
Abstract
Traumatic brain injury (TBI) is one of the main causes of death and disability in both civilian and military population. TBI may occur via a variety of etiologies, all of which involve trauma to the head. However, the neuroprotective drugs which were found to be very effective in animal TBI models failed in phase II or phase III clinical trials, emphasizing a compelling need to review the current status of animal TBI models and therapeutic strategies. No single animal model can adequately mimic all aspects of human TBI owing to the heterogeneity of clinical TBI. However, due to the ethical limitations, it is difficult to precisely emulate the TBI mechanisms that occur in humans. Therefore, many animal models with varying severity and mechanisms of brain injury have been developed, and each model has its own pros and cons in its implementation for TBI research. These challenges pose a need for study of continued TBI mechanisms, brain injury severity, duration, treatment strategies, and optimization of animal models across the neurotrauma research community. The aim of this review is to discuss (1) causes of TBI, (2) its prevalence in military and civilian population, (3) classification and pathophysiology of TBI, (4) biomarkers and detection methods, (5) animal models of TBI, and (6) the advantages and disadvantages of each model and the species used, as well as possible treatments.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Traumatic brain injury is a major public health crisis Traumatic brain injury (TBI) is a disruption of normal functions of the brain caused by an external force to the head, and has been recognized as a global public health crisis (CDC 2020; NINDS 2020). Approximately, 50 million people suffer from brain injury every year, with increase in prevalence by 8.4% between 1990 and 2016, and 80% of the TBI comes from the developing countries (GBD 2019). According to a CDC report from 2008 to 2014, the highest rates of TBI are observed in children < 5 years (1592/100 000 population), and > 75 years (2232/100 000 population). TBI-related emergency department visits were approximately 2.5 million followed by 282,000 TBI-related hospitalizations, and 56,000 TBI-related deaths each year, contributing 30% to all injury-related deaths (CDC 2019). Several factors have been identified for the increased TBI cases over the last several years, including our awareness about the acute and chronic neurodegenerative effects of sport-related concussion, and the brain injuries sustained by approximately 20% of U.S. military service members deployed to Iraq (Operation Iraqi Freedom — OIF), and Afghanistan (Operation Enduring Freedom — OEF) wars (Elder et al. 2019).
The leading causes of TBI Falls. According to the data from the CDC and National Institute of Neurological Disorders (NINDS), falls are the most common causes of TBI, and occur most frequently among the youngest and oldest age groups. From 2006 to 2010 alone, falls caused more than half (55 percent) of TBIs among children aged 14 and younger. Among Americans aged 65 and older, falls accounted for more than two-thirds (81 percent) of all reported TBIs. Blunt trauma. Accidents that involve the head being struck by or against an object, particularly sports-related injuries (contact TBI), are a major cause of TBI. Anywhere from 1.6 million to 3.8 million sports- and recreation-related TBIs are estimated to occur in the United States annually. Vehicle-related injuries. Pedestrian involved in traffic accidents, as well as speed-driven accidents involving motor vehicles and bicycles, are also very common causes of TBI. In young adults aged 15–24 years and > 65 years, motor vehicle accidents are the most likely cause of TBI. Assaults/violence. Assaults include abuse-related TBIs, such as head injuries that result from domestic violence or shaken baby syndrome, and gunshot wounds to the head. TBI-related deaths in children age 4 and younger are most likely the result of assault. Explosions/blasts. These non-contact types of blast traumatic brain injuries (bTBI) are caused by blast trauma from roadside bombs, became a common injury to service members in recent military conflicts. The majority of these bTBIs were classified as mild head injuries. Regardless of its cause, TBI often results in physical, cognitive and behavioral impairments, leading to temporary or permanent dysfunction (Gwarzo et al. 2021).
Classification of TBI TBI can generally be classified as either closed head injury (CHI), which does not involve skull fracture. In contrast penetrating brain injury (PBI) often result in skull fracture due to gun- shot wound or sharp objects. PBI is less common than CHI, but constitutes the most severe form of TBI. CHI is the most common type of TBI which is mainly caused by an external impact from sudden, violent motion that does not lead to skull fracture. In particular, CHI is more common in military and sports population than general civilians; caused by either a direct blow to the head, face, neck or elsewhere on the body with an “impulsive” force transmitted to the head (Silverberg and Iverson 2013; Theadom et al. 2020), and in some cases, by bullets or projectiles impacting the Kevlar helmet (Lindquist et al. 2017; Missliwetz and Wieser 1989).
Types of CHI include concussion, contusion, diffuse axonal injury, and intracranial hematoma (epidural hematoma, subdural hematoma, subarachnoid hemorrhage, and intra-parenchymal hemorrhage) (Hoogenboom et al. 2019).
In terms of severity, TBIs can be classified into two broad categories: A Mild TBI: The individual is usually awake. The symptoms may include a brief loss of consciousness, confusion, headache, disorientation, and memory loss (Silverberg et al. 2020). A Severe TBI: There is a loss of consciousness for several hours, or even weeks, and could result in permanent disability. The severity of TBI in humans can be determined by means of the Glasgow Coma Score (GCS), which is based the type of eye opening, speech, and motor response (Teasdale and Jennett 1974). A GCS of 3–8 is categorized as a severe brain injury, 9–12 moderate, and 13–15 a mild brain injury. However, the verbal evaluation score poses a critical challenge in infants, preverbal children. In addition, most of the patients with mild TBI recover in few weeks, but approximately 10–15 percent of TBI patients do not recover even after 1 year, and may continue to have chronic and often debilitating post-concussive signs resulting in neurodegenerative consequences including dementia, Alzheimer’s and Parkinson’s diseases (Graham and Sharp 2019). Unfortunately, only few therapeutic interventions have been successfully translated to the clinic. These reasons behind the failures of drug trials are (1) our inadequate knowledge about the basic mechanisms of TBI which can be translated to human brain injury mechanisms, and (2) lack of brain injury mechanisms targeted effective therapeutic strategies.
The need for animal models to study TBI Due to the ethical implications and logistical issues associated with human studies, the vast majority of TBI research is conducted using animal models. Animal TBI models have been employed using a variety of species including cats, dogs and non-human primates to study the underlying pathophysiology, genotype–phenotype relationships, long-term outcomes, and proof-of-concept models in brain injury research (Wojnarowicz et al. 2017). However, the use of rodent TBI models has dominated the laboratory research due to (1). Simplicity of performing surgery, (2). Large number of animals can be included in each group to provide adequate statistical data analysis and detect the true differences between the groups, and (3). Low cost of purchasing animals, handling and lodging. In contrast, experiments in large animals involve (1). Controversial ethical issues, (2). The requirement of complex surgical facilities for post-operative care, (3). Difficulty in performing behavioral testing, (4). The participation of experienced veterinarian staff, and (5). Abundant funding.
