
Abstract
Reaching for an object is a basic motor skill that requires precise coordination between elbow, shoulder and trunk motion. The purpose of this research study was to examine age-related differences in compensatory arm–trunk coordination during trunk-assisted reaching. To engage the arm and trunk, an older and younger group of participants were asked to (1) maintain a fixed hand position while flexing forward at the trunk [stationary hand task (SHT)] and (2) reach to a within-arm’s reach target while simultaneously flexing forward at the trunk [reaching hand task (RHT)] (Raptis et al. in J Neurophysiol 97:4069–4078, 2007; Sibindi et al. in J Vestib Res 23:237–247, 2013). Both tasks were completed with eyes closed. Participants completed the two tasks with their dominant and non-dominant arms, and at both a fast and a preferred speed. On average, young and older participants performed in a similar manner in the SHT, such that they maintained their hand position by compensating for trunk movement with modifications of the elbow and shoulder joints. In the RHT, young and older participants had similar endpoint accuracy. This similarity in performance between young and older participants in the SHT and RHT tasks was observed regardless of the arm used or movement speed. However, for both tasks, movements in older adults were significantly more variable compared to younger adults as shown by the larger variability in arm–trunk coordination performance (gain scores) in the SHT and higher movement time variability in the RHT. Thus, results imply that older adults maintain their ability to coordinate arm and trunk movements efficiently during reaching actions but are not as consistent as younger adults.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In our daily life, we are constantly engaged in actions that can be performed by numerous combinations of joint rotations [degrees of freedom (DFs)], a characteristic known as “motor equivalence” (Lashley 1951; Bernstein 1967; Latash et al. 2007). The fundamental question of how the nervous system chooses movement patterns from a potential redundant set of DFs for a particular motor task (known as the redundancy problem), was first raised by Bernstein (1967). To deal with the problem of redundancy, it has been proposed that the nervous system constrains the number of DFs to work in groups known as synergies. Movement synergies may be engaged in a time-ordered sequence and controlled as a unit to meet a specific demand in motor output, such as stabilization of a movement trajectory or prevention of falling during trunk bending (Bernstein 1967; Jeannerod 1988; Latash et al. 2002).
Coordination between the arm and trunk has been studied extensively in healthy adults. For example, Kaminski et al. (1995) asked healthy young adults to reach to five targets, two which were within arm’s reach (i.e., near targets), and three beyond (i.e., far targets). They found that the trunk participated mainly in reaches to far targets that could not be attained by arm motion alone. When the trunk did contribute to the transportation of the hand to the target, its motion started simultaneously with the arm movement and continued until target contact. The involvement of trunk flexion had no effect on the path of the hand or the smoothness of its velocity profile. This has also been shown by Ma and Feldman (1995) who asked participants to make fast uncorrected planar movements of the right arm from a near to a far target placed in the ipsilateral work space at a 45° angle to the sagittal midline of the trunk. These reaching movements were combined with forward or backward sagittal motion of the trunk. Direction, positional error, curvature, and velocity profile of the hand trajectory remained invariant despite different trunk movements. Feldman et al. suggested that the invariance of the hand trajectories across conditions was due to two synergies: an arm transport synergy that coordinates the arm joints to bring the hand to the target and a compensatory arm–trunk synergy that decreases the influence of the trunk motion on hand position by additional changes at the arm joints (Ma and Feldman 1995; Pigeon and Feldman 1998). The compensatory synergy is flexible such that when the target is placed beyond arm’s reach (Mark et al. 1997), the degree of compensation (i.e., modifications in the arm joints to decrease the influence of the trunk movement on hand movement) is attenuated to permit the trunk to increase movement extent (Rossi et al. 2002). Adamovich et al. (2001) refer to these angular modifications in trunk-assisted reaching as “compensatory arm–trunk coordination.” According to Adamovich et al. (2001), sensory feedback (i.e., proprioceptive, cutaneous, and/or vestibular) that arises from the trunk motion may underlie the compensatory modifications in arm joint angles used to maintain the same hand trajectory regardless of changes in the number of degrees of freedom involved in the pointing task.
The role of sensory feedback in compensatory arm–trunk modifications has been examined in patients with altered sensation (i.e., deafferented patients) (Tunik et al. 2003) and patients with unilateral vestibular lesions (Raptis et al. 2007). Tunik et al. (2003) found that patients, who lacked cutaneous and proprioceptive sensitivity but had relatively intact vestibular function maintained their ability to adapt movements using compensatory arm–trunk coordination for reaching tasks in the absence of vision. Thus, it was suggested that vestibular signals evoked by head motion following trunk flexion may play a major role in the initiation, maintenance, and modification of compensatory arm–trunk coordination, as opposed to proprioceptive input. This proposal was later confirmed by Raptis et al. (2007) who found that patients with vestibulospinal pathology, caused by unilateral vestibular lesions, had deficits in adapting arm joint motion for reaching when trunk motion was imposed. In their study, participants were asked to lean forward with the trunk, in the absence of vision, while maintaining the same hand position or while moving the hand to a target. While healthy participants were able to maintain the required hand position or trajectory to targets by modifying elbow and shoulder joint rotation after trunk movement onset, patients with unilateral vestibular deficits did not compensate for 30–100% of the trunk displacement, leading to alterations in the final hand position or arm trajectory.
In a similar study, Sibindi et al. (2013) quantified the extent of arm–trunk compensation in patients with unilateral vestibular deficits using two different reaching tasks: (1) a stationary hand task (SHT), in which participants maintained their hand position while flexing their trunk, and (2) a reaching hand task (RHT), in which participants reached to a target while simultaneously flexing their trunk. Movements were made in the absence of vision. In the SHT, Sibindi et al. (2013) characterized the efficiency of compensatory arm–trunk coordination with a gain (g) score that ranged from a value of 1, when the effect of trunk motion on the hand position was fully compensated for (the hand remained in a stable position), to a value of 0 when no compensation occurred, and the trunk motion was transmitted to the hand (Raptis et al. 2007; Pigeon and Feldman 1998). The gain score was calculated based on reach endpoints from trials in which the trunk was free to move and those in which it was unexpectedly blocked. On average, gain scores in the patients (g = 0.67 ± 0.19) were significantly lower than those in healthy controls (g = 0.85 ± 0.07). In other words, the hand position of vestibular patients deviated more from the target during trials with trunk movement compared to healthy controls, indicating an increased influence of trunk motion on hand position. In the RHT, vestibular patients tended to over reach the target in trials in which the trunk was free, again indicating a decreased ability to compensate for the contribution of trunk motion on hand movement extent.
