
Abstract
Light touch of a stable reference reduces sway during standing. However, unexpected displacement of a light touch reference leads to short-latency reactions in ankle muscles consistent with a balance reaction, that are replaced by responses in arm muscles on subsequent trials. We anticipated that the excitability of sensorimotor pathways arising from finger cutaneous afferents would reflect these changes in behavior. We hypothesized that (1) interlimb cutaneous reflexes in muscles of the ipsilateral leg, derived from median nerve (MED) stimulation would be facilitated when touch was stable, but reduced when touch was unreliable, (2) intralimb MED reflexes in muscles of the homonymous arm would be facilitated when touch was unreliable and participants tracked the touch reference with arm movements, and (3) radial nerve (RAD) evoked reflexes would be unaffected, given that the RAD innervation territory is not involved in the light touch task. Cutaneous reflexes were evoked using a transcutaneous train of pulses (5 × 1.0 ms square-wave pulses; 300 Hz) and recorded using electromyography of muscles of the ipsilateral arm and leg. As hypothesized, interlimb MED reflexes recorded in soleus (SOL) were larger when touching the stable reference (mean ± SD % MVC; 4.78 ± 1.57) than when not touching a reference (1.00 ± 1.05) or when touching an unstable reference (1.07 ± 1.16). In addition, intralimb MED reflexes in anterior deltoid (AD) were larger when touching an unstable reference (4.50 ± 1.31), compared to touching a stable reference (1.34 ± 1.01) or not touching (1.50 ± 1.00). In contrast, interlimb RAD reflexes in SOL were larger when not touching (4.29 ± 4.34), compared with touching a stable (1.14 ± 1.84) or unstable reference (3.11 ± 4.15). These findings indicate that cutaneous reflexes from the hand are scaled with a rapid change in motor behavior when a touch reference becomes unstable, suggesting that spinal sensorimotor pathways are functionally reweighted based in part upon the reliability of tactile inputs.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Tactile inputs from the hands provide meaningful cues related to balance and stability when the hands are holding external supports, such as a cane (Oshita and Yano 2016; Sozzi et al. 2017). Indeed, it is well-established that lightly touching an external reference reduces sway, even when the force applied (< 1 N) is insufficient to provide mechanical support (Holden et al. 1994; Jeka and Lackner 1994; Kouzaki and Masani 2008). However, the meaning of cutaneous inputs to balance control becomes quite different when holding objects that provide no additional support (e.g. a briefcase), or that destabilize balance (e.g. a dog’s leash). Ambiguity or misinterpretation of the sensory inputs could lead to inappropriate responses that not only may fail to restore balance but might themselves be destabilizing. Ambiguous sensory stimuli, including from visual (van Asten et al. 1988), vestibular (Fitzpatrick et al. 2002), proprioceptive (Hayashi et al. 1981), and tactile (Jeka et al. 1998; Misiaszek et al. 2016) inputs, has been shown to generate powerful illusions of movement, inducing sway and instability. These sway illusions have been induced by the manipulation of a single sensory modality, indicating that the inaccurate stimulus is difficult to ignore, despite the other sensory cues providing feedback on body position being in conflict. Thus, the accurate interpretation of sensory feedback is critical to generating functionally meaningful balance corrections (Peterka 2002).
We recently demonstrated that rapid, unexpected displacement of a touch reference can initiate a balance-corrective response, in the absence of a mechanical threat to stability (Misiaszek et al. 2016; Misiaszek and Vander Meulen 2017). These “false-positive” balance reactions were only observed on the first exposure to the unexpected stimulus, with subsequent touch displacements resulting in a more appropriate arm extension reaction. This rapid “repurposing” of the tactile cues following the initial inaccurate response indicates that the sensorimotor processes for initiating a motor response are highly adaptable. The ability to quickly modify the sensory interpretation and adapt the motor behaviour based upon recent experience is important to meet the needs of maintaining stability in challenging, and often unpredictable, environments. The need to rapidly select an appropriate motor behaviour to suit the immediate need is similar to that faced in other tasks, such as reaching, when multiple possible movements might be considered before one is decided upon and implemented (Cisek 2007; Thura et al. 2012). It has been suggested that when such challenges are encountered multiple motor solutions are encoded in parallel, enabling the motor system to respond quickly and flexibly (Gallivan et al. 2016). This “affordance competition hypothesis” (Cisek 2007; Gallivan et al. 2016; Thura et al. 2012) could also explain the rapid switch from a balance response strategy to an arm extension behaviour following a single touch displacement. The selection of an alternative motor solution should be recognizable as a change in sensorimotor gain of relevant neural pathways, including inter- and intralimb cutaneous reflexes.