Animal models of focal and diffuse injuries
During TBI, the brain damage can be either focal (confined to one localized area of the brain) and/or diffuse (spread in more than one areas of the brain). These focal and diffuse types of TBI are common in sports and military population. As shown in Fig. 1, Using rats and mice TBI models, brain injury has been induced in three complementary settings: focal impact, diffuse impact, and non-impact TBI using a well-characterized rotational acceleration device to impart a single rapid (12–20 ms) acceleration-deceleration rotation models. Focal impact brain injury animal models are further divided into (1) weight drop (WD), (2) fluid percussion (FP), and (3) controlled cortical impact (CCI) models. The focal injury animal model is best for studying TBI caused by direct blunt trauma. In this method, a craniotomy is mostly performed to expose the dura. Using a rod with computer guidance, the exposed tissue is subject to blunt force. The depth and force of the impact is measured (Dixon et al. 1991). This method is called the controlled cortical impact (CCI) brain injury.

Traumatic brain injury, classification and evaluation: In animals, TBI can be induced by CI, weight drop method, FPI, CHIMERA, blast tube (in closed lab environment) or blats explosives in open spaces. Most of these brain injuries are classified as primary (direct effect of an object on brain), or secondary, injury due to the progression of neuronal cell death mechanisms. Blast TBIs are classified as Primary, secondary, Tertiary and Quaternary. Primary bTBI is caused mainly by the direct effect of blast overpressure on tissue. Secondary bTBI is caused by the flying objects from bomb explosion leading to the multiple injuries and bleeding. Tertiary bTBI is caused by the high-energy explosions; occurs when people fly through the air and strike other objects. Quaternary bTBI comprises all other injuries caused by explosions of improvised explosive devices. Severity of TBI can be evaluated by blood-based biomarkers, neurobehavioral tests, mortality rate and immunohistochemistry
Advantages of CCI over other TBI models
The impact of injury can be better controlled, and reduces the risk of rebound injury. Using the CCI model of TBI, researchers are able to control the depth, duration or dwell time, and velocity of injury as well as choose what size and shape of tip to use. The velocity of the piston is monitored by a sensor and can be controlled to promote uniform injury across test animals. These measurements allow the researchers to create a more reliable and reproducible pattern of injury leading to a fewer variable data set. Cognitive deficits after CCI are highly dependent to both the depth of deformity and the impact velocity. The impairments can persist for up to 1 year and associated with brain atrophy and progressive reduction in cerebral blood flow. Mild-to-moderate TBI can cause transient interruption of BBB integrity and thereby provide a mechanism for subsequent brain injury (Hoogenboom et al. 2019). Neuro-immune changes are a probable consequence of BBB alterations and may be an important initial component of long-term cognitive, sensory–motor and behavioral impairments associated with TBI.
Disadvantages of CCI over other TBI models
In CCI, following a midline incision to expose the skull, a craniotomy of 5 mm diameter (injury window) is required, which is an invasive procedure that causes several complications including the disruption of the blood–brain barrier (BBB) induced by tissue shearing. This could produce immediate neuropathology due to hemorrhage and ischemia. And disruption of the tight junctions and alteration of the activation states of BBB cells (endothelium, astrocytes, microglia, pericytes and neurons) could result in acute or chronic neurodegenerative conditions. These changes may also manifest in decreased cognitive functioning (Dixon et al. 1987, 1991). Even moderate elevations in intracranial pressure (ICP) after CCI in mice without decompressive craniectomy were associated with increased axonal injury and white matter atrophy indicating the damaging effects of CCI alone on the progression of brain injury mechanisms (Friess et al. 2015).
Weight drop method of inducing TBI
Noticing the above criticism, the weight drop (WD) method of inducing TBI was developed to create both focal and diffuse brain injury studies in rats and mice. In the WD model, the injury is produced by a free-falling weight guided in a tube that is dropped directly on the cranium, the skull, or skull with helmet. The helmet is also a method to diffuse the injury and producing a contusion (Dail et al. 1981; Feeney et al. 1981; Morales et al. 2005). The severity of the injury can be adjusted by the height and mass of the weight dropped. Marmarou et al. 1994 refined his widely used weight drop TBI model (Marmarou et al. 1994). Marmarou’s Sprague Dawley (SD) rat model is very similar to the Shohami model that uses a brass weight dropped through a Plexiglas tube from an experimentally defined height. The weight can be increased from 20 gm up to 200 gm in 50-gm increments by attaching extra 50-gm brass weights. The weight drop height can be increased up to 2 m. Instead of placing the rats head on a firm plastic disk, the head rests on a foam bed, to prevent skull fracture. In addition, the central portion of the exposed skull is covered with a metal helmet (metal disk 10 mm diameter, 3 mm thick), which acts as the impact site for the weight, and this also helps prevent skull fracture. To better propagate diffused axonal injury (DAI) in models, the group used the weight drop model as a base, but instead of fixing the cranium of the animal, the skull was allowed to rotate downward upon impact. It is theorized that this downward motion may contribute to a more widespread and reproducible pattern of DAI (Marmarou et al. 1994).
Advantages of weight drop method over other TBI models
An advantage of WD models is that it is cost-effective and relatively easy to use. The magnitude of tissue damage exerted in this model is regulated by simple force and acceleration calculations using the mass of the weight and distance it is traveling. Weight drop models are used primarily to recreate mild injuries and generate a diffuse pattern of injury (Ma et al. 2019). This model has been demonstrated to induce varying degrees of diffuse axonal injury, depending on the amount of impact energy produce to generate intracranial pressure, subarachnoid and ventricular hemorrhage, as well as brainstem petechial bleeding persisting vasoconstriction of cerebral micro vessels and hypo-perfusion of the cerebral microcirculation (Logsdon et al. 2015). The lesions produced by dropping a 450 gm weight form 2 m were categorized as “severe” TBI, comparable to a human GSC score of < 8.
Disadvantages of weight drop method over other TBI models
Limitations of weight drop method exist, such as unintentional skull fracture, risk of a second rebound injury, and inaccuracy with regard to the impact site (Rostami 2012; Briones 2015). Despite the several advantages of this model, there is skepticism that DAI cannot be produced from the acceleration of the head alone (Li et al. 2011). In addition, there is the argument that the differential in size and relative anatomy between rodent and human skulls cannot accurately reflect how acceleration forces interact upon the human skull. Other criticisms of this model include the lack of reproducibility as well as a noted increased mortality rate seen in subjects who did not receive ventilatory support (Xiong et al. 2013). Finally, the accuracy of tissue deformation using this model has been questioned based on the variable rebound impact and variable impact velocity due to differences in machinery set up.
The fluid percussion injury (FPI) method of inducing TBI
In the FPI model, the primary brain injury is inflicted by a pendulum striking a piston at the end of a tube filled with fluid creating an fluid impulse that hits the exposed dura through a Luer lock implanted surgically through a craniotomy (Thompson et al. 2005). For detailed video of FPI procedure, please refer to (Alder et al. 2011).There are several variations in the piston device used, including compressed nitrogen, electromagnetic, or pneumatically driven pistons (Bodnar et al. 2019). The percussion briefly displaces and deforms the brain tissue, and the severity of the injury depends on the strength of the pulse. Fluid percussion can induce mild, moderate, or severe brain injury in mice and rats of any age.