While deficits in arm–trunk coordination have been demonstrated in deafferented and vestibular patients, it is unclear to what extent motor equivalence is affected by aging. Aging is accompanied by a well-documented progressive decline in motor performance (Wallace et al. 1980; Janicke and Wrobel 1984), which includes movement coordination difficulties (Seidler et al. 2002), increased movement variability (Contreras-Vidal et al. 1998; Darling et al. 1989), and movement slowing (Diggles-Buckles 1993). These difficulties negatively impact the ability of older adults to perform daily activities independently and have been related to an array of changes in the central nervous system, as well as peripheral structures, such as sensory receptors, muscles, peripheral nerves, and joints (Welford 1977; Salthouse 1985; Stelmach and Worringham 1985). Moreover, with age there is degeneration within the vestibular system, including a decrease in the number of vestibular hair cells (Rosenthal and Rubin 1975; Gleeson and Felix 1987), a decline in the size and number of neurons that make up the vestibular nucleus (Lopez et al. 1997), and a reduction in the number of vestibular nerve fibers (Park et al. 2001). Given these difficulties, we anticipated that older individuals would have difficulties in compensating for trunk motion in the SHT and RHT.
The aim of this study was to assess compensatory arm–trunk coordination during trunk-assisted reaching in healthy older adults over the age of 60, using the SHT and the RHT. Within our experimental design we considered the influence of movement speed and hand used. Specifically, participants performed the task at two speeds, a comfortable speed (similar to Sibindi et al. 2013) and a fast speed (i.e., as fast as possible). Since aging is characterized by slowness in motor performance, performance at two speeds allowed us to compare performance across older and younger adults when performing the tasks at a similar speed (e.g., the fast speed for older adults and the comfortable speed for younger adults). As well, participants completed all movements with their dominant and non-dominant arms, since reaching and rapid aiming movements are typically more accurate when completed with the dominant compared to the non-dominant arm (Roy and Elliott 1989; Carson et al. 1993). We hypothesized that, compared to healthy young adults, older individuals would: (1) in the SHT, show an increase of the influence of trunk motion on hand position; i.e., decrease in the ability to compensate for trunk movement with appropriate angular modifications at the elbow and shoulder joints, and (2) in the RHT, exhibit greater endpoint deviation; i.e., greater deviation of the index finger position when the trunk was involved in the reaches (free-trunk trials) compared to reaches without the trunk (blocked-trunk trials). Moreover, based on previous literature, we hypothesized that both groups would perform the tasks better with their dominant hand (Roy and Elliott 1989; Carson et al. 1993) and when moving at their preferred speed (Seidler-Dobrin and Stelmach 1998; Messier et al. 2003) (i.e., better compensation for trunk movement in the SHT and less arm deviation in the RHT).
Methods
Participants
Two groups of participants were recruited: 18 healthy young adults (mean age = 24.3 ± 2.9 years), and 18 gender-matched healthy older adults (mean age = 72.1 ± 2.4 years). All participants had no musculoskeletal, neurological, or cognitive deficits that would interfere with the performance of the experimental tasks [Dizziness Handicap Inventory mean score = 1.7/100 (Jacobson and Newman 1990), joint position sense test mean score = 8/8, Ottawa Sitting Scale mean score = 38.6/40 (Thornton and Sveistrup 2010), Monteral Cognitive Assessment mean score (only older adults) = 27.7/30 (Nasreddine et al. 2005)]. As well, all participants were right-handed as indicated by their responses to the 10-item Edinburgh Handedness Inventory (mean score = + 82.7 ± 17.9, where scores > + 40 indicate strongly right-handed; Oldfield 1971). All participants provided informed consent prior to the start of the experiment in accordance with the ethical guidelines set by the University of Ottawa’s Research Ethics Board.
Apparatus
The VICON motion capture system (VICON motion systems, UK; 3D resolution 2.5 mm), including 7 cameras and 8 reflective markers, was used to record movement kinematics. Five markers were placed on the upper limb being tested [index fingertip (endpoint), radial styloid (wrist), lateral epicondyle of humerus (elbow), ipsilateral acromion (ipsi shoulder), and contralateral acromion (contra shoulder)], and additional markers were placed on the middle of the sternum (trunk), forehead, and on the target. Data were recorded at a sampling rate of 60 Hz for 5 s.
Experimental set-up
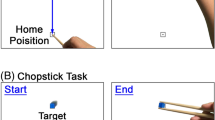
Participants were seated on a stool (i.e., chair with no back support and no arm rests), with their feet on the ground, shoulder width apart, and facing the motion tracking system (Portable Cartesian Stand of VICON; Fig. 1a). Participants wore a harness, fastened posteriorly at the level of the scapulae and held by a second experimenter. A fixed target was positioned at approximately 60% of the participant’s arm length (from the medial axillary border of the shoulder to the tip of the index finger) and was represented by a “yoyo” attached to a belt hanging from the ceiling and positioned at nose level. Participants performed one calibration task and two motor tasks (SHT and RHT), as described below and illustrated in Fig. 1.

Experimental set-up and procedures. a Marker positions: reflective markers were placed on the upper limb being tested [index fingertip (endpoint), radial styloid (wrist), lateral epicondyle of the humerus (elbow), ipsilateral acromion (ipsi shoulder), and contralateral acromion (contra shoulder)], and additional markers were placed on the middle of the sternum (trunk), forehead, and on the target (not shown in the figure). b Calibration: participants were seated with their testing arm held at nose level and flexed at the elbow so that their index finger was positioned under the fixed target. Participants were instructed to lean forward; i.e., to flex their trunk as far as possible. A foam constraint was used to make sure that the arm and trunk were fixed relative to one another. c Stationary hand task: participants were seated with their testing arm flexed at the elbow at nose level directly underneath the target without touching it. In this task, participants were asked to maintain their arm position under the target location and flex their trunk forward, bringing their nose to the target. d Reaching hand task: participants were seated with the testing arm positioned on an arm rest which was placed next to the trunk at hip joint level to ensure a multi-joint movement. In this task, participants were asked to move their testing arm to the target, while simultaneously flexing the trunk forward
-
(a)
Calibration
The aim of the calibration procedure was to quantify the maximal hand/index finger displacement possible when the participant leaned forward at the trunk, with their arm and trunk fixed relative to each another. Each participant completed 10 calibration trials per arm. Participants were seated with their testing arm held at nose level and flexed at the elbow (80° on average) so that their index finger was positioned under the fixed target. Participants were instructed to lean forward; i.e., to maximally flex their trunk. The arm was attached to a foam form strapped to the trunk that was used to make sure that the arm and trunk were fixed relative to one another (i.e., arm and trunk moved forward as one unit, Fig. 1b).
