due to their scan speed and anatomic characterization. Two such routine uses of GRE-based methods are T2*-based 2D/3D GRE for highlighting tissues prone to magnetic susceptibility effects such as hemorrhage, mineralization, or deoxygenated blood, and a 3D time-of-flight magnetic resonance angiography (TOF-MRA) for assessing cerebral arteries [1, 2]. Examples of T2* imaging include 2D GRE, SWI, or SWAN, and are routinely used to in the setting of stroke and trauma, as well as neurologic diseases with iron or hemosiderin deposition. TOF-MRA and its rotation maximum intensity projection images are often used to assess steno-occlusive lesions, cerebral arteriopathy, aneurysms, or vascular malformation.
In the pediatric setting, an efficient scan time is desirable to reduce sedation requirements, particularly in young children who are often motion-prone. The 3D multi-echo (ME) GRE technique may be a useful candidate for reducing scan time, as it facilitates simultaneous generation of naturally co-registered images with various contrasts [3,4,5]. This “plural contrast” sequence has been shown to generate images such as conventional T2* magnitude images, TOF, susceptibility-weighted images (SWI), quantitative susceptibility maps (QSM), R2* maps, and others (Supp Fig. 1). Notably, SWI has been shown more sensitive than standard (magnitude-based 2D GRE) T2*-imaging, as it further exploits variations in tissue magnetic susceptibility associated with venous blood, calcification, hemorrhage, and iron deposition [6,7,8,9,10,11]. However, the potential clinical utility of TOF-MRA processed from a 3D ME-GRE typically used for SWI, SWAN, or QSM imaging has not been explored.
Recently, there have been important breakthroughs in routine fast brain imaging, including the 5 min GO brain protocol [12] and the 1 min brain protocol [13]. The latter combines generative six MRI contrasts (T1-FLAIR, T2-w, DWI, ADC, T2*-w, T2-FLAIR) in a single sequence. In a similar vein, the work here strives toward this goal of using one sequence to generate multiple contrasts.
Here we utilize the 3D ME-GRE sequence to calculate the following swap mechanisms: a TOF-MRA from a first “echo image” (designated ‘pseudo-TOF’, or pTOF), and a T2*-weighted gradient echo image from a later second echo [3]. Here, the first (TOF) echo utilizes the inflow of unsaturated spins into the acquisition volume [1], whereas the later echo is based on the T2* effect [14] for venous imaging. The phase information in this 3D-based GRE method, which is typically discarded in routine clinical workflow, can also be used to calculate an SWI image.
This study goal was to simultaneously generate pTOF images and SWI from a routine 3D ME-GRE sequence, and evaluate the clinical performance of the generated pTOF images. We hypothesized that pTOF generated from a 3D ME-GRE acquisition that is typically used to generate a T2* image (SWI or SWAN) could provide diagnostic information contained within independently acquired conventional TOF-MRA (here denoted cTOF) for evaluating pediatric neurovascular pathology.
Materials and methods
Subjects
With an IRB approval, eighty consecutive pediatric patients presenting for evaluation of neurovascular pathology were retrospectively identified at our institution. Inclusion criteria were patients who obtained two image sequences on a 3 T MRI system, comprising 3D ME-GRE, and 3D TOF MRA (cTOF). Non-diagnostic images due to patient motion and metal artifacts were excluded. Subjects included 32 females and 48 males, with a mean age of 10.2 years (range 2 days to 39 years). The types of neurovascular pathology by final diagnosis are listed in Supplemental Table 1.
MR imaging
All imaging was performed on a 3 T GE scanner (MR750, GE Healthcare Systems, Waukesha, WI) equipped with an 8-channel head-coil. As part of routine neurovascular protocol for pediatric brain, a flow-compensated, single slab, 3D parallel-imaging-accelerated ME-GRE sequence was acquired with the following parameters: axial plane, FOV = 22 cm, matrix size = 384 × 256, number of partitions = 66, resolution = 0.6 × 0.9 × 2 mm3, acceleration factor = 2, flip angle = 15°, TR = 36 ms, seven echoes ranging from TE = 4 m – 33 ms (4.8 ms increments), and scan time = 5:44 min. On completion of the scan, the raw data from the scanner was automatically reconstructed using compiled threaded MATLAB (version 7.8.0; MathWorks Inc., Natick, MA, USA) code, with all images sent to the hospital PACS database in less than 4 min.