Fluid percussion injury (FPI) models present the conditions of clinical TBI without skull fracture. FPI can efficiently replicate intracranial hemorrhage, brain swelling, and progressive gray matter damage. The midline FPI (MFPI) model produces a diffuse, concussive-like TBI in rodents, whereas lateral FPI (LFPI) produces a mixed focal and diffuse injury. To this end, the primary FPI neuropathology is diffuse axonal injury, rather than noticeable cell death.
However, there are continuous and chronic cell death mechanisms generated around glial cells at the impact site leading to progressive neurodegeneration beginning seconds after injury and lasting years post-injury. This occurs predominantly in the cortex, hippocampus, thalamus, striatum, and amygdala (Bramlett and Dietrich 2002; Cernak 2005; Liu et al. 2010). This differential in location of regional neuronal loss appears to produce neurobehavioral impairments, such as changes in reflexes and cognitive function. Neurobehavioral deficits assessed are commonly motor, cognition, and depression/anxiety behaviors using a variety of different testing methods (Bodnar et al. 2019).
Advantages of fluid percussion method over other TBI models
Among the TBI models, FPI is the most established and commonly used model to evaluate focal, diffuse or mixed focal and diffuse brain injury. It is reproducible and is standardized to allow for the manipulation of brain injury severity, such as mild, moderate and severe TBI. The fluid-percussion injury model enabled the researchers to study possible behavioral outcomes to perform large-scale studies of experimental therapeutics to obtain meaningful statistically significant results. Fluid percussion was later adapted for use in ferrets, pigs, and smaller animals, such as rats and mice, providing the means of studying TBI in experimentally and genetically altered animals. Thus, FPI model has since become the most well-characterized and extensively used model of experimental TBI (Lyeth 2016). FPI also recapitulates brain injuries observed in humans, thus rendering it clinically relevant, and allows for exploration of novel therapeutics for clinical translation.
Disadvantages of fluid percussion method over other TBI models
In this model, it becomes critical to accurately place the craniotomy to ensure reproducibility. The need for craniotomy in FPI is a disadvantage, not only because of the equipment placement reproducibility, complexity of procedure and instruments, but also because it causes pathology independent from TBI. Therefore, its use for studying CHI is inappropriate. Another weakness of this FPI model is the lack of any produced fracture of the skull, thus reducing its accuracy in recreation of moderate and severe TBI events (Xiong et al. 2013). Additionally, the mortality of animals in FPI is higher than others due to a compromised brainstem and resulting apnea (Cernak 2005).
All three above-mentioned techniques of generating TBI in rats and mice are known to cause a deformity in the underlying cortex, resulting in cortical tissue loss, hemorrhage, axonal injury, concussion, contusion and BBB dysfunction similar to those seen in patients (Chen et al. 1996; Schmidt and Grady 1993; Whalen et al. 1998; Xiong et al. 2013). CCI is considered a superior focal impact model, because it provides better control over factors, such as the duration and velocity of impact, and the depth of resulting damage in the brain, and also eliminates the risk of a rebound injury (Briones 2015; Rostami et al. 2012). A limitation of these CCI, WD and FPI animal TBI models is that the injuries are commonly induced by direct contact with the brain through a craniotomy, while the animal’s head is immobilized, conditions which typically do not characterize human brain injury. Various researchers have tried to overcome these limitations by designing the following Closed-head impact model of engineered rotational acceleration (CHIMERA).
Closed-head impact model of engineered rotational acceleration (CHIMERA)
The recently developed nonsurgical CHIMERA mice/rat model of TBI requires only isoflurane anesthesia. This model enables immediate neurological severity evaluations using loss of righting reflex (LRR), Neurological Severity Score (NSS), and chronic behavioral changes including the passive avoidance (PA), Barnes maze (BM), elevated plus maze (EPM) and rotarod (RR) tasks (Tucker et al. 2021). CHIMERA is ideal for studies investigating multiple impacts as well as the long-term consequences of impact TBI, which involves impact to the intact unrestrained head can overcome this limitation (Namjoshi et al. 2013). The chimera model has been used to produce precisely controlled injuries, and allows for kinematic analysis of head movement at the time of impact, which can be correlated with behavioral, histological and biochemical outcomes (Namjoshi et al. 2017). After injury, damage to the brain tissue can be evaluated with various markers to determine injury severity and its progression over time.
Rodent models of blast traumatic brain injury (bTBI)
The primary and secondary effects of bTBI can be induced in animals through live-fire testing, compressed-gas shock tubes, combustion shock tubes, and small explosion shock tubes in small animals, such as rats and mice, and large animals including pig (Axelsson et al. 2000; Rubovitch et al. 2011; Yarnell et al. 2013). Number of shock-tube models for bTBI in rats and mice have been developed to represent ‘mild–moderate–severe’ brain injury scale using a single or a set of repeat blast intensities ranging from 10 PSI to 20 PSI. Despite the recent advancement of bTBI research in animal model, there is lack of consensus and information about the rationale for selection of range of blast overpressure and impulse as accepted predictors of bTBI because it is difficult to replicate human bTBI which is mainly caused due to the detonation of an improvised explosive device (IED) causing primary, secondary and tertiary mechanisms of bTBI.
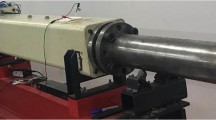
A small animal model of rats and mice using an overpressure blast to the head has recently been described (Guley et al. 2016). This system also uses blast overpressure to create a focal closed head mild TBI in mice. In anesthetized mice and rats, the body and head are both cushioned and secure allowing for minimal movement and acceleration–deceleration forces to be applied to the animal. Higher psi blasts can be applied to create higher levels of injury and subsequent neurological deficits. As shown in Fig. 2, the shock tube model is a two-chambered model which uses a compression chamber and an expansion chamber separated by a diaphragm. When the compression chamber is pressurized, the membrane ruptures, and the expansion chamber carries high-velocity pressure waves. The thickness of the membrane dictates the peak overpressure that is generated making injury highly reproducible (Long et al. 2009). The mechanism of injury is based on the movement of the brain inside the skull caused by rapidly rotating the head in a closed head animal model (Elder and Cristian 2009). The location of the animal in the shock tube creates different mechanical loading. This model has been used in a variety of animals including rodents, swine, and primates and is known to cause DAI, edema, and ischemia of tissue (Garman et al. 2011; Ryu et al. 2014).