-
(b)
Stationary hand task
For the SHT, participants were seated with their tested arm flexed at the elbow at nose level directly underneath the target without touching it. Participants were instructed that upon hearing a verbal “go” signal, they should close their eyes and lean forward with their trunk in a single uncorrected movement (15–20 cm shoulder displacement in the sagittal plane from an upright posture; Free-trunk trials). The final position was held for 2 s before participants returned their trunk back to the starting position (Fig. 1c). After completing the movement, participants opened their eyes. Participants were instructed to complete the trunk flexion while maintaining a fixed arm position in space. Four sets of 10 trials (40 trials) were completed for each hand and at two movement speeds (see Introduction) for a total of 160 trials. A 2-min rest was taken after each set of 10 trials. The first 40 trials for each arm were done as fast as possible, and the subsequent 40 were done at a preferred, comfortable speed.
During the SHT, the trunk movement was unexpectedly blocked on a subset of trials (40%) by an examiner who held the handle attached to the back of the tightly fitted harness strapped to the participant’s chest (Blocked-trunk trials). When blocked, the trunk movement was arrested for the entire trial. In the blocked-trunk trials, participants were still able to maintain their initial hand position. The percentage of the blocked-trunk trials was chosen based on previous research suggesting that 40% is sufficient to minimize anticipation of the upcoming trunk condition (Adamovich et al. 2001; Raptis et al. 2007).
-
(c)
Reaching hand task
For the RHT, participants were seated with the tested arm positioned on an arm rest placed next to the trunk at hip level to stabilize the initial position. Participants were instructed to move their tested arm to the target, while simultaneously flexing the trunk forward (as in the SHT). At a verbal “go” signal, participants closed their eyes and reached to the target while simultaneously flexing and leaning forward with the trunk (see Fig. 1d). When participants believed that their hand had reached the target, they were instructed to hold the final hand position for 2 s, and then they were verbally prompted to return to the start position and open their eyes. Participants completed the task at two speeds with both arms, once moving as quickly as possible and once moving at their preferred, comfortable speed. For each arm and speed, participants completed 4 sets of 10 trials (40 trials) with a 2 min rest period between each set of trials, for a total of 160 trials. In 40% of trials, trunk movement was unexpectedly blocked, while the participant was required to reach the same target position as in free-trunk trials.
Each participant performed the SHT and RHT with the same arm before testing the opposite arm. The order of the testing arm (right or left) was counterbalanced across participants. Within each task, the type of trial (free versus blocked-trunk) was also randomized.
Data analysis
Data from each task were analyzed using custom-written software in MATLAB version R2013a and SPSS version 24. The start and end of the trunk movement were determined as the times at which the tangential velocity of the sternum marker first surpassed and remained above or fell and remained below 10% of the trunk peak velocity, respectively.
Calibration task
Trunk (sternum marker) and arm displacement (i.e., index finger marker) in the sagittal plane were determined according to the anterior–posterior (A/P) distance covered (i.e., position at the end of the movement relative to the position at the start of the movement in the sagittal plane) and expressed in cm. The deviation in the finger position that was determined from the calibration trials (hm) represents the maximal horizontal deviation in the index finger position that would be expected if the trunk motion were fully transmitted to the hand (i.e., this mimics what would occur if the arm joint angles did not compensate for the trunk motion at all).
Stationary hand task
To determine arm–trunk coordination, a gain score (g) was calculated in the sagittal (y) plane (Raptis et al. 2007; Sibindi et al. 2013). Specifically, the gain score was calculated for each participant for each hand and speed using the following equation: g = 1–(h/hm); where h was the average horizontal deviation of the hand position in free- compared to blocked-trunk trials and hm was determined from the calibration trials. Given that the amount of trunk displacement could be different between calibration and free-trunk trials, hand displacement was normalized according to this difference. A score of g = 1 would occur when elbow flexion and shoulder horizontal flexion fully compensated for trunk motion resulting in no hand movement from the initial position (h ~ 0). Conversely, a score of g = 0 indicates that no compensation occurs (h = hm), and the hand moves with the trunk. It should be noted that in the gain score calculation, the influence of trunk motion on final hand position was considered instead of movement accuracy with respect to the target, as according to Pigeon et al. (2000), participants typically make systematic errors that, without knowledge of results (as was the case in our study), are reproduced in repeated trials. These errors were not the focus of our study and thus, to avoid the confounding effect of vision-dependent systematic errors on gain scores, coefficient h was determined by calculating the deviation in the final positions of the index finger in blocked-trunk trials from the respective positions in free-trunk trials. In addition to movement time and gain score, trunk displacement and hand deviation (h from the gain score equation) were computed and expressed in cm. Trunk displacement was defined as the anterior–posterior (A/P) distance moved by the trunk in the sagittal plane during free-trunk trials, while hand deviation refers to the A/P difference of the final hand position in the free- compared to blocked-trunk trials.
Reaching hand task
For the RHT, the start and end of movement for free- and blocked-trunk trials were defined as the times at which the tangential velocity of the finger marker first surpassed and remained above or fell and remained below 10% of finger peak velocity, respectively. Movement time was calculated as the difference between these two time points. An error measure indicating the difference (d) in final hand position in the free- versus blocked-trunk trials was used to determine compensatory arm–trunk coordination during the RHT (i.e., hand deviation). This difference was calculated in 2D from the sagittal (horizontal and vertical) coordinates of the finger marker in the free- and blocked-trunk trials and was normalized by each participant’s arm length to allow comparison between groups. Specifically, this error measure was expressed in relation to the ratio (r) of the arm length of the participant to the group mean arm length. Thus, for each participant, the normalized difference (dn) was computed as dn = r·d. A small difference value indicated that participants were able to compensate for the effect of trunk movement on hand position. In addition, the 2D positions of the hand relative to the fixed target position in both free- and blocked-trunk trials were computed and expressed in cm.