For the pTOF images, the 8-channel coil data (first echo only) were first combined with the complex sum-of-squares, followed by taking the maximum intensity projection (MIP) over the slices. To generate the SWI images, first the weighted magnitude images were calculated by combining all the echo images, using the echo time as a weighting factor. This was followed by SWI-processing: here the last echo (TE = 33 ms) was used to generate a phase mask using a 2D Hanning window; this mask was then multiplied 5 times by the magnitude of the weighted combination of the two echoes [7, 15]. This SWI processing was performed on a per coil basis, followed by coil combination using the sum-of-squares approach. While multi-stab ME-GRE could be considered, in this study, we were curious if a faster single-slab ME-GRE typically designed for clinical T2* imaging could retroactively be processed to generate a clinically useful “time of flight-like” MRA image.
The conventional single slab 3D TOF-MRA (cTOF) were acquired using the following parameters: axial plane, FOV = 22 cm, matrix size = 384 × 224, number of partitions = 128, NEX = 5, phase FOV = 0.75, resolution = 0.6 × 1.0 × 1.2 mm3, acceleration factor = 2, flip angle = 15°, TR/TE = 24/3 ms, and scan time = 3:46 min. Other standard of care routine brain sequences included: diffusion-weighted imaging (DWI), 3D T1 spoiled gradient echo (SPGR), T2 fast spin echo (FSE), T1 FLAIR, and arterial spin labeling (ASL) perfusion.
Imaging evaluation
Two board-certified neuroradiologists with Certificate of Added Qualification (KY, MI; over ten and five years of experience, respectively) independently evaluated the randomized datasets comprising pTOF that were simultaneously generated from 3D ME-GRE, and its single-sequence alternative (cTOF images) for the 80 patients. The readers were blinded to the type of the sequence and underlying pathology and reviewed the images in two separate sessions with at least a two-week interval to minimize recall bias.
The reviewers evaluated each of the two image datasets (pTOF, cTOF) for quality using a modified 5-point Likert scale: 1 nondiagnostic, 2 poor, 3 average, 4 good, 5 outstanding. Specifically, the reviewers evaluated for lesion conspicuity if they identified an underlying pathology or for conspicuity of normal vasculature if the cases were considered negative. If neurovascular lesions (e.g., steno-occlusion, vascular malformation, or aneurysm) were present on pTOF or cTOF, the reviewers also labeled the lesion location and number.
The reviewers also evaluated for overall diagnostic confidence in making the final diagnostic decision, also using the Likert scale. The final clinical diagnosis was made by consensus between the two reviewers, the final MRI report, and all clinical and all available imaging material (including previous exams or associated digital subtraction angiography if available), which served as ground of truth for the study. All statistical analyses were done with MATLAB code (version 7.8.0; MathWorks Inc., Natick, MA, USA). Wilcoxon signed-rank tests were used to assess the radiologists’ ratings.
Results
We respectively identified 80 consecutive subjects who had undergone 3D ME-GRE alongside conventional sequences of TOF-MRA and 2D GRE. Out of 80 subjects, neurovascular pathology was identified in 32 subjects (40% of total subjects, Table 1). Supplementary Table 1 outlines the initial indication for MRI across all subjects.
pTOF versus cTOF in diagnostic performance
Across 80 images read by two independent evaluators, the rating of lesion conspicuity on pTOF was higher than that of cTOF; however, this was non-significant (Fig. 1, Table 2; 4.0 ± 0.7 versus 4.5 ± 1.0, respectively, p = 0.06). Diagnostic confidence was rated as significantly higher using cTOF as compared with pTOF (4.8 ± 0.5 versus 3.7 ± 0.6, respectively, p < 0.001). Furthermore, the inter-rater reliability for lesion number across 80 images was classified as almost perfect in agreement (κ = 0.98, 96% CI 0.8–1.0). Specifically, more patients were identified to have lesions on pTOF than cTOF (43% of patients versus 40%, respectively), but this was not statistically significant. A total of 92 lesions over all patients were found on pTOF and 82 lesions were found on cTOF. In one patient, it was found that pTOF could depict superior anatomic vascularity compared with the cTOF.