Blast-tube for laboratory use. The Advanced Blast Simulator consists of a high-pressure driver, transition section, test section, and end wave eliminator/muffler. The pressure driver is 6 in × 24 in × 11 in the shock tube. The transition section is designed to gradually widen the blast wavefront planar when it arrives at the test section. The anesthetized rat is placed within the driver chamber at 60 cm from the Mylar membrane while breathing room air. When compressed air is used, the normal operating pressure in the high -pressure drive is about 40 – 160 psi and the peak pressure of the blast is about 6 – 16 psi at the test section
Advantages of blast injury method over other TBI models
Practical and safety concerns make the shock tube the most frequently used model of blast injury (Agoston and Kamnaksh 2015). This model is useful as it allows precise control of blast wave intensity and thus more reproducibility than explosion modeling; the energy created does not decay like field explosion (Reneer et al. 2011; Zhu et al. 2013). This model also minimizes the ocular and head acceleration blast effects unlike other closed head models, and works to eliminate the contribution from head acceleration, lung damage, cardiovascular pressure surges, or injury to other structures from secondary and tertiary blast injuries. It has been found to recapitulate the sensory, motor and emotional deficits seen after mild bTBI in humans. Overpressure in blast results in complex structural, cellular and molecular changes as well as axonal pathologies (Wojnarowicz et al. 2017).
Disadvantages of blast injury method over other TBI
Challenges are encountered when considering differences between a given animal and humans in respect to criteria, such as brain surface, geometry, white/gray ratios and size. When considering the mass of the human brain versus the brain of a rodent model, there is a differential in the mass effect created during a dynamic injury. In a smaller brain, a similar force would create less of a strain. This leads to the need to scale up injuries in rodents to create a similar effect (Margulies et al. 1990). Shock tube methods have not been standardized, with variations occurring in explosive used, tube design, species, location in the tube, body shielding, and head mobility (Albert-Weißenberger et al. 2012). Shock tube models often have accompanying hypoxia, blood pressure surges from compression of lungs, heart and aorta and resultant blood vessel damage. bTBI is rarely an isolated injury and is often accompanied by other injuries, such as burns, limb amputation and shock (Earle et al. 2007). Because of this, there is interest in creating polytrauma models to incorporate the added complexities. Field models are a more complex recreation of bTBI that has the potential to recreate primary through quaternary injury. However, polytrauma models are complicated when considering incorporating seizures, post-traumatic stress disorder (PTSD) and depression, three very relevant comorbidities (Earle et al. 2007).
Outcomes of brain injury are dependent on mimicking the known consequences of bTBI severity and duration on human neuropathology. However, the limited knowledge of human neuropathology making it often necessary to instead focus on physical and neurobehavioral conditions associated with TBI. Other differences in rodent models versus human injury become apparent when trying to model repeated mild bTBI as one must consider the temporal differences in animal pathology versus humans. For example, the period of increased vulnerability is measured in hours in rodents as compared to days in humans (Povlishock 2013). Additionally, the classification of mild, moderate and severe injury in animal models of TBI is non-standardized (Bodnar et al. 2019).
In summary, while each model has its own unique advantages, it is important to note that no injury model accurately reproduces the complete spectrum of pathologies observed in human TBI. Among the three commonly used TBI animal models are, such as fluid percussion, cortical impact and weight drop/impact acceleration. The fluid percussion device produces an injury through a craniectomy by applying a brief fluid pressure pulse on to the intact dura. Conversely, cortical impact injury delivers mechanical energy to the intact dura via a rigid impactor under pneumatic pressure. The weight drop/impact model is characterized by the fall of a rod with a specific mass on the closed skull.
Also, these animal TBI models require the use of anesthetic agents at the time of injury for ethical reasons. Since certain anesthetics, such as isofluorane and ketamine, have been shown to be neuroprotective, improving functional and histological outcomes in TBI models when present at the time of injury (Rowe et al. 2013; Statler et al. 2000, 2006). This approach may contribute to reduced clinical translation as patients are devoid of anesthetic agents at the time of injury.
Pathophysiological mechanisms of TBI
Metabolic and ionic disturbances in TBI
The intracellular cascade after head injury is extremely complex and involves fluctuations in metabolic, inflammatory, neuroendocrine pathways and ionic potentials. These fluctuations have been shown to produce deleterious impacts upon cellular plasticity, immune-excitotoxicity, intracellular calcium and binding proteins, caspase cascades, apoptosis, cerebral blood flow, glucose metabolism, free-radical production, cytoskeleton breakdown, DNA damage, and nitric oxide and superoxide anions (Blaylock and Maroon 2011). Neuronal, axonal, and glial cell injury all occur in bTBI with white matter being the more vulnerable location and correlated to the burden of neurocognitive impairment (Bauman et al., 2009; Cernak et al. 2001; Giza and Hovda 2001).
Potassium efflux and sodium and calcium influx occur after mechanoporation of lipid membranes (Giza and Hovda 2001). Intracellular calcium becomes dysregulated by altered permeability of cell surface receptors leading to degenerative and excitotoxic mechanisms that are damaging to the cell. Inflammation, vascular dysfunction, white matter disease, myelin damage, axonal damage and free-radical generation are all induced by calcium-induced phospholipase activation. Calcium-induced proteolysis (as well as sheer force of injury) breaks down cytoskeletal structure and axon transport. A breakdown in the electron transport chain occurs in these times of stress leading to decreased mitochondrial calcium loading capacity and ultimately activation of the caspase-dependent apoptosis pathway. Activation of ROS can generate mitochondrial damage and apoptosis as well (Kelley et al. 2007). The presence of increased calcium alters ATP production by impairing oxidative phosphorylation and glycolysis (Giza and Hovda 2001).
Glucose is the obligate mitochondrial fuel source of the mammalian brain. Approximately 85% of brain glucose utilization is directed toward fueling sodium/potassium pumps that restore membrane potential. In an injured state, these pumps shift into overdrive to restore the altered cellular electrochemical balance requiring an increase in energy demand (Giza and Hovda 2001). Neurons lack carbohydrate storage and rely on peripheral glucose uptake past the BBB (Prieto et al. 2011). GLUT1 transporter is highly expressed in the human brain and is responsible for regulating nutrient transport depending on the metabolic state. SGLT1 also plays a role, more so in states of ischemia-hypoxia (Vemula et al. 2009). The time of increased energy demand is known to be a state of increased vulnerability in repeat injury (Giza and Hovda 2001). In the injured brain, the mitochondrial dysfunctions compromise the cellular ATP production through mitochondrial oxidative phosphorylation system (OXPHOS). Since energy demands for the survival of the injured cells are increased immediately after TBI, the exhausted mitochondria get damaged and release free radicals through its dysfunctional electron transport chain (Lifshitz et al. 2003). Following the increased free radicals, mitochondrial membrane permeability is compromised, and the pro-apoptotic protein cytochrome-c, located between the inner and outer membranes of the mitochondria, is released into the cytoplasm leading to neuronal cell death as a secondary event of TBI (Giza and Hovda 2001; Robertson et al. 2007).