Statistical analysis
Mean trunk and hand (i.e., index finger) displacements in the calibration task were analyzed in a two group (old vs. young) × 2 hand (dominant/right vs. non-dominant/left) mixed analysis of variance (ANOVA) with repeated measures (RM) on the last factor. We had initially hypothesized that older participants would move more slowly at their preferred speed compared to older adults. As outlined below, this was not the case. Thus, for each variable that was analyzed in the SHT and RHT, mean values and variability (standard deviations) for each kinematic variable were compared across participants using a two group × 2 hand × 2 speed (preferred vs. fast) mixed ANOVA with RM on the last two factors. Mean movement time (MT) and variability in the RHT were analyzed in a two group × 2 hand × 2 speed × 2 trial type (free-vs. blocked-trunk trials). For all analyses, differences with a probability of < 0.05 were considered significant and Bonferroni post hoc analyses were performed to determine the locus of the differences.
Results
-
1.
Calibration task
During calibration trials, trunk displacement did not differ between groups or hands. The average trunk displacement was 17.9 cm for older adults and 17.3 cm for younger adults with the right arm, and 17.0 cm and 16.2 cm, respectively, for the left arm. Similarly, the average hand/finger displacement caused by trunk movement was similar between groups and hands. Movement of the trunk led to an average hand/finger displacement of 14.0 cm and 13.1 cm when the right and left hands were used, respectively.
-
2.
Stationary hand task
-
(a)
Trunk movement time (MT)
Overall, when participants performed the task at their preferred, comfortable speed, both groups completed the task in approximately 1.6 s, using either arm (Table 1). When participants were instructed to perform the task as fast as possible, older participants executed the movement faster than in the preferred speed condition only when using their left arm (Table 1). In contrast, younger participants were able to complete the task faster using both arms (Table 1). In accordance with these observations, ANOVA revealed a significant group × hand × speed interaction [F(1,34) = 20.85, p < 0.001]. Post hoc analysis showed that trunk movement time differed significantly between speed conditions for the same arm in the younger group but not in the older group. In addition, between groups, older adults made significantly slower trunk movements when moving as fast as possible while maintaining their right hand position under the fixed target (p = 0.043).
While variability in MT did not differ significantly between groups [F(1,34) = 2.61, p = 0.12], there was a significant group × hand × speed interaction [F(1,34) = 4.90, p = 0.03] (Table 1). In particular, post hoc analysis revealed that in the older adults, MT was significantly more variable when the task was performed with the right hand compared to the left hand in the fast speed condition (p < 0.001).
-
(b)
Trunk displacement
The harness was effective in blocking trunk movement, such that trunk flexion during blocked-trunk trials was minimal for both groups with both hands. The average amount of trunk flexion during blocked-trunk trials for both groups was 1.1 cm when the right hand was at the target and 1.0 cm when the left hand was at the target across speed conditions. In free-trunk trials, trunk displacement was similar to the 17.1 cm in the calibration trials. Specifically, collapsed across speed conditions, average trunk displacement was 16.8 cm, with a corresponding variability of 5.2 cm. These values did not vary between groups, hands or speed.
-
(c)
Hand deviation
Example endpoint positions of the hand relative to the target in the horizontal plane are shown in Fig. 2a, c for a typical younger and older participant. The hand in free-trunk trials deviated from the target by 1.7 cm more on average than in blocked-trunk trials when the task was performed using the right hand and 1.2 cm more on average when the task was performed with the left hand, collapsed across participants and speed conditions. ANOVA revealed no main effects of group or hand (Table 1). However, there was a significant hand × speed interaction [F(1,34) = 4.17, p = 0.04], such that participants had a larger hand deviation when they performed the task using their right hand compared to their left hand, but this was only significant in the fast speed condition (p = 0.01) (Table 1).

Horizontal endpoint position errors relative to the target for one younger adult (black squares) and one older adult (white squares) in the SHT (a, c) when moving the right hand at a comfortable speed. 2-Dimensional endpoint position errors relative to the target for one younger adult (black squares) and one older adult (white squares) in the RHT (b, d) when moving the right hand at a comfortable speed. The endpoint errors for the older adult were more variable than the younger adult in the SHT when the trunk was involved in the movement, as seen by the scatter in endpoint positions across trials in a
As seen in Fig. 2a, older adults were more variable in their ability to maintain their hand position in the free-trunk trials using either hand and in both speed conditions compared to younger adults [effect of group: F(1,34) = 7.72, p < 0.001] (Table 1). Analyses also revealed a significant hand × speed interaction [F(1,34) = 5.31, p = 0.02] when the trunk was blocked. Post hoc analyses indicated that the variability in right hand deviation increased significantly when the movements were executed as fast as possible compared to when the movements were completed at the preferred speed for both groups (Table 1).
-
(d)
Gain
Participants in both groups were able to compensate for the influence of trunk motion on their hand position regardless of hand used and movement speed (Fig. 3a). Although gain scores were slightly lower in older adults compared to younger participants, across both hands and both movement speeds, there were no differences between groups, hands or speeds. In the older participants, the mean gain score was 0.75 across both hands and speed conditions. Similarly, for the younger participants, the mean gain score was 0.81 across both hands and speed conditions.

a Mean gain scores in the stationary hand task. Younger and older participants performed the task in a similar manner with high gain scores (≈ 0.7), regardless of the hand being used and the speed of the movement completed. b Variability in gain scores in the SHT. Performance of older adults was significantly more variable compared to younger participants using both hands, and at both movement speeds. Error bars reflect standard errors of the mean
Although both groups were able to perform the SHT with a high level of compensation, as reflected in the high gain scores, older adults were significantly more variable in their performance compared to younger participants, using either hand and at both speed conditions [main effect of group: F(1,34) = 6.89, p = 0.01] (Fig. 3b).
-
3.