Mean grade value of the readers’ assessment of lesion conspicuity and diagnostic confidence for (a) TOF-MRA generated from the 3D ME GRE sequence (pTOF) and conventional TOF-MRA (cTOF), and (b) SWI generated from the 3D ME-GRE and T2*-weighted conventional GRE
Reconstructed SWI versus 2D GRE T2* in diagnostic performance
In the same cohort of subjects, two independent evaluators compared reconstructed SWI and conventional T2* images for lesion conspicuity and diagnostic confidence. For lesion conspicuity, SWI was rated on average significantly higher than that of 2D GRE T2* images (Supplemental Table 2; 4.6 ± 0.7 versus 4.0 ± 0.7, respectively, p < 0.001). For diagnostic confidence, SWI was rated similarly to 2D GRE T2* images (4.1 ± 0.4 versus 4.0 ± 0.72 respectively, p = 0.026). The inter-rater reliability for individual subject’s lesion count was classified as almost perfect in agreement (κ = 0.91, 96% CI 0.8–1.0). More patients were identified to have lesions on SWI than 2D GRE T2* (59% of patients versus 57%, respectively), but this was not statistically significant. A total of 102 lesions over all patients were found on 2D GRE T2* and 110 lesions were found on SWI. An illustrative example of SWI versus 2D GRE T2* images is shown in Supplemental Fig. 2.
Illustrative examples of cTOF versus pTOF
A 53-week-old infant presented with left arm weakness and was subsequently found to have an acute right middle cerebral artery (MCA) infarct on DWI (Fig. 2). pTOF generated from 3D ME-GRE revealed steno-occlusion at right MCA. cTOF revealed similar steno-occlusion at right MCA.

A 53-week old infant with left arm weakness. Acute right MCA infarct is seen on DWI. The pTOF image shows right MCA steno-occlusion, which is also confirmed on cTOF (arrows). Given that 3D ME GRE can generate both pTOF and T2* magnitude image, focal steno-occlusion seen on pTOF can be directly cross-referenced to focal T2* low signal, representing an M1 clot (arrow) on the magnitude image
In another case, a 4-year-old girl was found on eye exam to exhibit morning glory optic disc (Fig. 3). Dysplastic, aneurysmal appearance of bilateral ICA was appreciated on both pTOF and cTOF images; however, peripheral vasculature was better delineated with cTOF in this case. Digital subtraction angiography (DSA) subsequently confirmed aneurysmal dilatation of the left ICA.

A 4-year old girl with morning glory optic disc on eye exam. Both pTOF and cTOF demonstrate dysplastic and aneurysmal appearance of the bilateral ICA (arrows). 3D rotation view from DSA confirms aneurysmal dilatation of the left ICA. Note more peripheral vascular delineation is more robust for cTOF (*) compared to pTOF
Finally, a 6-year-old boy with a history of arteriovenous malformation presented for follow-up (Fig. 4). Ferumoxytol-enhanced T1 SPGR image indicated an abnormal tangle of vessels in the right occipital lobe. This was subsequently confirmed with DSA. pTOF image generated from 3D ME-GRE prior to ferumoxytol injection highlighted abnormal tangle of vessels in a similar fashion to that of cTOF.