Mechanisms of neuronal cell death following TBI
Neuronal cell death occurs due to both apoptotic and necrotic mechanisms of cellular degeneration (Cernak et al. 2005; Kato et al. 2007). The initial cell insult occurs from the impairment of axonal transport. Axons swell within hours of trauma which can be observed by immunohistochemistry staining (Povlishock and Becker 1985; Smith et al. 1995). The disruption in transport results in accumulation of phosphorylated neurofilament proteins in cell bodies leading to activation of microglia and thus initiating an inflammatory process. In response to this inflammatory process, glutamate receptors may become sensitized, GABA receptors may become internalized, the immune system is impacted, vasculature is compromised, and the blood–brain barrier (BBB) becomes damaged (Kaur et al. 1995; Säljö et al. 2000). This loss of membrane integrity leads to reduced barrier protection and susceptibility to neuro-inflammation (McKee et al. 2013; Tagge et al. 2018). TBI-induced mitochondrial damage, brain metabolic failure, and neurodegenerative proteins are related to cognitive deficits in rat models (Ariyannur et al. 2021).
Neutrophils initially line the vasculature and then migrate to the contusion and surrounding tissue by twenty-four hours post injury followed by infiltration of parenchymal macrophages (Johnson et al. 2015). Microglia proliferation, astrocyte hypertrophy and leukocytosis have all been observed following TBI in rats. Microglia are the predominant immune cell in a healthy brain and function on a daily basis to phagocytize apoptotic cells with neurons acting as key immunomodulators controlling microglia activity (Wofford et al. 2019). In addition, it has been shown that damage to substantia nigra in TBI is linked with microglial activation and subsequent increased risk of the development of Parkinson’s disease (Kelley et al. 2007; Loane et al. 2014). Long-term, animal models show chronic microglial activation is linked to progressive brain atrophy in mice (Hyder et al. 2002; Johnson et al. 2013). Non-traumatic sources of brain insult may be instigators of microglial priming in advance of TBI or mTBI, therefore worsening TBI or mTBI outcome (Kelley et al. 2007).
Clinical biomarkers and future outlook
The need for effective clinical interventions in chronic neurological diseases following TBI is in desperate need. The identification of serum biomarkers can be done by determining the qualitative and quantitative changes in a serum component at different time points post injury. By comparing the temporal pattern of the changes with changes detected after other forms of TBI, the biomarker allows differentiation of different injury mechanisms and comparison of the onset, extent and duration of the injury (Agoston and Kamnaksh 2015). A number of reports exist on clinical studies of plasma or CSF from trauma victims using bioassays for quantitation of breakdown products of neuronal, glial, astrocytic cells or the myelin sheath. For example, levels of glial-derived proteins, such as glial fibrillary acidic protein (GFAP), astrocyte-derived protein, such as S100b, and the neuronal-derived neuron-specific enolase (NSE) or myelin basic protein, in peripheral blood, have been used to predict outcome after severe traumatic brain injury (Berger et al. 2005; Ingebrigtsen et al. 1999; Raabe et al. 1999).
It has been suggested that a panel of biomarkers or a combination of biomarker assays and functional or radiological tests would have more usefulness in predicting TBI than a single stand-alone assay (Berger 2006). This is because of (1) the complexity of the brain tissue, in which injury to multiple cell types of varying degrees of severity will give varying outcomes, and (2) the varying half-life of biomarkers, causing them to be undetectable if assayed at an inappropriate time, i.e., the half-life for S100B is less than 60 min, making the detectability of S100B in the blood a rapid and transient event. Because of the difficulty in interpreting any one individual bioassay, the statistical probability of detecting the TBI would be higher if multiple parameters are involved rather than any single event. However, current pharmaceutical and surgical approaches are limited and complicated by the complexities of the biochemical pathways involved in injury (Giza and Hovda 2001). There is a growing call for non-drug and non-surgical methods of treatment.
Available treatment strategies for TBI
Literature regarding treatment of TBI is extensive and will be briefly discussed here. One theme that transcends current treatment modalities is uncertainty regarding its efficacy and an inability to transition pharmaceutical measures to the clinical setting (Hyder AA et al. 2007). Much of the treatment used in the current clinical setting is focused on education and supportive care rather than interventions; there is an ongoing failure of clinical trials for TBI treatment. The importance of proper supportive measures cannot be understated. Patients suffering from TBI are traditionally placed in low-stress environments to include minimizing auditory, visual, and emotional triggers. Despite these measures, outcomes are traditionally poor and prolonged. Research regarding the use of proper nutrition, vitamins and supplements as an adjunct to clinical therapies is ongoing and to date has yielded mixed results (Lucke-Wold BP et al. 2018).Many interventional options have been explored but require further research.
Psychotherapy (individual and group) emphasizes emotional and behavioral therapies specifically combating the common behavioral changes after TBI including anger, depression, anxiety, and aggression. Studies show that creating coping skills and advising on anger management techniques can reduce patient aggression and improve outcomes of TBI injury (Sinnakarppan I et al. 2005). Eastern medical techniques such as acupuncture and mind body practices may be helpful in some circumstances, however not in an acute trauma setting. Hyperbaric oxygen therapy (HBOT) is the inhalation of 100% oxygen under pressure greater than 1 atmosphere absolute (ATA) (1 ATA = 101.3 kPa). Studies have showed improved cerebral blood flow following HBOT in patients with chronic brain injury (Golden ZL et al. 2002). Positive effects such as improved quality of life in patients with post-concussion syndrome or mild TBI have also been noted (Harch PG et al. 2012). In severe TBI, HBOT is thought to even reduce mortality and lead to enhanced functional outcomes (Rockswold GL et al. 1992). Erythropoietin (EPO) promotes proliferation and differentiation of red blood cells physiologically in the body. Additional effects are enhancement of anti-apoptotic, anti-inflammatory, and neuroprotective effects. Of note, data show that recombinant human EPO mobilized endothelial progenitor cells and angiogenesis to improve the functional prognosis of TBI in rats (Wang L et al. 2015 ). More researches are needed for human studies.
The use of non-invasive brain stimulation includes repetitive transcranial magnetic stimulation (rTMS). This is a painless, non-invasive, easily operated treatment with few known adverse reactions and success in treating depression and schizophrenia. rTMS alters neuronal excitability by generating excitatory (> 5 Hz) or inhibitory (1 Hz) activity allowing manipulation of the patients neuronal function in a situation of high neuronal stress.8
Conclusion
Most of these animal models of TBI described above are mimetic of clinical TBI, and could be utilized to better investigate drivers of acute and chronic neuro-inflammation that are translationally relevant to clinical presentations. In the future, we aim to elucidate the specific passive and active immune modulators that are received by immune cells and influence their phenotype.
In a research field where inter-laboratory comparisons are difficult; this review illustrates the need to provide a degree of standardization of the methods used across laboratories. Due to the complex pathophysiology and various etiologies of TBI, bTBI, and DAI, multiple models have been brought forward in the attempt of creating accurate models of TBI injury patterns. Rodent models have proven vital in the research of TBI and bTBI. These models have been employed in the furthering of understanding of pathophysiology, associated injury patterns, development of targeted therapies and pharmaceutical interventions for the treatment of TBI. Despite these advancements, however, this review has shown that there still remain concerns, and challenges in the reproducibility, standardization, reliability, and accuracy of these models. In the future, we should aim to elucidate the multiple mechanism targeted TBI treatments based on personalized needs of patients.