Electrical stimulation of cutaneous nerves serving the hand leads to segmental and non-segmental responses in motoneuronal activity (Chen and Ashby 1993; Jenner and Stephens 1982; Zehr et al. 2001). For this study, we refer to the non-segmental responses in the ipsilateral leg as interlimb reflexes and the segmental responses within the homonymous arm as intralimb reflexes. Recently, Forero and Misiaszek (2014, 2015) demonstrated that the excitability of these cutaneous-evoked reflexes is modulated when participants were asked to lightly touch a stable reference while walking blind-folded on a treadmill. The implication is that cutaneous reflexes are relevant sensorimotor neural pathways related to the role of light touch in creating stability while walking, and presumably, standing. If so, then we expect that cutaneous reflexes evoked from nerves serving the hand will demonstrate changes in excitability consistent with the expression of an alternative motor solution after participants switch from a balance reaction to an arm extension response with repeated exposures of a light touch reference. Specifically, we hypothesized that reflexes evoked with median nerve stimulation, innervating the volar surface of the lateral digits, including the index finger used to apply light touch, would be (1) facilitated in the muscles of the ankle when the touch reference was stable, but would be reduced when the touch reference had moved and participants were engaging an arm extension behaviour, and (2) would be facilitated in the arm muscles when participants were engaging an arm extension behaviour. In addition, we hypothesized that (3) reflexes evoked with radial nerve stimulation would be unaffected by touch or the switch in motor behaviour, given that the radial nerve innervation territory, serving the dorsal aspect of the hand, is not involved in the light touch task.
Material and methods
Participants
Twenty-three healthy adults (20–28 years of age; 17 women) volunteered to participate in this investigation. Participants reported no history of neurologic, musculoskeletal, metabolic or cardiovascular disease, and had not experienced musculoskeletal injury or concussion in the past 6 months. Participants provided written consent prior to testing, however were kept naïve to the fact that the touch reference would move. Following testing, the true nature of the study was disclosed and participants were given the opportunity to withdraw their consent. The study was approved by the University of Alberta Research Ethics Board in accordance with the Declaration of Helsinki.
Instrumentation
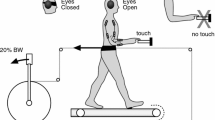
Participants stood barefoot on a 5 cm thick foam (ethylene–vinyl acetate, EVA) atop a 6-component force plate (OR6-7-1000, Advanced Mechanical Technology, Inc., Watertown, MA, USA) with feet shoulder-width apart, or what was deemed comfortable by the participant. The vision was occluded by the use of a pair of blackened goggles. Participants were instructed to stand quietly and to maintain a neutral posture of the head. In some conditions, participants were asked to lightly touch a plastic rod (7.5 cm long) with their right index finger. The rod included a centrally located raised dimple to provide a spatial reference. The rod was located in front and to the right of participants, such that it was aligned laterally to the arm. The right index finger was angled so that only the finger pad was in contact with the rod, while the other fingers were curled into the palm to prevent inadvertently contacting the rod. The arm was positioned so that the forearm was aligned horizontally and the upper arm was vertical, such that the elbow was maintained in approximately 90° of flexion. In the “no touch” conditions, participants were asked to maintain the same posture, but with the touch reference lowered so that no contact was made. The touch reference was mounted on a square rail acme screw drive positioning stage (LinTech 130 Series, LinTech Positioning Systems, Monrovia, CA, USA), driven by a two-phase stepper motor (Applied Motion Products 5023-124 2-phase hybrid stepper motor, Watsonville, CXA, USA), to produce ramp-and-hold linear displacements in the fore/aft direction. Touch plate displacements were 12.5 mm with a peak velocity of 124 mm/s. Stage position was measured using a linear displacement sensor (Penny & Giles SLS130, Curtis-Wright Industrial Group, Christchurch, UK). The entire touch reference positioning apparatus was mounted on a 6-component force transducer (MC3A-100, Advanced Mechanical Technology, Inc., Watertown, MA, USA) to measure the vertical load applied by the participant when touching the rod. Participants were instructed to maintain a light touch of less than 1 N during the “touch” conditions. Prior to testing, participants were allowed to practice maintaining light touch and were provided auditory cueing during testing when the touch force exceeded 1 N. The mild noise generated by the operating motor was obscured by delivering white noise via a pair of over-the-ear headphones. Participants wore the headphones and received white noise during all conditions. A safety harness was not used, but a spotter was positioned adjacent to the participant during testing.
Electromyographic (EMG) recordings were obtained from tibialis anterior (TA), soleus (SOL), vastus lateralis (VL), and biceps femoris (BF) of the right leg, and anterior deltoid (AD), posterior deltoid (PD), biceps brachii (BB), and triceps brachii (TB) of the right arm, replicating the muscles recorded in Misiaszek et al. (2016) with the addition of VL and BF. Pairs of Ag/AgCl surface electrodes (NeuroPlus A10040, Vermed, Bellows Falls, Vermont, USA) were placed on the skin over the bellies of the intended muscles, with an inter-electrode distance of about 2 cm. Ground electrodes were placed over the right clavicle, at the midpoint between the acromium and sternum, and the anterior tibia of the right leg, at the midpoint between the medial condyle and medial malleolus. All electrode sites (including the stimulations sites below) were shaved and cleaned with isopropyl alcohol prior to application of the electrodes to ensure an impedance of less than 20 kΩ (Grass F-EZM5 impedance meter, Astro-Med, Inc., West Warwick, Rhode Island, USA). An electrogoniometer (SG110, Biometrics Ltd., Newport, UK) was placed across the right elbow joint.