A 6-year old boy with arteriovenous malformation. Ferumoxytol-enhanced (Fe-enhanced) T1 SPGR image shows abnormal tangle of vessels in right occipital lobe (arrowhead), which was subsequently confirmed by DSA (not shown). The pTOF generated from 3D ME-GRE prior to Ferumoyxtol injection shows abnormal tangle of vessels (arrows) similar to cTOF
Discussion
This work shows that TOF-MRA (pTOF) generated from single 3D ME-GRE sequence may be a useful alternative to single-sequence conventional TOF-MRA (cTOF) for pediatric neurovascular evaluation. If a dedicated MRA was not initially acquired, but later a question arises regarding potential neurovascular disease, a 3D ME-GRE automated to generate a pTOF could address the clinical question without requiring a repeat scan, potentially reducing additional cost and sedation requirements. In the present study, we found that pTOF can provide information useful for diagnosis of neurovascular pathologies, as compared to conventional cTOF. While pTOF may not be equivalent in performance to pTOF as shown by lower overall diagnostic confidence and poor distal vessel visualization, pTOF may serve as a useful diagnostic adjunct when cTOF images are absent.
Simultaneous generation of TOF-MRA in addition to SWI from a single 3D ME-GRE acquisition (as opposed to acquisition of their single-sequence alternatives) could allow for significant reduction in scan time. Note however that scan time savings could also be achieved through the use of “fast brain” protocols, which (through more efficient acquisition and image processing strategies) shorten the scan time of routine contrast mechanisms such as SPRR, FSE, and DWI [16,17,18,19,20,21,22,23,24,25,26,27]. Another advantage of the 3D ME-GRE sequence is that since the image outputs are naturally co-registered, it can mitigate misregistration that might occur between separate image acquisitions (Fig. 2). For example, since all 3D ME-GRE-derived sequences can more precisely co-localize, a focal T2* clot within a vessel (e.g., M1 or M2 occlusion associated with an MCA infarction) can co-localize to a vascular branch.
While agreement between pTOF and cTOF was high, there were notable discrepancies. Specifically, the reviewers over-called stenotic lesions on pTOF compared with cTOF (92 versus 82 lesions respectively). After consensus review and review of all vascular imaging data (e.g., diagnostic cerebral angiography and CT angiography when available), the 10 additional stenotic lesions detected by pTOF were considered artifacts stemming from signal dropout in the proximal ICA and M1 segments in subjects with prominent T2* susceptibility associated with the paraclinoid bony structures. While such false positives did not significantly affect overall performance of pTOF compared with cTOF, if a potential stenosis of proximal anterior circulation is found on pTOF, a false positive could be mitigated by review of the raw source data.
Another limitation of pTOF may be reduced visualization of more distal vasculature. The readers reported reduced visualization of peripheral cerebral vessels on pTOF as a main source for lower overall diagnostic confidence. In children, due to intrinsic high blood flow and high SNR, cTOF at 3T is capable of flow-related enhancement of the M3 and M4 MCA branches. However, the readers noted that pTOF did not reliably confer signal beyond M1 or M2 MCA branches. Thus, pTOF may more reliably detect proximal vessel diseases such as M1/2 occlusions or moyamoya disease versus more distal neurovascular processes such as reversible cerebral vasoconstriction syndrome or small vessel vasculitis. As our study cohort mainly comprised subjects with proximal vessel disease, we were not able to adequately assess the effectiveness of pTOF in evaluating distal lesions. The loss of distal vessel visualization on pTOF warrants further discussion. The MRA parameters chosen in this study are based on routine standard of care clinical protocol. Thus, the flip angle for the ME-GRE was selected based on what is used for T2* imaging. Future studies are needed to determine the optimal flip angle in ME-GRE which balances T2*-w tissue contrast with adequate background suppression for the TOF. In a similar vein, better depiction of distal vessels could be achieved with multi-slab ME by enhancing in-flow effects, however, at the expense of scan time.
While this study targeted pTOF comparison against cTOF, as one might expect, we also observed higher sensitivity of SWI (generated from a 3D ME-GRE) to T2* lesions when compared against conventional 2D GRE. For example, the blinded reviewers identified 8 more T2* lesions on SWI compared with 2D GRE (110 versus 102 lesions, respectively), albeit not statistically significant. As an illustrative case (Supplemental Fig. 2), siderosis in a patient with prior aneurysmal subarachnoid hemorrhage was not detected by both readers on 2D GRE.