References
Agoston DV, Kamnaksh A (2015) Frontiers in Neuroengineering Modeling the Neurobehavioral Consequences of Blast-Induced Traumatic Brain Injury Spectrum Disorder and Identifying Related Biomarkers. In: Brain Neurotrauma: Molecular, Neuropsychological, and Rehabilitation Aspects, vol. (Kobeissy FH, ed). Boca Raton (FL): CRC Press/Taylor & Francis© 2015 by Taylor & Francis Group, LLC
Albert-Weißenberger C, Várrallyay C, Raslan F, Kleinschnitz C, Sirén AL (2012) An experimental protocol for mimicking pathomechanisms of traumatic brain injury in mice. Exp Transl Stroke Med 4:1
Alder J, Fujioka W, Lifshitz J, Crockett DP, Thakker-Varia S (2011) Lateral fluid percussion: model of traumatic brain injury in mice. J Vis Exp
Ariyannur PS, Xing G, Barry ES, Benford B, Grunberg NE, Sharma P (2021), Effects of pyruvate administration on mitochondrial enzymes, neurological behaviors, and neurodegeneration after traumatic brain injury. Aging Dis
Axelsson H, Hjelmqvist H, Medin A, Persson JK, Suneson A (2000) Physiological changes in pigs exposed to a blast wave from a detonating high-explosive charge. Mil Med 165:119–126
Bauman RA, Ling G, Tong L, Januszkiewicz A, Agoston D, Delanerolle N, Kim Y, Ritzel D et al (2009) An introductory characterization of a combat-casualty-care relevant swine model of closed head injury resulting from exposure to explosive blast. J Neurotrauma 26:841–860
Berger RP (2006) The use of serum biomarkers to predict outcome after traumatic brain injury in adults and children. J Head Trauma Rehabil 21:315–333
Berger RP, Adelson PD, Pierce MC, Dulani T, Cassidy LD, Kochanek PM (2005) Serum neuron-specific enolase, S100B, and myelin basic protein concentrations after inflicted and noninflicted traumatic brain injury in children. J Neurosurg 103:61–68
Blaylock RL, Maroon J (2011) Immunoexcitotoxicity as a central mechanism in chronic traumatic encephalopathy-A unifying hypothesis. Surg Neurol Int 2:107
Bodnar CN, Roberts KN, Higgins EK, Bachstetter AD (2019) A systematic review of closed head injury models of mild traumatic brain injury in mice and rats. J Neurotrauma 36:1683–1706
Rockswold GL, Ford SE, Anderson DC, Bergman TA, Sherman RE (1992) Results of a prospective randomized trial for treatment of severely brain-injured patients with hyperbaric oxygen. J Neurosurg 76:929–934
Rossi S, Hallett M, Rossini PM, Pascual-Leone A, Safety of TMSCG (2009) Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research. Clin Neurophysiol 120:2008–2039
Bramlett HM, Dietrich WD (2002) Quantitative structural changes in white and gray matter 1 year following traumatic brain injury in rats. Acta Neuropathol 103:607–614
Briones TL (2015) Chapter 3 animal models of traumatic brain injury: is there an optimal model that parallels human brain injury? Annu Rev Nurs Res 33:31–73
CDC, Morbidity and Mortality Weekly Report (MMWR). Brain Injury Awareness Month in: Centers for Disease Control and Prevention USDoHaHS (Ed.), 2020, pp. 225–230
CDC, Surveillance Report of Traumatic Brain Injury-related Emergency Department Visits, Hospitalizations, and Deaths—United States, Centers for Disease Control and Prevention, U.S. Department of Health and Human Services., 2019
Cernak I (2005) Animal models of head trauma. NeuroRx 2:410–422
Cernak I, Wang Z, Jiang J, Bian X, Savic J (2001) Cognitive deficits following blast injury-induced neurotrauma: possible involvement of nitric oxide. Brain Inj 15:593–612
Cernak I, Stoica B, Byrnes KR, Di Giovanni S, Faden AI (2005) Role of the cell cycle in the pathobiology of central nervous system trauma. Cell Cycle 4:1286–1293
Chen Y, Constantini S, Trembovler V, Weinstock M, Shohami E (1996) An experimental model of closed head injury in mice: pathophysiology, histopathology, and cognitive deficits. J Neurotrauma 13:557–568
Dail WG, Feeney DM, Murray HM, Linn RT, Boyeson MG (1981) Responses to cortical injury: II. Widespread depression of the activity of an enzyme in cortex remote from a focal injury. Brain Res 211:79–89
Dixon CE, Lyeth BG, Povlishock JT, Findling RL, Hamm RJ, Marmarou A, Young HF, Hayes RL (1987) A fluid percussion model of experimental brain injury in the rat. J Neurosurg 67:110–119
Dixon CE, Clifton GL, Lighthall JW, Yaghmai AA, Hayes RL (1991) A controlled cortical impact model of traumatic brain injury in the rat. J Neurosci Methods 39:253–262
Earle SA, de Moya MA, Zuccarelli JE, Norenberg MD, Proctor KG (2007) Cerebrovascular resuscitation after polytrauma and fluid restriction. J Am Coll Surg 204:261–275
Elder GA, Cristian A (2009) Blast-related mild traumatic brain injury: mechanisms of injury and impact on clinical care. Mt Sinai J Med 76:111–118
Elder GA, Ehrlich ME, Gandy S (2019) Relationship of traumatic brain injury to chronic mental health problems and dementia in military veterans. Neurosci Lett 707:134294
Feeney DM, Boyeson MG, Linn RT, Murray HM, Dail WG (1981) Responses to cortical injury: I. Methodology and local effects of contusions in the rat. Brain Res 211:67–77
Friess SH, Lapidus JB, Brody DL (2015) Decompressive craniectomy reduces white matter injury after controlled cortical impact in mice. J Neurotrauma 32:791–800
Garman RH, Jenkins LW, Switzer RC 3rd, Bauman RA, Tong LC, Swauger PV, Parks SA, Ritzel DV et al (2011) Blast exposure in rats with body shielding is characterized primarily by diffuse axonal injury. J Neurotrauma 28:947–959
GBD (2019) Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 18:56–87
Giza CC, Hovda DA (2001) The neurometabolic cascade of concussion. J Athl Train 36:228–235
Graham NS, Sharp DJ (2019) Understanding neurodegeneration after traumatic brain injury: from mechanisms to clinical trials in dementia. J Neurol Neurosurg Psychiatry 90:1221–1233
Guley NH, Rogers JT, Del Mar NA, Deng Y, Islam RM, D’Surney L, Ferrell J, Deng B et al (2016) A novel closed-head model of mild traumatic brain injury using focal primary overpressure blast to the cranium in mice. J Neurotrauma 33:403–422
Gwarzo IH, Perez-Patron M, Xu X, Radcliff T, Horney J (2021), Traumatic brain injury related hospitalizations: factors associated with in-hospital mortality among elderly patients hospitalized with a TBI. Brain Inj:1–9.