Nerve stimulation
Cutaneous reflexes were elicited by delivering electrical stimulation to two nerves in the right arm: (1) the median nerve (MED), which innervates the palmar surface and the distal thumb, the index and middle finger; and (2) the superficial radial nerve (RAD), which innervates the dorsum of the thumb, index, and middle finger. As participants needed to be naïve to the study protocol, each nerve was studied in two separate cohorts of participants. Twelve participants received MED stimulation, while eleven received RAD stimulation. The cutaneous reflexes were elicited with trains (5 × 1.0 ms square-wave pulses at 300 Hz) of isolated current (Grass S88 stimulator with SIU5 and CCU1 isolation and constant current units, Astro-med Inc., West Warwick, RI, USA) delivered via a pair of disposable Ag/AgCl surface electrodes (NeuroPlus A10040, Vermed, Bellows Falls, Vermont, USA). For stimulation of the MED, the electrodes were placed on the ventral surface of the forearm, just proximal to the crease of the wrist joint. For stimulation of the RAD, the electrodes were placed on the dorsal surface of the forearm, just proximal to the distal radial head and the crease of the wrist. Optimal placement of the electrodes was facilitated by using a probe electrode to isolate the subcutaneous location of the nerve of interest before applying the self-adhesive electrodes used during testing. Stimulus intensity was expressed as a multiple of the radiating threshold (RT), estimated as the lowest current necessary to produce a clear radiating cutaneous paresthesia of the innervation territory of the stimulated nerve. A stimulus intensity of 2 × RT was used during testing and RT was verified between conditions to ensure consistency of the applied stimulus. Twenty stimuli were delivered for each test condition, with an inter-stimulus time of between 8 and 15 s.
Protocol
Reflexes were collected during four standing conditions: (1) without touch (no touch, NT), (2) lightly touching a stable reference (T), (3) lightly touching an unstable reference (U), and (4) a second NT. Given that the introduction of touch reference displacements was expected to alter the sensorimotor state, the order of presentation of the conditions could not be randomized. During the T condition, participants were instructed to stand quietly and maintain a light touch of the reference while receiving the stimuli at the wrist. During the U condition, the participant was instructed that the trial would be replicating the previous T condition. Participants stood touching the reference for a minimum of 10 s before the first unexpected displacement of the touch reference occurred. This first unexpected displacement was always in the forward direction (i.e. away from the participant). Thereafter, displacements of the reference were delivered randomly in either direction with random inter-displacement intervals ranging from 1 to 10 s. Cutaneous reflexes were delivered during inter-displacement periods with a minimum of 2 s after the preceding displacement and only when the participant was visibly stable and maintaining a touch less than 1 N. The U condition required approximately 5 min to acquire the 20 stimuli, consequently, the other conditions were the same duration with stimuli randomly distributed throughout the testing period. Participants were asked to sit for a minimum of 2 min between conditions. Following testing, maximum voluntary contractions (MVC) were obtained from the EMG of each muscle by asking participants to perform isometric contraction against resistance. To obtain the MVCs, participants were seated in a chair with back support, their torso vertical, and their upper legs perpendicular. The knee was flexed to 120° and the ankle was at 90°. A nylon strap, positioned beneath the forefoot for SOL, over the forefoot for TA, about the lower tibia for VL and BF, provided resistance against plantarflexion, dorsiflexion, knee extension, and knee flexion, respectively. For AD and PD, participants raised their arms forward or backward, respectively, to just below horizontal and were asked to elevate further against a nylon strap just proximal of the elbow. For BB and TB, participants flexed their elbow to 90° and were asked to further flex or extend against the nylon strap positioned at the wrist, their elbow supported by an arm rest. Participants were asked to make three attempts at their maximal effort, with vocal encouragement and visual feedback of their EMG output.
Data acquisition and processing
All data signals were digitized online at 2000 Hz using a National Instruments data acquisition card (PCI-MIO-16E-4, National Instruments, Austin, TX, USA) and stored to the hard drive in a continuous data stream using a custom-written LabView v8.2 (National Instruments, Austin, TX, USA) data acquisition routine. Prior to digitization, the EMG signals were band-pass filtered (30 Hz–1 kHz) and variably amplified (500–5000×) using Grass P511 amplifiers (Astro-Med, Inc., West Warwick, RI, USA). Subsequently, the data were processed offline using custom-written LabView v8.2 analysis routines. The EMG signals were digitally full-wave rectified and then low-pass filtered at 50 Hz (zero-lag fourth-order Butterworth filter), while the mechanical signals were low-pass filtered at 10 Hz.
To calculate the cutaneous reflexes, each stimulus train was identified within the continuous data stream of a trial and a 300 ms data segment extracted, beginning 50 ms prior to the onset of the stimulus artifact. Subsequently, the 20 extracted segments from a trial were averaged and reflex amplitudes were estimated from the averaged EMG trace. The amplitude of the middle latency cutaneous reflexes was taken as the root mean square (RMS) value within the time window of 80–120 ms for the interlimb reflexes, and 50–90 ms for the intralimb reflexes. Reflex amplitudes were then expressed as a percentage of the maximum voluntary contraction for that muscle (% MVC). Background EMG activity was estimated as the RMS value from the 50 ms period prior to the stimulus artifact and expressed as a % MVC. In addition, the touch force was estimated from the respective averaged traces for the 50 ms prestimulus period.