Reaching hand task (RHT)
-
(a)
Movement time (MT)
In the preferred speed condition, both groups completed the task in approximately 1.2 s using either hand in both types of trials (i.e., in free- and blocked-trunk trials) (Table 2). Similar to the SHT, in the fast speed condition, younger participants were able to execute the movement faster with both hands in both types of trials, while older adults did not move faster using either hand or in either type of trial (Table 2). Analysis revealed a significant group × hand × speed × trial type interaction [F(1,34) = 7.00, p = 0.01]. Post hoc analysis showed that in the fast speed condition, older adults were significantly slower in their performance compared to younger participants, using either hand, in both types of trials (p = 0.01 for both hands in both types of trials). In the preferred speed condition, although older adults showed a trend of moving slower than younger participants, the difference was not significant between groups with either hand and in either type of trial (all p > 0.08).
With respect to MT variability in free- and blocked-trunk trials, there were significant main effects of group [F(1,34) = 11.39, p < 0.001], trial type [F(1,34) = 5.18, p = 0.02], and a hand × trial type interaction [F(1,34) = 5.33, p = 0.03]. When moving at a fast speed, older adults were significantly more variable than the younger adults in both types of trials, using either hand. In contrast, when moving at their preferred speed, older adults were more variable than the younger adults only when the left hand was used for both types of trials (p < 0.001). (Table 2).
-
(b)
Trunk displacement
Similar to the SHT, trunk flexion was minimal during the blocked-trunk trials (on average 1.35 cm across hands and speed conditions). Moreover, there were no effects of group, hand, speed or any interaction with respect to the mean or the variability of trunk displacement. Collapsed across speeds, older adults had an average trunk displacement of 18.8 cm when reaching with the right hand and 17.6 cm when reaching with the left hand (Table 2). This was similar to the average trunk displacement in younger adults, which was 18.2 cm and 17.0 cm when reaching with the right and left hands, respectively (Table 2). In terms of variability, there was no significance difference between groups. When reaching with the right hand, variability in trunk displacement was 4.8 cm for older adults and 3.9 cm for younger adults, while when reaching with the left hand, it was 4.8 cm for older adults and 4.7 cm for younger ones, collapsed across speed conditions (Table 2).
-
(c)
Hand deviation
Example 2D distance errors relative to the target are shown in Fig. 2b, d for a typical younger and older participant. Overall, participants reached 7.9 cm and 6.6 cm further from the target (i.e., overshot the target) in free- and blocked-trunk trials, respectively, with no differences in reaching errors between trials types for group, hand or speed (Fig. 4a). From Fig. 4b it appears that older adults had greater variability in final hand position in the free-trunk trials compared to younger adults; however, the difference between groups was not significant (only a trend) [main effect of group: F(1,34) = 0.37, p = 0.72] (Fig. 4b). As well, there was no difference in variability of final endpoint positions between groups in the blocked-trunk trials.

a Normalized mean hand position differences in 2D in the RHT (hand deviation). On average participants reached 1.3 cm further in the free-trunk trials compared to blocked-trunk trials. b Variability in normalized 2D final hand position during the free-trunk trials in the RHT. c Variability in normalized 2D final hand position during the blocked-trunk trials in the RHT. In both b, c, older adults showed a trend of greater variability compared to younger adults but there was no significant effect of group. Error bars reflect standard errors of the mean
Discussion
We examined age-related differences in arm–trunk coordination during two motor tasks; the Stationary Hand Task and the Reaching Hand Task. In the SHT, both groups were able to compensate for trunk motion in the free-trunk trials by appropriate changes in elbow and shoulder joint rotations as demonstrated by high gain scores (mean score range between 0.75 and 0.81) and minimal hand deviations (~ 1.4 cm compared to the blocked-trunk trials) regardless of the hand used and movement speed. In the RHT, young and older adults made similar small overshoot errors (~ 1.3 cm) in free- compared to blocked-trunk trials, for both hands and movement speeds. This small difference suggests that participants were able to compensate for the effect of trunk movement on hand position. On the other hand, performance of older adults was significantly more variable compared to the younger adults as shown by the larger variability in gain scores in the SHT, greater variability in final hand positions when the trunk was involved in the SHT, and higher MT variability in the RHT.
Stationary hand task
The goal for this task was to keep the hand stationary under the fixed target position while flexing the trunk forward. Participants in both groups were able to reduce the influence of trunk motion on the hand position as demonstrated by high gain scores, reflecting that the hand remained relatively stationary. These findings resemble those previously reported for young and middle-aged healthy participants (Adamovich et al. 2001; Raptis et al. 2007; Sibindi et al. 2013). Previous literature has suggested that when the trunk is intentionally involved in reaching to targets placed within arm’s reach, the influence of the trunk movement on the hand position is compensated for by appropriate rotations of the elbow and shoulder joints (Ma and Feldman 1995; Pigeon et al. 2000; Adamovich et al. 2001). In neurologically intact participants, this compensation has been suggested to be driven by afferent signals (proprioceptive and/or vestibular) elicited by the trunk movement and transmitted to the arm muscles (Adamovich et al. 2001; Tunik et al. 2003; Raptis et al. 2007). Specifically, trunk motion is accompanied by vestibular signals from the associated head movement. These signals can be sent to the spinal cord by different descending pathways such as the vestibulospinal and reticulospinal tracts (Lobel et al. 1998), influencing motoneurons of arm muscles and resulting in compensatory changes in the arm joint angles during movement. Moreover, trunk flexion evokes proprioceptive signals from muscles in the hip, trunk and neck in addition to proprioceptive signals from the joints and skin. These signals can be sent to arm motoneurons by short- and long-loop pathways (propriospinal and transcortical tracts) resulting in compensatory arm movements (Adamovich et al. 2001; Bresciani et al. 2002b, 2005; Mars et al. 2003; Guillaud et al. 2006). Since all of our participants were healthy with no musculoskeletal or neurological impairments, these sensory feedback signals would be expected to be available during the performance of the motor task, potentially leading to similarities in the degree of compensation regardless of age.