The 3D ME-GRE technique has other potential advantages: it can be further exploited to produce a number of other images with various contrasts (Supplemental Fig. 1). In addition to TOF-MRA and SWI, it is possible to produce T1 images, R2* maps [28,29,30], T2* FLAIR-like (FLAIR*) images [4], field maps and Quantitative Susceptibility Mapping (QSM) images [31,32,33,34,35,36,37,38], myelin water fraction [39], ultra-short TE-like contrast, venous oxygenation maps [40], and (although less validated) p-space [41]. These plural-contrast datasets may have a role for neuroanatomical and neuropathological research and further assist clinical investigations of neurological disorders. Of particular interest is the use of QSM, which utilizes the phase information from a 3D GRE sequence to produce a semi-quantitative contrast in MRI that is directly linked to iron in the brain. This approach has been shown to uniquely characterize anatomical structures [42,43,44,45], as well as microhemorrhages and high-resolution blood volume [43, 46, 47]. Future studies could examine clinical utility of these additional contrast mechanisms extracted from a single-sequence approach.
Conclusion
In summary, we investigated the use of a TOF-MRA generated in addition to SWI from a single 3D ME-GRE sequence, and compared it to independent acquisition of conventional MRA. pTOF from the 3D ME-GRE sequence offered diagnostic information that was comparable to conventional TOF-MRA. Thus, in the event conventional MRA was not acquired but a clinical question arises regarding potential neurovascular lesion, TOF-MRA images can be retroactively processed from a 3D ME-GRE sequence to assist neurovascular assessment.
Availability of data
Upon request
References
Nishimura DG (1990) Time-of-flight MR angiography. Magn Reson Med 14:194–201. https://doi.org/10.1002/mrm.1910140206
Graves MJ (1997) Magnetic resonance angiography. Br J Radiol 70:6–28. https://doi.org/10.1259/bjr.70.829.9059290
Du YP, Jin Z (2008) Simultaneous acquisition of MR angiography and venography (MRAV). Magn Reson Med 59:954–958. https://doi.org/10.1002/mrm.21581
Luo J, Jagadeesan BD, Cross AH, Yablonskiy DA (2012) Gradient echo plural contrast imaging--signal model and derived contrasts: T2*, T1, phase, SWI, T1f, FST2*and T2*-SWI. Neuroimage 60:1073–1082. https://doi.org/10.1016/j.neuroimage.2012.01.108
Deistung A, Dittrich E, Sedlacik J, Rauscher A, Reichenbach JR (2009) ToF-SWI: simultaneous time of flight and fully flow compensated susceptibility weighted imaging. J Magn Reson Imaging 29:1478–1484. https://doi.org/10.1002/jmri.21673
Haacke EM, Makki M, Ge Y, Maheshwari M, Sehgal V, Hu J, Selvan M, Wu Z, Latif Z, Xuan Y, Khan O, Garbern J, Grossman RI (2009) Characterizing iron deposition in multiple sclerosis lesions using susceptibility weighted imaging. J Magn Reson Imaging 29:537–544. https://doi.org/10.1002/jmri.21676
Mittal S, Wu Z, Neelavalli J, Haacke EM (2009) Susceptibility-weighted imaging: technical aspects and clinical applications, part 2. AJNR Am J Neuroradiol 30:232–252. https://doi.org/10.3174/ajnr.A1461
Haacke EM, Cheng NYC, House MJ et al (2005) Imaging iron stores in the brain using magnetic resonance imaging. Magn Reson Imaging 23:1–25. https://doi.org/10.1016/j.mri.2004.10.001
Ogg RJ, Langston JW, Haacke EM, Steen RG, Taylor JS (1999) The correlation between phase shifts in gradient-echo MR images and regional brain iron concentration. Magn Reson Imaging 17:1141–1148. https://doi.org/10.1016/s0730-725x(99)00017-x