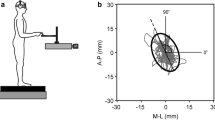
In addition, the occurrence of a postural response following the first, unexpected displacement of the light touch reference was identified for each participant. To do so, a 900 ms trace was extracted from the continuous data feed, aligned to the onset of the touch displacement and including a 300 ms predisplacement period. To determine if the touch displacement evoked a response in the recorded muscles, a two standard deviations band around the mean EMG activity for the 100 ms prior to the displacement was calculated. A response was considered to be present if the EMG trace after the onset of the displacement exited this band for at least 20 continuous milliseconds (Misiaszek et al. 2016). For consistency with our previous studies, only responses with onset latencies < 200 ms were considered, capturing the rapid responses (~ 100 ms latency) observed in TA and SOL previously. A similar method was used to determine if the elbow angle changed in response to the touch displacement, except that a movement onset of < 400 ms was considered. To estimate if the touch displacement induced a forward sway the anterior–posterior position of the center of pressure (COPA–P) was calculated from the force plate data and a 900 ms trace, with a 300 ms predisplacement period, aligned to the displacement was extracted. A two standard deviation band was estimated for the 300 ms predisplacement period and if the COPA–P exited this band for at least 20 continuous ms < 400 ms after the displacement onset, a touch-induced sway was considered to have occurred. A postural response was considered to have been evoked in response to the first unexpected forward displacement of the touch reference if a forward sway was identified, coupled with an EMG burst in TA. A forward sway alone was insufficient to meet the requirements of a postural response as the forward displacement of the COP could arise from other events, including a forward extension of the arm. The presence of an elbow extension or burst in AD indicated an arm-tracking response. Given that the displacements of the touch reference were used to create instability in the light touch, whilst eliciting cutaneous reflexes intermittently throughout, the subsequent touch displacements could not be evaluated.
Statistics
Due to a technical limitation, the MVCs from one participant in the MED cohort could not be obtained. Therefore, this participant’s data was not included in the analysis of the median nerve reflex amplitudes. However, this participant’s data was included in the evaluation of the first trial responses as that analysis does not require normalization of the EMG. To ensure that no systematic changes in reflex amplitude were evident over time for a task that was expected to yield comparable results, the second NT condition was compared to the first using paired t tests. No differences (p > 0.05) between NT conditions were identified and the subsequent statistical analysis included only the first NT condition. Cutaneous reflex amplitudes across conditions were compared using separate repeated measures analyses of variance (rmANOVA) for each muscle and stimulated nerve. Normality of the data was confirmed with the Shapiro–Wilk test and the Greenhouse–Geisser correction was used when sphericity was not met. Main effects of condition, identified by the rmANOVAs, were then further characterized by Bonferroni corrected paired t tests (comparing NT vs. T, NT vs. U, T vs. U). Background EMG was also compared in this way. Touch force was compared between the T and U conditions with the use of a two-tailed paired t test. Frequency of occurrence of postural responses following the first unexpected touch displacements were compared between cohorts and with previous data (Misiaszek et al. 2016) using Fisher’s exact test. Statistical analyses were performed with the Real Statistics Using Excel add-in (Zaiontz 2020) with α = 0.05. Descriptive statistics are presented as the mean ± standard deviation and Cohen’s d is presented for significant effects identified by paired t tests.
Results
Typically, cutaneous reflexes evoked with electrical stimulation require background EMG activity in the target muscle to be expressed. In this study, the task of standing on foam led to preferential activation of SOL, while maintaining the posture of the arm introduced tonic activity in AD, across all participants. Thus, cutaneous reflexes were consistently observed in these two muscles, with inconsistent responses expressed in the other recorded muscles. Consequently, we focus our findings on the reflexes observed in SOL and AD.
Median nerve stimulation
Stimulation of MED resulted in a middle latency reflex in SOL that was most apparent when participants were standing while lightly touching the stable reference. Figure 1a depicts the average EMG trace from one participant while touching (T, thick trace) overlaid onto the trace while standing without touching (NT, thin trace). As can be seen, the reflex in the NT condition is barely expressed but is clearly apparent during the T condition. In Fig. 1b, it can be seen that after the touch reference becomes unreliable (U, thick trace) the response to the MED stimulation is not obviously different from that observed during the NT condition. These findings were consistent across participants, as depicted in the group summary data displayed in Fig. 1c. The mean middle latency reflex amplitudes in SOL to MED stimulation were 1.00 ± 1.05% MVC, 4.78 ± 1.57% MVC, and 1.07 ± 1.16% MVC, for NT, T, and U, respectively. The rmANOVA indicated a main effect of condition (F2,20 = 39.48, p < 0.001), with post hoc comparisons indicating that reflexes during T were significantly larger than during both NT (p < 0.001, d = 1.99) and U (p < 0.001, d = 1.88). In contrast, the background EMG activity in SOL was not different across conditions. Mean background EMG in SOL was 7.54 ± 2.56% MVC, 8.53 ± 3.69% MVC, and 9.13 ± 4.22% MVC, for NT, T, and U, respectively. The rmANOVA indicated no significant main effect of condition (F2,20 = 1.33, p = 0.29) on background SOL EMG amplitudes.