Reaching hand task
Hand deviations were small in both groups of participants in the RHT despite the task complexity. Specifically, participants in both groups were able to neutralize the effect of trunk movement on hand displacement. These results are also consistent with the findings of Archambault et al. (1999) and Adamovich et al. (2001), who reported similar compensation in healthy young participants, as well as Raptis et al. (2007) and Sibindi et al. (2013), who showed good compensation for trunk movement in healthy middle-aged participants. It has been suggested that while the brain issues central commands for transporting the hand to the target and flexing the trunk, compensatory arm movements are not issued in the same way (i.e., modifications in arm joint angles to diminish the influence of the trunk flexion on the hand). Instead, compensation emerges from vestibular and proprioceptive signals evoked by the trunk movement, leading to a reorganization of the arm movement synergy. Control systems have also been suggested to modulate the degree of compensation by “gating” the afferent signals evoked by the trunk movement to provide the appropriate contribution of the trunk to hand transport based on the task requirements (e.g., whether the target is within or beyond the reach of the arm) (Adamovich et al. 2001).
The difference in movement speed between groups
Younger and older adults had similar preferred speeds when completing both the SHT and RHT. Younger adults were able to increase the speed of their movements when instructed to move faster. Older adults were also able to increase their movement speed, but only when using their left hand. Previous research has suggested that movement slowing with aging may be strategic in older adults such that they may select a strategy in which greater emphasis is placed on response accuracy leading to a decrement in speed of performance (Seidler-Dobrin and Stelmach 1998).
In contrast to our hypothesis, the performance of older adults with respect to mean outcome measures and variability was similar across instructed movement speeds. One reason for this similarity across speed conditions, may be due to their inability to increase their movement speed in either task with the right hand. Although younger adults were able to increase their movement speed significantly in both tasks and with both hands, the increase in movement speed did not impact their movement kinematics (i.e., gain in SHT and hand deviation in RHT). In a previous study, Messier et al. (2003) had older adult participants make reaching movements to four remembered visual targets at slow, natural, and fast speeds. Their results showed that participants made larger spatial errors at both slow and fast speeds compared to their natural speed. However, most movement kinematic features were invariant across speed conditions. It is possible that their subjects were able to sustain fairly accurate and straight hand trajectories for multi-joint reaching movements at different speeds regardless of changes in inter-segmental dynamics or interaction torques (Morasso 1981; Hollerbach and Flash 1982; Adamovich et al. 1994; Gordon et al. 1994b).
Handedness
We found that the hand used did not influence movement kinematics in either the SHT or RHT (specifically, gain and hand deviation scores). Similar findings have been shown in other studies. For example, when Al-Senawi and Cooke (1985) instructed participants to move a lever in the horizontal plane to different distances (i.e., 5°, 10°, 20°, 30°, and 40°) with each arm at a self-selected speed, there was no difference in spatial error between the arms and the velocity profiles were nearly identical. In another study, Sainburg and Kalakanis (2000) asked participants to move their hand to targets that required 20° of elbow extension and either 5°, 10°, or 15° of shoulder extension without visual feedback using both the dominant and non-dominant arms. Although each arm used a different strategy to reach the target (i.e., the dominant arm used elbow and shoulder torques synergistically to move the upper arm but the same torques countered one another in the non-dominant arm), accuracy was similar for both limbs. Such findings support the notion of motor equivalence (Head 1920; Bartlett 1932; Bernstein 1967; Schmidt 1975).
Interjoint coordination
Our findings in both motor tasks did not support our hypotheses. Since aging results in a decline in sensorimotor control and functioning, we expected that older participants would show an increase of the influence of trunk motion on hand position; i.e., a decrease in the gain score in the SHT, and exhibit greater hand deviation; i.e., greater deviation of the finger position in the free- compared to blocked-trunk trials in the RHT. Few studies have evaluated the effects of aging on coordination. Moreover, most previous studies have focused on inter-limb rather than intra-limb coordination, with inconclusive findings. For example, Stelmach et al. (1988) found greater reaction time differences between the two hands for older adults compared to younger adults during bimanual aiming movements. On the other hand, Rothstein et al. (1989) showed no age effects on inter-limb differences in movement initiation and termination times. Recently, Seidler et al. (2002) examined intra-limb coordination in older adults during the performance of multi-joint arm pointing movements to four different targets. One target could be reached using elbow extension only and the remaining three required a coordination between elbow extension and shoulder horizontal flexion. Older adults co-activated antagonist muscles to a greater extent than young adults for single-joint actions, which compensated for heightened muscle force variability leading to smoother movements. On the other hand, older adults did not apply this compensatory mechanism to movements that were more complex, i.e., double-joint movements. Instead, they decreased co-activation levels when transitioning from single- to double-joint actions, while young adults increased their elbow joint co-activation. Decreasing co-activation was accompanied by movements that became less smooth and less accurate as shoulder joint contribution increased. Based on these results, Seidler et al. (2002) concluded that increasing co-activation may be difficult for older adults to implement in double-joint actions due to increases in complexity of movement planning and associated energy costs. Therefore, older adults appeared to use co-activation in a fundamentally different manner from the younger adults. In our experiment, similar to younger adults, older adults showed good compensation for trunk motion in the SHT and attained similar hand deviation errors in the RHT. However, performance of older adults was significantly more variable in the SHT and trended to greater variability in the RHT compared to younger participants. We did not investigate the activation in upper-limb muscles while performing the tasks. Further investigation regarding the activation in upper-limb agonist and antagonist muscles is needed to determine what compensatory strategy older adults used that resulted in similar performance to the younger participants but accompanied with a significant increment in variability.
Variability in performance (SHT and RHT)
Performance of older adults was more variable compared to younger participants in both the SHT and RHT (see Tables 1, 2). Variability in motor output can be defined as the unintentional variations in the output of voluntary contractions (Christou 2010). It can be found within a trial (e.g., movement trajectory) or from trial to trial (e.g., endpoint variability) (Christou 2010). It is well documented that older adults exhibit greater motor output variability compared to younger adults. Literature suggests that both forms of variability (within trial and between trials) are associated with greater end-point error in force, displacement and time in older adults (Christou et al. 2007; Christou 2011), which influence their ability to move smoothly and accurately (Christou and Tracy 2005). Moreover, increased variability may decrease the ability to learn new tasks and adapt to changing environments, thus compromising their independence (Christou 2009). The increment in variability in movements of older adults has been linked to altered activation of the involved muscles due to structural and neural changes associated with aging in higher centers (e.g., death of cortical neurons) (Eisen et al. 1996) and the spinal cord (e.g., motor unit reorganization) (Enoka et al. 2003). According to Darling et al. (1988), who compared muscle EMG patterns and trajectory variability between movements made by older participants with those of younger ones during an aiming task, the increase in variability of movements with age can be caused by factors affecting the production of joint torques necessary for acceleration and deceleration of the limb. These factors include: (1) changes in the motor neuron population and firing rate variability, and (2) abnormal control of the phasic and tonic antagonist muscle activity. Moreover, the inconsistency in the performance of older adults in their ability to maintain endpoint performance (i.e., maintain a stable hand position) in reaching tasks requiring additional DFs (i.e., trunk movement) implies decreases in movement adaptability (i.e., capacity of motor equivalence) (Raptis et al. 2007; Sibindi et al. 2013; Tunik et al. 2004).