Petridou N, Wharton SJ, Lotfipour A, Gowland P, Bowtell R (2010) Investigating the effect of blood susceptibility on phase contrast in the human brain. Neuroimage 50:491–498. https://doi.org/10.1016/j.neuroimage.2009.12.052
Sedlacik J, Kutschbach C, Rauscher A, Deistung A, Reichenbach JR (2008) Investigation of the influence of carbon dioxide concentrations on cerebral physiology by susceptibility-weighted magnetic resonance imaging (SWI). Neuroimage 43:36–43. https://doi.org/10.1016/j.neuroimage.2008.07.008
Trofimova A, Kadom N (2019) Added value from abbreviated brain MRI in children with headache. Am J Roentgenol 212:1348–1353. https://doi.org/10.2214/ajr.18.20439
Skare S, Sprenger T, Norbeck O, Rydén H, Blomberg L, Avventi E, Engström M (2017) A 1-minute full brain MR exam using a multicontrast EPI sequence. Magn Reson Med 79:3045–3054. https://doi.org/10.1002/mrm.26974
Ogawa S, Lee T-M, Nayak AS, Glynn P (1990) Oxygenation-sensitive contrast in magnetic resonance image of rodent brain at high magnetic fields. Magn Reson Med 14:68–78. https://doi.org/10.1002/mrm.1910140108
Reichenbach JR, Venkatesan R, Schillinger DJ, Kido DK, Haacke EM (1997) Small vessels in the human brain: MR venography with deoxyhemoglobin as an intrinsic contrast agent. Radiology 204:272–277. https://doi.org/10.1148/radiology.204.1.9205259
Nael K, Khan R, Choudhary G et al (2014) Six-minute magnetic resonance imaging protocol for evaluation of acute ischemic stroke. Stroke 45:1985–1991. https://doi.org/10.1161/strokeaha.114.005305
Miller JH, Walkiewicz T, Towbin RB, Curran JG (2009) Improved delineation of ventricular shunt catheters using fast steady-state gradient recalled-echo sequences in a rapid brain MR imaging protocol in nonsedated pediatric patients. Am J Neuroradiol 31:430–435. https://doi.org/10.3174/ajnr.a1866
Missios S, Quebada PB, Forero JA, Durham SR, Pekala JS, Eskey CJ, Duhaime AC (2008) Quick-brain magnetic resonance imaging for nonhydrocephalus indications. J Neurosurg Pediatr 2:438–444. https://doi.org/10.3171/ped.2008.2.12.438
Tekes A, Senglaub SS, Ahn ES, Huisman TAGM, Jackson EM (2018) Ultrafast brain MRI can be used for indications beyond shunted hydrocephalus in pediatric patients. Am J Neuroradiol. https://doi.org/10.3174/ajnr.a5724
Lindberg DM, Stence NV, Grubenhoff JA, Lewis T, Mirsky DM, Miller AL, O’Neill BR, Grice K, Mourani PM, Runyan DK (2019) Feasibility and accuracy of fast MRI versus CT for traumatic brain injury in young children. Pediatrics 144:e20190419. https://doi.org/10.1542/peds.2019-0419
Ramgopal S, Karim SA, Subramanian S, Furtado AD, Marin JR (2020) Rapid brain MRI protocols reduce head computerized tomography use in the pediatric emergency department. BMC Pediatr 20:14. https://doi.org/10.1186/s12887-020-1919-3
Patel DM, Tubbs RS, Pate G, Johnston JM, Blount JP (2014) Fast-sequence MRI studies for surveillance imaging in pediatric hydrocephalus. J Neurosurg Pediatr 13:440–447. https://doi.org/10.3171/2014.1.peds13447
Iskandar BJ, Sansone JM, Medow J, Rowley HA (2004) The use of quick-brain magnetic resonance imaging in the evaluation of shunt-treated hydrocephalus. J Neurosurg Pediatr 101:147–151. https://doi.org/10.3171/ped.2004.101.2.0147