Middle latency reflex responses in TA and SOL following MED stimulation. Overlaid average EMG traces from TA and SOL for one participant during the a NT (thin trace) and T (thick trace) conditions, and b NT (thin trace) and U (thick trace) conditions. The grey boxes indicate the middle latency window used for analysis of the reflex amplitude. c Amplitude of the middle latency reflexes in SOL across participants for the three touch conditions. Each data point represents individual participants. Asterisks indicate statistically significant differences (p < 0.05). TA tibialis anterior; SOL soleus; NT no touch; T stable touch; U unstable touch
Figure 2a depicts the average EMG trace in AD following stimulation of MED during the T (thick trace) and NT (thin trace) conditions from one participant. For this participant, a clear middle latency reflex was expressed in AD during both conditions. The waveform expressed in the two conditions was qualitatively different, however the amplitude of the response within the middle latency analysis window was comparable. In contrast, the amplitude of the middle latency reflex expressed during the U condition (thick trace in Fig. 2b) was markedly increased, as contrasted against the NT condition (thin trace in Fig. 2b). This increase in middle reflex amplitude during the U condition was consistently expressed in all participants, as shown in the group summary data in Fig. 2c. The mean middle latency reflex amplitudes in AD to MED stimulation were 1.50 ± 1.00% MVC, 1.34 ± 1.01% MVC, and 4.50 ± 1.31% MVC for NT, T, and U, respectively. The rmANOVA indicated a main effect of condition (F2,20 = 88.82, p < 0.001), with post hoc comparisons indicating that reflexes during U were significantly larger than during both NT (p < 0.001, d = 3.07) and T (p < 0.001, d = 3.14). In contrast, the background EMG activity in AD was not different across conditions. Mean background EMG in AD was 6.52 ± 2.39% MVC, 6.20 ± 2.42% MVC, and 6.56 ± 2.26% MVC, for NT, T, and U, respectively. The rmANOVA indicated no significant main effect of condition (F2,20 = 0.64, p = 0.54) on background AD EMG amplitudes.

Middle latency reflex responses in PD and AD following MED stimulation. Overlaid average EMG traces from PD and AD for one participant during the a NT (thin trace) and T (thick trace) conditions, and b NT (thin trace) and U (thick trace) conditions. The grey boxes indicate the middle latency window used for the analysis of the reflex amplitude. c Amplitude of the middle latency reflexes in AD across participants for the three touch conditions. Each data point represents individual participants. Asterisks indicate statistically significant differences (p < 0.05). PD posterior deltoid; AD anterior deltoid; NT no touch; T stable touch; U unstable touch
Mean touch force was 0.51 ± 0.28 N and 0.55 ± 0.25 N for T and U, respectively. A paired t test indicated no significant difference between conditions (t10 = − 0.53, p = 0.61).
Radial nerve stimulation
Figure 3a, b depicts the average EMG traces for TA and SOL from one participant that received RAD stimuli. A clear reflex was evoked in SOL in the NT condition (thin trace), that was markedly decreased in the T condition (thick trace) in Fig. 3a. The amplitude of the reflex during the U condition (thick trace) was comparable to NT for this participant (Fig. 3b). This adaptation in SOL middle reflex amplitude was generally expressed across all participants, as shown in Fig. 3c. The mean middle latency reflex amplitudes in SOL to RAD stimulation were 4.29 ± 4.34% MVC, 1.14 ± 1.84% MVC, and 3.11 ± 4.15% MVC, for NT, T, and U, respectively. The rmANOVA indicated a main effect of condition (F2,20 = 11.72, p < 0.001), with post hoc comparisons indicating that reflexes during T were significantly smaller than during both NT (p = 0.0032, d = 1.16) and U (p = 0.015, d = 0.87). In contrast, the background EMG activity in SOL was not different across conditions. Mean background EMG in SOL was 11.57 ± 3.72% MVC, 11.18 ± 3.56% MVC, and 11.99 ± 4.24% MVC, for NT, T, and U, respectively. The rmANOVA indicated no significant main effect of condition (F2,20 = 1.52, p = 0.24) on background SOL EMG amplitudes.

Middle latency reflex responses in TA and SOL following RAD stimulation. Overlaid average EMG traces from TA and SOL for one participant during the a NT (thin trace) and T (thick trace) conditions, and b NT (thin trace) and U (thick trace) conditions. The grey boxes indicate the middle latency window used for analysis of the reflex amplitude. c Amplitude of the middle latency reflexes in SOL across participants for the three touch conditions. Each data point represents individual participants. Asterisks indicate statistically significant differences (p < 0.05). TA tibialis anterior; SOL soleus; NT no touch; T stable touch; U unstable touch
Mean touch force was 0.39 ± 0.25 N and 0.39 ± 0.24 N for T and U, respectively. A paired t test indicated no significant difference between conditions (t10 = 0.12, p = 0.91).