Harch PG, Andrews SR, Fogarty EF, Amen D, Pezzullo JC, Lucarini J, Aubrey C, Taylor DV et al (2012) A phase I study of low-pressure hyperbaric oxygen therapy for blast-induced post-concussion syndrome and post-traumatic stress disorder. J Neurotrauma 29:168–185
Hoogenboom WS, Branch CA, Lipton ML (2019) Animal models of closed-skull, repetitive mild traumatic brain injury. Pharmacol Ther 198:109–122
Hyder AA, Wunderlich CA, Puvanachandra P, Gururaj G, Kobusingye OC (2007) The impact of traumatic brain injuries: a global perspective. NeuroRehabilitation 22:341-353
Hyder F, Rothman DL, Shulman RG (2002) Total neuroenergetics support localized brain activity: implications for the interpretation of fMRI. Proc Natl Acad Sci U S A 99:10771–10776
Ingebrigtsen T, Waterloo K, Jacobsen EA, Langbakk B, Romner B (1999) Traumatic brain damage in minor head injury: relation of serum S-100 protein measurements to magnetic resonance imaging and neurobehavioral outcome. Neurosurgery 45:468–475
Johnson VE, Stewart JE, Begbie FD, Trojanowski JQ, Smith DH, Stewart W (2013) Inflammation and white matter degeneration persist for years after a single traumatic brain injury. Brain 136:28–42
Johnson VE, Meaney DF, Cullen DK, Smith DH (2015) Animal models of traumatic brain injury. Handb Clin Neurol 127:115–128
Kato K, Fujimura M, Nakagawa A, Saito A, Ohki T, Takayama K, Tominaga T (2007) Pressure-dependent effect of shock waves on rat brain: induction of neuronal apoptosis mediated by a caspase-dependent pathway. J Neurosurg 106:667–676
Kaur C, Singh J, Lim MK, Ng BL, Yap EP, Ling EA (1995) The response of neurons and microglia to blast injury in the rat brain. Neuropathol Appl Neurobiol 21:369–377
Kelley BJ, Lifshitz J, Povlishock JT (2007) Neuroinflammatory responses after experimental diffuse traumatic brain injury. J Neuropathol Exp Neurol 66:989–1001
Li Y, Zhang L, Kallakuri S, Zhou R, Cavanaugh JM (2011) Quantitative relationship between axonal injury and mechanical response in a rodent head impact acceleration model. J Neurotrauma 28:1767–1782
Lifshitz J, Friberg H, Neumar RW, Raghupathi R, Welsh FA, Janmey P, Saatman KE, Wieloch T et al (2003) Structural and functional damage sustained by mitochondria after traumatic brain injury in the rat: evidence for differentially sensitive populations in the cortex and hippocampus. J Cereb Blood Flow Metab 23:219–231
Lindquist LK, Love HC, Elbogen EB (2017) Traumatic brain injury in iraq and afghanistan veterans: new results from a national random sample study. J Neuropsychiatry Clin Neurosci 29:254–259
Liu YR, Cardamone L, Hogan RE, Gregoire MC, Williams JP, Hicks RJ, Binns D, Koe A et al (2010) Progressive metabolic and structural cerebral perturbations after traumatic brain injury: an in vivo imaging study in the rat. J Nucl Med 51:1788–1795
Loane DJ, Kumar A, Stoica BA, Cabatbat R, Faden AI (2014) Progressive neurodegeneration after experimental brain trauma: association with chronic microglial activation. J Neuropathol Exp Neurol 73:14–29
Logsdon AF, Lucke-Wold BP, Turner RC, Huber JD, Rosen CL, Simpkins JW (2015) Role of microvascular disruption in brain damage from traumatic brain injury. Compr Physiol 5:1147–1160
Lucke-Wold BP, Logsdon AF, Nguyen L, Eltanahay A, Turner RC, Bonasso P, Knotts C, Moeck A et al (2018) Supplements, nutrition, and alternative therapies for the treatment of traumatic brain injury. Nutr Neurosci 21:79–91
Long JB, Bentley TL, Wessner KA, Cerone C, Sweeney S, Bauman RA (2009) Blast overpressure in rats: recreating a battlefield injury in the laboratory. J Neurotrauma 26:827–840
Ma X, Aravind A, Pfister BJ, Chandra N, Haorah J (2019) Animal models of traumatic brain injury and assessment of injury severity. Mol Neurobiol 56:5332–5345
Margulies SS, Thibault LE, Gennarelli TA (1990) Physical model simulations of brain injury in the primate. J Biomech 23:823–836
Marmarou A, Foda MA, van den Brink W, Campbell J, Kita H, Demetriadou K (1994) A new model of diffuse brain injury in rats. Part I: pathophysiology and biomechanics. J Neurosurg 80:291–300
McKee AC, Stern RA, Nowinski CJ, Stein TD, Alvarez VE, Daneshvar DH, Lee HS, Wojtowicz SM et al (2013) The spectrum of disease in chronic traumatic encephalopathy. Brain 136:43–64
Missliwetz J, Wieser I (1989) Gunshot wounds of the head in soldiers wearing military helmets– general aspects and experiments and observations on the biomechanics and wound morphology. Z Rechtsmed 102:41–54
Morales DM, Marklund N, Lebold D, Thompson HJ, Pitkanen A, Maxwell WL, Longhi L, Laurer H et al (2005) Experimental models of traumatic brain injury: do we really need to build a better mousetrap? Neuroscience 136:971–989
Namjoshi DR, Good C, Cheng WH, Panenka W, Richards D, Cripton PA, Wellington CL (2013) Towards clinical management of traumatic brain injury: a review of models and mechanisms from a biomechanical perspective. Dis Model Mech 6:1325–1338
Namjoshi DR, Cheng WH, Bashir A, Wilkinson A, Stukas S, Martens KM, Whyte T, Abebe ZA et al (2017) Defining the biomechanical and biological threshold of murine mild traumatic brain injury using CHIMERA (Closed Head Impact Model of Engineered Rotational Acceleration). Exp Neurol 292:80–91
NINDS, Traumatic Brain Injury. Hope Through Research, in: Stroke NIoNDa (Ed.), Office of Communications and Public Liaison. National Institutes of Health Bethesda, Maryland 20892 NIH Publication No. 20-NS-2478
Povlishock JT (2013) The window of risk in repeated head injury. J Neurotrauma 30:1
Povlishock JT, Becker DP (1985) Fate of reactive axonal swellings induced by head injury. Lab Invest 52:540–552
Prieto R, Tavazzi B, Taya K, Barrios L, Amorini AM, Di Pietro V, Pascual JM, Marmarou A et al (2011) Brain energy depletion in a rodent model of diffuse traumatic brain injury is not prevented with administration of sodium lactate. Brain Res 1404:39–49
Raabe A, Grolms C, Seifert V (1999) Serum markers of brain damage and outcome prediction in patients after severe head injury. Br J Neurosurg 13:56–59