Niederhauser BD, McDonald RJ, Eckel LJ et al (2013) Retrospective review of rapid pediatric brain MR imaging at an academic institution including practice trends and factors affecting scan times. Am J Neuroradiol 34:1836–1840. https://doi.org/10.3174/ajnr.a3510
Flom L, Fromkin J, Panigrahy A, Tyler-Kabara E, Berger RP (2016) Development of a screening MRI for infants at risk for abusive head trauma. Pediatr Radiol 46:519–526. https://doi.org/10.1007/s00247-015-3500-z
Kralik SF, Yasrebi M, Supakul N, Lin C, Netter LG, Hicks RA, Hibbard RA, Ackerman LL, Harris ML, Ho CY (2017) Diagnostic performance of ultrafast brain MRI for evaluation of abusive head trauma. Am J Neuroradiol 38:807–813. https://doi.org/10.3174/ajnr.a5093
Yue EL, Meckler GD, Fleischman RJ, Selden NR, Bardo DME, Chu O'Connor AK, Vu ET, Fu R, Spiro DM (2015) Test characteristics of quick brain MRI for shunt evaluation in children: an alternative modality to avoid radiation. J Neurosurg Pediatr 15:420–426. https://doi.org/10.3171/2014.9.peds14207
Khalil M, Enzinger C, Langkammer C, Tscherner M, Wallner-Blazek M, Jehna M, Ropele S, Fuchs S, Fazekas F (2009) Quantitative assessment of brain iron by R2* relaxometry in patients with clinically isolated syndrome and relapsing–remitting multiple sclerosis. Mult Scler J 15:1048–1054. https://doi.org/10.1177/1352458509106609
Yan S-Q, Sun J-Z, Yan Y-Q, Wang H, Lou M (2012) Evaluation of brain iron content based on magnetic resonance imaging (MRI): comparison among phase value, R2* and magnitude signal intensity. PLoS One 7:e31748. https://doi.org/10.1371/journal.pone.0031748
Liu Z, Liao H, Yin J, Li Y (2013) Using R2* values to evaluate brain tumours on magnetic resonance imaging: preliminary results. Eur Radiol 24:693–702. https://doi.org/10.1007/s00330-013-3057-x
Salomir R, de Senneville BD, Moonen CTW (2003) A fast calculation method for magnetic field inhomogeneity due to an arbitrary distribution of bulk susceptibility. Concepts Magn Reson 19B:26–34. https://doi.org/10.1002/cmr.b.10083
de Rochefort L, Liu T, Kressler B, Liu J, Spincemaille P, Lebon V, Wu J, Wang Y (2009) Quantitative susceptibility map reconstruction from MR phase data using bayesian regularization: validation and application to brain imaging. Magn Reson Med 63:194–206. https://doi.org/10.1002/mrm.22187
Kressler B, de Rochefort L, Liu T et al (2010) Nonlinear regularization for per voxel estimation of magnetic susceptibility distributions from MRI field maps. IEEE Trans Med Imaging 29:273–281. https://doi.org/10.1109/TMI.2009.2023787
de Rochefort L, Brown R, Prince MR, Wang Y (2008) Quantitative MR susceptibility mapping using piece-wise constant regularized inversion of the magnetic field. Magn Reson Med 60:1003–1009. https://doi.org/10.1002/mrm.21710
Schofield MA, Zhu Y (2003) Fast phase unwrapping algorithm for interferometric applications. Opt Lett 28:1194. https://doi.org/10.1364/ol.28.001194
Liu T, Khalidov I, de Rochefort L, Spincemaille P, Liu J, Tsiouris AJ, Wang Y (2011) A novel background field removal method for MRI using projection onto dipole fields (PDF). NMR Biomed 24:1129–1136. https://doi.org/10.1002/nbm.1670
Schweser F, Deistung A, Lehr BW, Reichenbach JR (2011) Quantitative imaging of intrinsic magnetic tissue properties using MRI signal phase: an approach to in vivo brain iron metabolism? Neuroimage 54:2789–2807. https://doi.org/10.1016/j.neuroimage.2010.10.070