During these standing tasks, stimulation of RAD did not evoke prominent or consistent middle latency reflexes in AD. Consequently, analysis of middle latency reflexes in AD was not pursued further.
First trial postural responses
Postural responses to the first unexpected displacement of the touch reference were considered to have occurred when a short-latency (< 200 ms) burst of TA activity was coupled with early onset (< 400 ms) forward sway in the COP. Of the 12 participants in the MED cohort, only 2 responded to the first unexpected displacement of the touch reference with a postural response. In contrast, 7 of the 11 participants in the RAD cohort responded to the first touch displacement with a postural response. Fisher’s exact test indicated that there was a significant difference in the postural response rate between the cohorts (p = 0.036). Fisher’s exact tests were also used to compare these findings to the response rates observed previously by Misiaszek et al. (2016), wherein 12 of 20 participants responded to the first light touch displacement with a postural response. The response rate in the MED cohort was found to be different (p = 0.028), whereas the response rate in the RAD cohort was not different (p = 1.0). None of the participants, of either cohort, responded to the first perturbation trial with an EMG burst in AD or extension of the elbow.
Discussion
Contact with a light touch reference during standing, and the unexpected displacement of that reference, alter the excitability of cutaneomuscular reflexes arising from the hand. Reflexes arising from both the sensory territory of the light touch (MED) and from uninvolved regions of skin (RAD) were affected by the presence and reliability of the touch reference. We propose here that these findings reflect context-dependent gain changes of spinally-mediated sensorimotor pathways involved with the generation of rapid reactions to unexpected sensory events at the hand.
Selective gating and amplification of cutaneous reflexes
The light touch of a stable reference resulted in a fourfold increase in the amplitude of the middle latency reflex in SOL evoked with MED stimulation. This indicates that the sensorimotor pathways linking the cutaneous afferents of the fingertip to muscles at the ankle are facilitated when touch is functionally relevant in standing balance control. This is consistent with the findings of Forero and Misiaszek (2015) who demonstrated that interlimb reflexes evoked with MED stimulation were facilitated by the presence of fingertip light touch during treadmill walking. However, when the light touch reference periodically and unpredictably moved, the amplitude of these interlimb cutaneous reflexes in SOL was not different from standing without touch. The implication being that the introduction of instability at the touch contact leads to the gating of the interlimb reflex. In contrast, the amplitude of the middle latency reflex in AD with MED stimulation was not influenced by touching a stable reference. Rather, these intralimb cutaneous reflexes demonstrated a fourfold increase in amplitude when the light touch reference had become unstable, coincident with the gating of the interlimb reflex. Taken together, these findings are consistent with our hypotheses and demonstrate a correlation between the amplitude of cutaneomuscular reflexes arising from MED and the expression of specific behavioural responses to the unexpected displacement of a touch reference observed previously (Misiaszek et al. 2016; Misiaszek and Vander Meulen 2017).
The middle latency interlimb reflex in SOL observed with stimulation of RAD was markedly suppressed when participants touched a stable reference, in contrast to our hypothesis. Given that RAD innervates the dorsum of the hand, we had anticipated that reflexes arising from this nerve would be unaffected by the light touch activities as this region of the hand was not involved with the task per se. Indeed, we previously demonstrated that the amplitude of interlimb reflexes arising from RAD were correlated with the changes in background EMG activity during treadmill walking, but that the presence or absence of a touch reference did not otherwise affect the amplitude (Forero and Misiaszek 2015). What is interesting to note is that the RAD-evoked reflex in SOL was largest during the no touch and the unreliable touch conditions, being suppressed during the touch condition. This pattern of task-related modulation was opposite the pattern observed for the MED-evoked reflexes in SOL and suggests that the change was not related to some generalized state of arousal. Recently, Pearcey and Zehr (2019) described the territory innervated by RAD as serving a role as a “sensory antenna” during walking, capable of detecting potential threats to stability and initiating appropriate gait adaptations, through intersegmental cutaneous reflexes, in response. If RAD serves a similar role in standing balance, then the larger intersegmental reflexes we observed could reflect a specific amplification of this pathway when the hand was not engaged in balance stabilization per se, that is, during no touch and unstable touch conditions where contact with the outside of the hand might be anticipated, in the absence of contact with a stable touch reference in the touch condition. Such a role for the RAD territory in standing balance control is worthy of further study but is supported by the observation that light touch need not be applied at the fingertip to influence standing sway (Rogers et al. 2001).
Functional reweighting of tactile sensorimotor pathways in balance control
It is well documented that cutaneous reflexes are modulated in a task-dependent manner. Indeed, gating of intralimb cutaneous reflexes arising from the skin of the feet is correlated with the functional demands of restoring stability during standing (Burke et al. 1991) and walking (Haridas et al. 2005). Interlimb cutaneous reflexes in the arm, arising from the stimulation of the nerves of the foot, have also been shown to be modulated based upon the presence of a tripping threat (Haridas et al. 2006) or contact with an earth-referenced handrail (Lamont and Zehr 2007). Similarly, cutaneous reflexes arising from the hand are regulated depending on the presence or absence of a stable light touch reference during walking (Forero and Misiaszek 2014, 2015). Thus, there is an abundance of evidence to indicate that cutaneous reflexes are specifically regulated within the framework of postural control and stability.