Conclusion
To summarize, healthy older adults were able to maintain a stable hand position when reaching movements involved the trunk. The preservation of hand position was achieved by active compensatory changes in the arm joint angles nullifying the influence of the trunk motion on hand position. The integration of additional degrees of freedom (trunk) into movement is assumed to be driven by afferent signals (proprioceptive and/or vestibular) evoked by the trunk motion and transmitted to the arm muscles. Despite the fact that older adults were able to coordinate arm and trunk movements efficiently during the reaching actions, they were not as consistent as younger adults. This increase in variability across movements could be linked to structural and neural changes at higher centers (i.e., brain and spinal cord) associated with aging and may suggest a reduction in the capacity of the nervous system to achieve motor equivalence (i.e., reduced movement adaptability).
References
Adamovich SV, Berkinblit MB, Smetanin B, Fookson O, Poizner H (1994) Influence of movement speed on accuracy of pointing to memorized targets in 3D space. Neurosci Lett 172:171–174
Adamovich SV, Archambault PS, Ghafouri M, Levin MF, Poizner H, Feldman AG (2001) Hand trajectory invariance in reaching movements involving the trunk. Exp Brain Res 138:288–303
Al-Senawi D, Cooke JD (1985) Matching of movements made independently by the two arms in normal humans. J Mot Behav 17:321–334
Archambault P, Pigeon P, Feldman AG, Levin MF (1999) Recruitment and sequencing of different degrees of freedom during pointing movements involving the trunk in healthy and hemiparetic subjects. Exp Brain Res 126:55–67
Bartlett FC (1932) Remembering: a study in experimental and social psychology. Cambridge University Press, Cambridge
Bernstein N (1967) The coordination and regulation of movements. Pergamon Press, Oxford
Bresciani JP, Blouin J, Sarlegna F, Bourdin C, Vercher JL, Gauthier GM (2002b) On-line versus off-line vestibular-evoked control of goal-directed arm movements. Neuroreport 13:1563–1566
Bresciani JP, Gauthier GM, Vercher JL, Blouin J (2005) On the nature of the vestibular control of arm-reaching movements during whole-body rotations. Exp Brain Res 164(4):431–441
Carson RG, Elliott D, Goodman D, Thyer L, Romeo C, Eric AR (1993) The role of impulse variability in manual-aiming asymmetries. Psychol Res 55:291–298
Christou EA (2009) Aging and neuromuscular adaptations with practice. In: Shinohara M (ed) Advances in neuromuscular physiology of motor skills and muscle fatigue. Research Signpost, Thiruvananthapuram, pp 65–79
Christou EA (2010) Motor output variability. In: Kompoliti K, Verhagen-Metman L (eds) Encyclopedia of movement disorders. Academic Press, Oxford, pp 202–204
Christou EA (2011) Aging and variability of voluntary contractions. Exerc Sport Sci Rev 39:77–84
Christou EA, Tracy BL (2005) Aging and motor output variability. In: Davids K, Bennett S, Newell K (eds) Movement system variability. Human Kinetics, Champaign, pp 199–215
Christou EA, Poston B, Enoka JA, Enoka RM (2007) Different neural adjustments improve endpoint accuracy with practice in young and old adults. J Neurophysiol 97:3340–3350
Contreras-Vidal JL, Teulings HL, Stelmach GE (1998) Elderly subjects are impaired in spatial coordination in fine motor control. Acta Physiol (Oxf) 100(1–2):25–35
Darling WG, Cole KJ, Abbs JH (1988) Kinematic variability of grasp movements as a function of practice and movement speed. Exp Brain Res 73:225–235
Darling WG, Cooke JD, Brown SH (1989) Control of simple arm movements in elderly humans. Neurobiol Aging 10:149–157
Diggles-Buckles V (1993) Age-related slowing. In: Stelmach GE, Homberg V (eds) Sensorimotor impairment in the elderly. Kluwer Academic, Norwell
Eisen A, Entezari-Taher M, Stewart H (1996) Cortical projections to spinal motoneurons: changes with aging and amyotrophic lateral sclerosis. Neurology 46(5):1396–1404
Enoka RM, Christou EA, Hunter SK, Kornatz KW, Semmler JG, Taylor AM, Tracy BL (2003) Mechanisms that contribute to differences in motor performance between young and old adults. J Electromyogr Kinesiol 13:1–12
Gleeson MJ, Felix H (1987) A comparative study of the effect of age on the human cochlear and vestibular neuroepithelia. Acta Otolaryngol (Stockh) Suppl 436:103–109
Gordon J, Ghilardi MF, Cooper SE, Ghez C (1994b) Accuracy of planar reaching movements. II. Systematic extent errors resulting from inertial anisotropy. Exp Brain Res 99:112–130
Guillaud E, Gauthier G, Vercher JL, Blouin J (2006) Fusion of visuo-ocular and vestibular signals in arm motor control. J Neurophysiol 95:1134–1146
Head H (1920) Studies in neurology, vol 2. Oxford University Press, London
Hollerbach JM, Flash T (1982) Dynamic interactions between limb segments during planar arm movements. Biol Cybern 44:67–77
Jacobson GP, Newman CW (1990) The development of the Dizziness Handicap Inventory. Arch Otolaryngol Head Neck Surg 116(4):424–427
Janicke B, Wrobel D (1984) Changes in motor activity with age and the effects of pharmacologictreatment. Exp Gerontol 19:321–328
Jeannerod M (1988) The Neural and behavioural organization of goal-directed movements. Clarendon Press, Oxford
Kaminski TR, Bock C, Gentile AM (1995) The coordination between trunk and arm motion during pointing movements. Exp Brain Res 106:457–466
Lashley KS (1951) The problem of serial order in behavior. In: Jeffress LA (eds). Cerebral mechanisms in behavior (the Hixon symposium). Wiley, New York