Liu J, Liu T, de Rochefort L, Ledoux J, Khalidov I, Chen W, Tsiouris AJ, Wisnieff C, Spincemaille P, Prince MR, Wang Y (2012) Morphology enabled dipole inversion for quantitative susceptibility mapping using structural consistency between the magnitude image and the susceptibility map. Neuroimage 59:2560–2568. https://doi.org/10.1016/j.neuroimage.2011.08.082
Lenz C, Klarhöfer M, Scheffler K (2011) Feasibility of in vivo myelin water imaging using 3D multigradient-echo pulse sequences. Magn Reson Med 68:523–528. https://doi.org/10.1002/mrm.23241
Fan AP, Evans KC, Stout JN, Rosen BR, Adalsteinsson E (2015) Regional quantification of cerebral venous oxygenation from MRI susceptibility during hypercapnia. Neuroimage 104:146–155. https://doi.org/10.1016/j.neuroimage.2014.09.068
Liu C, Li W (2013) Imaging neural architecture of the brain based on its multipole magnetic response. Neuroimage 67:193–202. https://doi.org/10.1016/j.neuroimage.2012.10.050
Duyn JH, van Gelderen P, Li T-Q, de Zwart JA, Koretsky AP, Fukunaga M (2007) High-field MRI of brain cortical substructure based on signal phase. Proc Natl Acad Sci U S A 104:11796–11801. https://doi.org/10.1073/pnas.0610821104
Marques JP, Maddage R, Mlynarik V, Gruetter R (2009) On the origin of the MR image phase contrast: an in vivo MR microscopy study of the rat brain at 14.1 T. Neuroimage 46:345–352. https://doi.org/10.1016/j.neuroimage.2009.02.023
Rauscher A, Sedlacik J, Deistung A, Mentzel HJ, Reichenbach JR (2006) Susceptibility weighted imaging: data acquisition, image reconstruction and clinical applications. Z Med Phys 16:240–250. https://doi.org/10.1078/0939-3889-00322
Zhong K, Leupold J, von Elverfeldt D, Speck O (2008) The molecular basis for gray and white matter contrast in phase imaging. Neuroimage 40:1561–1566. https://doi.org/10.1016/j.neuroimage.2008.01.061
Langkammer C, Liu T, Khalil M, Enzinger C, Jehna M, Fuchs S, Fazekas F, Wang Y, Ropele S (2013) Quantitative susceptibility mapping in multiple sclerosis. Radiology 267:551–559. https://doi.org/10.1148/radiol.12120707
Langkammer C, Schweser F, Krebs N, Deistung A, Goessler W, Scheurer E, Sommer K, Reishofer G, Yen K, Fazekas F, Ropele S, Reichenbach JR (2012) Quantitative susceptibility mapping (QSM) as a means to measure brain iron? A post mortem validation study. Neuroimage 62:1593–1599. https://doi.org/10.1016/j.neuroimage.2012.05.049
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Preliminary results from this article was presented at the American Society of Neuroradiology 2016 Annual Meeting, May 21-26, Washington, DC. Funding support was provided by ASNR Comparative Effectiveness Grant and NIH grant 1R21HD08380301A1.
Conflict of interest/Competing interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Stanford University Institutional Review Board in the Research Compliance Office (RCO). The study protocol number is 44683.
Informed consent
As the study was entirely retrospective in nature, informed consent for subjects in this study were not required.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
BAL and YH are co-first authors.
Electronic supplementary material
ESM 1
(DOCX 2.32 MB)
Rights and permissions
About this article

Cite this article
Lanzman, B.A., Huang, Y., Lee, E.H. et al. Simultaneous time of flight-MRA and T2* imaging for cerebrovascular MRI. Neuroradiology 63, 243–251 (2021). https://doi.org/10.1007/s00234-020-02499-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00234-020-02499-5