Our results add to this growing body of evidence, but further indicate that these spinal sensorimotor pathways are rapidly reweighted based in part upon the relevance or reliability of the tactile inputs. That is, contact with a surface is not sufficient to cause an increased gain in these spinal reflexes. Rather, the gain in the reflex pathway is regulated in part due to the perceived functional role of the sensory feedback arising from the contact. Prochazka (1989) referred to this context-dependent selective gating and amplification of sensorimotor pathways, based upon the expected requirements of a movement, as sensorimotor or postural set. Misiaszek (2006) further suggested that the postural set scales the gains within sensorimotor pathways in part based upon the changing needs of the specific behavioural task being performed. In this way, multiple motor solutions are constantly evaluated based upon the context and sensory state at the time of a disturbance reminiscent of a finite state control system (Prochazka 1996). The behaviour that is ultimately expressed then arises as a consequence of the summation of the pre-weighted or scaled sensorimotor pathways recruited by the stimulus (Misiaszek et al. 2020). This context-dependent regulation of sensorimotor pathways is consistent with the concept of sensory reweighting (Peterka 2002). Peterka (2002) argued that the integration of sensory information for balance control is adaptive, with reweighting of sensory channels playing a critical role in regulating the relative importance of each sensory input. We suggest that sensory reweighting of the spinal reflexes, achieved by descending postural set, allows for the selective gating and amplification of the functionally relevant sensorimotor pathways that we observed.
Functional considerations
Misiaszek et al. (2016) demonstrated that the sudden, unexpected displacement of a light touch reference normally resulted in an “illusory” balance corrective reaction, which was only observed with the first trial. Balance corrective responses were not observed with subsequent displacements. Rather, an arm-tracking behaviour emerged thereafter. The modulation of the MED reflexes we observed in both the leg and the arm mirror these anticipated changes in behaviour. However, it is important to note that participants in the present study did not respond to the initial light touch displacement in the same way as our previous studies. In each of our previous studies, a balance corrective reaction was observed in approximately 60% of all participants when the initial displacement of the light touch reference is presented alone (Misiaszek et al. 2016, 2020; Misiaszek and Vander Meulen 2017), while 100% of participants displayed a balance reaction when the initial displacement was paired with an acoustic startle (Misiaszek et al. 2020). In the present study, the RAD cohort of participants responded to the initial touch displacement in a similar ratio as what we have seen previously, with 7 of 11, or 64%, displaying a balance corrective response. In contrast, only 17%, or 2 of 12 participants of the MED cohort displayed a balance corrective response with the initial touch displacement. On the surface, this outcome challenges the premise of the hypothesis for this study and suggests that the regulation of the MED reflexes was independent of the presumed correlation with an evoked balance corrective response. However, it is important to note that none of the MED cohort displayed an “arm-tracking” behaviour with the initial touch displacement, and two participants did display a balance corrective response. We suggest that this indicates that the expression of a balance corrective response with the light touch displacement paradigm is peri-threshold and that the MED stimulation pushed the expression of the response further from the threshold.
Typically, the expression of the balance corrective response is not ubiquitous with only 60% of individuals displaying the response. However, the response was uniformly expressed when the touch displacement was paired with an acoustic startle, suggesting the threshold for the response is malleable. We suggest that the stimulation of MED, which likely increased the awareness or attention to the stimulus territory of the touch, altered the threshold for expression of the behavioural response, but not the selection of the response per se. The interaction of the stimulus to MED with the expression of the balance corrective response is worthy of further study. The balance corrective responses to the light touch displacement are “false positive” reactions, that could themselves be destabilizing to balance. Illusory or false positive balance reactions are common and have been observed with a variety of stimulus modalities including visual (van Asten et al. 1988), vestibular (Fitzpatrick et al. 2002), proprioceptive (Hayashi et al. 1981), and light touch (Jeka et al. 1998; Misiaszek et al. 2016) stimuli. The accurate interpretation of the sensory information related to balance control is essential. This finding suggests a potential means of reducing the expression of the illusory response and thereby reducing the risk that misinterpreted sensory input will lead to a fall.