Latash ML, Scholz JF, Danion F, Schöner G (2002) Finger coordination during discrete and oscillatory force production tasks. Exp Brain Res 146:419–432
Latash ML, Scholz JP, Schöner G (2007) Toward a new theory of motor synergies. Mot Control 11:276–308
Lobel E, Kleine JF, Le Bihan D, Leroy-Willig A, Berthoz A (1998) Functional MRI of galvanic vestibular stimulation. J Neurophysiol 80:2699–2709
Lopez I, Honrubia V, Baloh RW (1997) Aging and the human vestibular nucleus. J Vestib Res 7(1):77–85
Ma S, Feldman AG (1995) Two functionally different synergies during arm reaching movements involving the trunk. J Neurophysiol 73:2120–2122
Mark LS, Nemeth K, Gardner D, Dainoff MJ, Paasche J, Duffy M, Grandt K (1997) Postural dynamics and the preferred critical boundary for visually guided reaching. J Exp Psychol Hum Percept Perform 23:1365–1379
Mars F, Archambault PS, Feldman AG (2003) Vestibular contribution to combined arm and trunk motion. Exp Brain Res 150:515–519
Messier J, Adamovich S, Berkinblit M, Tunik E, Poizner H (2003) Influence of movement speed on accuracy and coordination of reaching movements to memorized targets in three-dimensional space in a deafferented subject. Exp Brain Res 150(4):399–416
Morasso P (1981) Spatial control of arm movements. Exp Brain Res 42:223–227
Nasreddine Z, Phillips N, Bediriam V, Charbonneau S, Whitehead V, Collin I, Cummings J, Chertkow H (2005) The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 53(4):695–699
Oldfield RC (1971) The assessment and analysis of handedness: The Edinburgh Inventory. Neuropsychololgia 9:97–113
Park JJ, Tang Y, Lopez I, Ishiyama A (2001) Age-related change in the number of neurons in the human vestibular ganglion. J Comp Neurol 431(4):437–443
Pigeon P, Feldman AG (1998) Compensatory arm–trunk coordination in pointing movements is preserved in the absence of visual feedback. Brain Res 802:274–280
Pigeon P, Yahia LH, Mitnitski AB, Feldman AG (2000) Superposition of independent units of coordination during pointing movements involving the trunk with and without visual feedback. Exp Brain Res 131:336–349
Raptis H, Dannenbaum E, Paquet N, Feldman A (2007) Vestibular system may provide equivalent motor actions regardless of the number of body segments involved in the task. J Neurophysiol 97:4069–4078
Rosenthal U, Rubin W (1975) Degenerative changes in the human vestibular sensory epithelia. Acta Otolaryngologica (Stockh) 79:67–80
Rossi E, Mitnitski A, Feldman AG (2002) Sequential control signals determine arm and trunk contributions to hand transport during reaching in humans. J Physiol 538:659–671
Rothstein D, Larish D, Petruzzello S, Crew D, Nahom A (1989) Bimanual coordination in the healthy old. Gerontologist 29:258A–259A
Roy E, Elliott D (1989) Manual asymmetries in aimed movements. Q J Exp Psychol Sect A 41(3):501–516
Sainburg RL, Kalakanis D (2000) Differences in control of limb dynamics during dominant and non dominant arm reaching. J Neurophysiol 83(5):2661–2675
Salthouse TA (1985) Speed of behavior and its implications for cognition. In: Birren JE, Schaie KW (eds) Handboolc of the psychology of aging. Van Nostrand Reinhold, New York, pp 400–426
Schmidt RA (1975) A schema theory of discrete motor skill learning. Psychological Rev 82(4):225–260
Seidler-Dobrin RD, Stelmach GE (1998) Persistence in visual feedback control by the elderly. Exp Brain Res 119(4):467–474
Seidler RD, Alberts JL, Stelmach GE (2002) Changes in multi-joint performance with age. Mot Control 6(1):19–31
Sibindi TM, Krasovsky T, Feldman AG, Dannenbaum E, Zeitouni A, Levin MF (2013) Arm–trunk coordination as a measure of vestibulospinal efficiency. J Vestib Res 23:237–247
Stelmach GE, Worringham CJ (1985) Sensorimotor deficits related to postural stability: implications for falling in the elderly. Clin Geriatr Med 1(3):679–694
Stelmach GE, Goggin NL, Amrhein PC (1988) Aging and the restructuring of precued movements. Psychol Aging 3:151–157
Thornton M, Sveistrup H (2010) Intra- and inter-rater reliability and validity of the Ottawa Sitting Scale: a new tool to characterise sitting balance in acute care patients. Disabil Rehabil 32(19):1568–1575
Tunik E, Poizner H, Levin M, Adamovich SV, Messier J, Lamarre Y, Feldman A (2003) Arm–trunk coordination in the absence of proprioception. Exp Brain Res 153(3):343–355
Tunik E, Poizner H, Adamovich SV, Levin M, Feldman A (2004) Deficits in adaptive upper limb control in response to trunk perturbations in Parkinson’s disease. Exp Brain Res 159:23–32
Wallace JE, Krauter EE, Campbell BA (1980) Motor and reflexive behavior in the aging rat. J Gerontol 35:364–370
Welford AT (1977) Motor performance. In: Birren JE, Schai KW (eds) Handbook for the psychology of aging. Van Nostrand Reinhold, New York
Acknowledgements
(MFL and HS) Heart and Stroke Foundation Center for Stroke Recovery (HSFCSR PT-59562) Catalyst Grant. Elucidating the underlying mechanisms of disordered upper limb function in stroke: the relationship between deficits in trunk control and upper limb coordination. April 1, 2013-March 31, 2015. Thanks are extended to S.K. Subramanian for help with the experimental set-up and to all the participants in the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Khanafer, S., Sveistrup, H., Levin, M.F. et al. Age differences in arm–trunk coordination during trunk-assisted reaching. Exp Brain Res 237, 223–236 (2019). https://doi.org/10.1007/s00221-018-5412-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-018-5412-2