Reneer DV, Hisel RD, Hoffman JM, Kryscio RJ, Lusk BT, Geddes JW (2011) A multi-mode shock tube for investigation of blast-induced traumatic brain injury. J Neurotrauma 28:95–104
Robertson CL, Saraswati M, Fiskum G (2007) Mitochondrial dysfunction early after traumatic brain injury in immature rats. J Neurochem 101:1248–1257
Rostami E, Davidsson J, Ng KC, Lu J, Gyorgy A, Walker J, Wingo D, Plantman S et al (2012) A model for mild traumatic brain injury that induces limited transient memory impairment and increased levels of axon related serum biomarkers. Front Neurol 3:115
Rowe RK, Harrison JL, Thomas TC, Pauly JR, Adelson PD, Lifshitz J (2013) Using anesthetics and analgesics in experimental traumatic brain injury. Lab Anim (NY) 42:286–291
Rubovitch V, Ten-Bosch M, Zohar O, Harrison CR, Tempel-Brami C, Stein E, Hoffer BJ, Balaban CD et al (2011) A mouse model of blast-induced mild traumatic brain injury. Exp Neurol 232:280–289
Ryu J, Horkayne-Szakaly I, Xu L, Pletnikova O, Leri F, Eberhart C, Troncoso JC, Koliatsos VE (2014) The problem of axonal injury in the brains of veterans with histories of blast exposure. Acta Neuropathol Commun 2:153
Säljö A, Bao F, Haglid KG, Hansson HA (2000) Blast exposure causes redistribution of phosphorylated neurofilament subunits in neurons of the adult rat brain. J Neurotrauma 17:719–726
Schmidt RH, Grady MS (1993) Regional patterns of blood-brain barrier breakdown following central and lateral fluid percussion injury in rodents. J Neurotrauma 10:415–430
Silverberg ND, Iverson GL (2013) Is rest after concussion “the best medicine?”: recommendations for activity resumption following concussion in athletes, civilians, and military service members. J Head Trauma Rehabil 28:250–259
Silverberg ND, Iaccarino MA, Panenka WJ, Iverson GL, McCulloch KL, Dams-O’Connor K, Reed N, McCrea M et al (2020) Management of concussion and mild traumatic brain injury: a synthesis of practice guidelines. Arch Phys Med Rehabil 101:382–393
Sinnakaruppan I, Downey B, Morrison S (2005) Head injury and family carers: a pilot study to investigate an innovative community-based educational programme for family carers and patients. Brain Inj 19:283–30
Smith DH, Soares HD, Pierce JS, Perlman KG, Saatman KE, Meaney DF, Dixon CE, McIntosh TK (1995) A model of parasagittal controlled cortical impact in the mouse: cognitive and histopathologic effects. J Neurotrauma 12:169–178
Statler KD, Kochanek PM, Dixon CE, Alexander HL, Warner DS, Clark RS, Wisniewski SR, Graham SH et al (2000) Isoflurane improves long-term neurologic outcome versus fentanyl after traumatic brain injury in rats. J Neurotrauma 17:1179–1189
Statler KD, Alexander H, Vagni V, Dixon CE, Clark RS, Jenkins L, Kochanek PM (2006) Comparison of seven anesthetic agents on outcome after experimental traumatic brain injury in adult, male rats. J Neurotrauma 23:97–108
Tagge CA, Fisher AM, Minaeva OV, Gaudreau-Balderrama A, Moncaster JA, Zhang XL, Wojnarowicz MW, Casey N et al (2018) Concussion, microvascular injury, and early tauopathy in young athletes after impact head injury and an impact concussion mouse model. Brain 141:422–458
Theadom A, Mahon S, Hume P, Starkey N, Barker-Collo S, Jones K, Majdan M, Feigin VL (2020) Incidence of sports-related traumatic brain injury of all severities: a systematic review. Neuroepidemiology 54:192–199
Thompson HJ, Lifshitz J, Marklund N, Grady MS, Graham DI, Hovda DA, McIntosh TK (2005) Lateral fluid percussion brain injury: a 15-year review and evaluation. J Neurotrauma 22:42–75
Tucker LB, Fu AH, McCabe JT (2021), Hippocampal-dependent cognitive dysfunction following repeated diffuse rotational brain injury in male and female mice. J Neurotrauma
Vemula S, Roder KE, Yang T, Bhat GJ, Thekkumkara TJ, Abbruscato TJ (2009) A functional role for sodium-dependent glucose transport across the blood-brain barrier during oxygen glucose deprivation. J Pharmacol Exp Ther 328:487–495
Wang L, Wang X, Su H, Han Z, Yu H, Wang D, Jiang R, Liu Z et al (2015) Recombinant human erythropoietin improves the neurofunctional recovery of rats following traumatic brain injury via an increase in circulating endothelial progenitor cells. Transl Stroke Res 6:50–59
Whalen MJ, Carlos TM, Kochanek PM, Heineman S (1998) Blood-brain barrier permeability, neutrophil accumulation and vascular adhesion molecule expression after controlled cortical impact in rats: a preliminary study. Acta Neurochir Suppl 71:212–214
Wofford KL, Loane DJ, Cullen DK (2019) Acute drivers of neuroinflammation in traumatic brain injury. Neural Regen Res 14:1481–1489
Wojnarowicz MW, Fisher AM, Minaeva O, Goldstein LE (2017) Considerations for experimental animal models of concussion, traumatic brain injury, and chronic traumatic encephalopathy-these matters matter. Front Neurol 8:240
Xiong Y, Mahmood A, Chopp M (2013) Animal models of traumatic brain injury. Nat Rev Neurosci 14:128–142
Yarnell AM, Shaughness MC, Barry ES, Ahlers ST, McCarron RM, Grunberg NE (2013), Blast traumatic brain injury in the rat using a blast overpressure model. Curr Protoc Neurosci Chapter 9:Unit 9 41
Zhu F, Skelton P, Chou CC, Mao H, Yang KH, King AI (2013) Biomechanical responses of a pig head under blast loading: a computational simulation. Int J Numer Method Biomed Eng 29:392–407
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Patrick Haggard.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Uniformed Services University, Department of the Navy, Department of Defense, nor the U.S. Government. This work was supported, by CDMRP Grant 167094 funding to PS.
Rights and permissions
About this article

Cite this article
Petersen, A., Soderstrom, M., Saha, B. et al. Animal models of traumatic brain injury: a review of pathophysiology to biomarkers and treatments. Exp Brain Res 239, 2939–2950 (2021). https://doi.org/10.1007/s00221-021-06178-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-021-06178-6