References
Burke D, Dickson HG, Skuse NF (1991) Task-dependent changes in the responses to low-threshold cutaneous afferent volleys in the human lower limb. J Physiol 432:445–458
Chen R, Ashby P (1993) Reflex responses in upper limb muscles to cutaneous stimuli. Can J Neurol Sci 20:271–278
Cisek P (2007) Cortical mechanisms of action selection: the affordance competition hypothesis. Philos Trans R Soc Lond B Biol Sci 362:1585–1599
Fitzpatrick RC, Marsden J, Lord SR, Day BL (2002) Galvanic vestibular stimulation evokes sensations of body rotation. NeuroReport 13:2379–2383
Forero J, Misiaszek JE (2014) The effect of light touch on the amplitude of cutaneous reflexes in the arms during treadmill walking. Exp Brain Res 232:2967–2976
Forero J, Misiaszek JE (2015) The amplitude of interlimb cutaneous reflexes in the leg is influenced by fingertip touch and vision during treadmill locomotion. Exp Brain Res 233:1773–1782
Gallivan JP, Logan L, Wolpert DM, Flanagan, (2016) Parallel specification of competing sensorimotor control policies for alternative action options. Nat Neurosci 19:320–326
Haridas C, Zehr EP, Misiaszek JE (2005) Postural uncertainty leads to dynamic control of cutaneous reflexes from the foot during human walking. Brain Res 1062:48–62
Haridas C, Zehr EP, Misiaszek JE (2006) Context-dependent modulation of interlimb cutaneous reflexes in arm muscles as a function of stability threat during walking. J Neurophysiol 96:3096–3103
Hayashi R, Miyake A, Jijiwa H, Watanabe S (1981) Postural readjustment to body sway induced by vibration in man. Exp Brain Res 43:217–225
Holden M, Ventura J, Lackner JR (1994) Stabilization of posture by precision contact of the index finger. J Vestib Res 4:285–301
Jeka JJ, Lackner JR (1994) Fingertip contact influences human postural control. Exp Brain Res 100:495–502
Jeka JJ, Oie K, Schöner G, Dijkstra T, Henson E (1998) Position and velocity coupling of postural sway to somatosensory drive. J Neurophysiol 79:1661–1674
Jenner JR, Stephens JA (1982) Cutaneous reflex responses and their central nervous pathways studied in man. J Physiol 333:405–419
Kouzaki M, Masani K (2008) Reduced postural sway during quiet standing by light touch is due to finger tactile feedback but not mechanical support. Exp Brain Res 188:153–158
Lamont EV, Zehr EP (2007) Earth-referenced handrail contact facilitates interlimb cutaneous reflexes during locomotion. J Neurophysiol 98:433–442
Misiaszek JE (2006) Neural control walking balance: IF falling THEN react ELSE continue. Exerc Sport Sci Rev 34:128–134
Misiaszek JE, Vander Meulen J (2017) Balance reactions to light touch displacements when standing on foam. Neurosci Lett 639:13–17
Misiaszek JE, Forero J, Hiob E, Urbanczyk T (2016) Automatic postural responses following rapid displacement of a light touch contact during standing. Neuroscience 316:1–12
Misiaszek JE, Chodan SDC, McMahon AJ, Fenrich KK (2020) Influence of pairing startling acoustic stimuli with postural responses induced by light touch displacement. Appl Sci 10:382. https://doi.org/10.3390/app10010382
Oshita K, Yano S (2016) Effect and immediate after-effect of lightly gripping the cane on postural sway. J Physiol Anthropol 35:14. https://doi.org/10.1186/s40101-016-0096-4
Pearcey GEP, Zehr EP (2019) We are upright-walking cats: human limbs as sensory antennae during locomotion. Physiology 34:354–364
Peterka RJ (2002) Sensorimotor integration in human postural control. J Neurophysiol 88:1097–1118
Prochazka A (1989) Sensorimotor gain control: a basic strategy of motor systems? Prog Neurobiol 33:281–307
Prochazka A (1996) The fuzzy logic of visuomotor control. Can J Physiol Pharmacol 74:456–462
Rogers MW, Wardman DL, Lord SR, Fitzpatrick RC (2001) Passive tactile sensory input improves stability during standing. Exp Brain Res 136:514–522
Sozzi S, Crisafulli O, Schieppati M (2017) Haptic cues for balance: use of a cane provides immediate body stabilization. Front Neurosci 11:705. https://doi.org/10.3389/fnins.2017.00705
Thura D, Beauregard-Racine J, Fradet C-W, Cisek P (2012) Decision making by urgency gating: theory and experimental support. J Neurophysiol 108:2912–2930
Van Asten WN, Gielen CC, van der Gon JJ (1988) Postural movements induced by rotations of visual scenes. J Opt Soc Am A 5:1781–1789
Zaiontz C (2020) Real statistics using excel. Available online: http://www.real-statistics.com/. Accessed 28 Jan 2020
Zehr EP, Collins DF, Chua R (2001) Human interlimb reflexes evoked by electrical stimulation of cutaneous nerves innervating the hand and foot. Exp Brain Res 140:495–504
Acknowledgements
This work was funded through a Grant from the Natural Sciences and Engineering Research Council (NSERC) Canada (RGPIN-2017-04175 to JEM). The authors thank Dr. K. Fenrich for technical assistance with the data collection and Dr. D. F. Collins for providing comments on a draft of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Additional information
Communicated by Francesco Lacquaniti.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Misiaszek, J.E., Hackett, H., McMahon, A.J. et al. Influence of a light touch reference on cutaneous reflexes from the hand during standing. Exp Brain Res 239, 787–796 (2021). https://doi.org/10.1007/s00221-020-06019-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-020-06019-y