
Abstract
During trunk-assisted reaching to targets placed within arm’s length, the influence of trunk motion on the hand trajectory is compensated for by changes in the arm configuration. The role of proprioception in this compensation was investigated by analyzing the movements of 2 deafferented and 12 healthy subjects. Subjects reached to remembered targets (placed ~80° ipsilateral or ~45° contralateral to the sagittal midline) with an active forward movement of the trunk produced by hip flexion. In 40% of randomly selected trials, trunk motion was mechanically blocked. No visual feedback was provided during the experiment. The hand trajectory and velocity profiles of healthy subjects remained invariant whether or not the trunk was blocked. The invariance was achieved by changes in arm interjoint coordination that, for reaches toward the ipsilateral target, started as early as 50 ms after the perturbation. Both deafferented subjects exhibited considerable, though incomplete, compensation for the effects of the perturbation. Compensation was more successful for reaches to the ipsilateral target. Both deafferented subjects showed invariance between conditions (unobstructed or blocked trunk motion) in their hand paths to the ipsilateral target, and one did to the contralateral target. For the other deafferented subject, hand paths in the two types of trials began to deviate after about 50% into the movement, because of excessive elbow extension. In movements to the ipsilateral target, when deafferented subjects compensated successfully, the changes in arm joint angles were initiated as early as 50 ms after the trunk perturbation, similar to healthy subjects. Although the deafferented subjects showed less than ideal compensatory control, they compensated to a remarkably large extent given their complete loss of proprioception. The presence of partial compensation in the absence of vision and proprioception points to the likelihood that not only proprioception but also vestibulospinal pathways help mediate this compensation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Due to the redundant number of degrees of freedom (DFs) of the body, a given movement can be performed using different kinematic and kinetic patterns. Redundancy underlies an essential property of neuromuscular control—motor equivalency, or the ability to reach the motor goal using different body configurations and environmental means (Lashley 1951; Bernstein 1967). For example, the hand and finger kinematics in reaching and grasping the same object in space can vary depending on the need to avoid obstacles and the shape of the object to be grasped. Understanding how the nervous system selects movement patterns from the redundant set of DFs while preserving the efficiency of the motor action is fundamental for the understanding of the basic principles underlying motor control (Lashley 1951; Bernstein 1967; Latash et al. 2002).
It has been suggested that the nervous system may divide DFs into groups or functional synergies, each controlled by a small number of variables depending on the task demands (Bernstein 1967). For example, trunk-assisted reaching movements to targets within the reach of the arm are thought to be comprised of two synergies: an arm transport synergy, bringing the hand to the object, and a compensatory arm–trunk synergy, minimizing the influence of the trunk motion on the position of the hand through additional changes at the arm joints (Ma and Feldman 1995; Pigeon and Feldman 1998). The compensatory synergy is organized in a flexible way so that, in movements to targets placed beyond arm’s reach, the degree (“gain”) of the compensation is attenuated to allow the trunk to contribute to the movement extent (Rossi et al. 2002). Furthermore, in order for the goal to be accomplished in a coordinated and timely manner, the modulation of synergies must be rapid. Empirical data suggest that the nervous system is capable of such rapid responses, for example in maintaining speech production when the jaw movement is unexpectedly perturbed (Gracco and Abbs 1985) or in maintaining the hand trajectory during reaching movements when the trunk motion is mechanically blocked (Adamovich et al. 2001).
Data on the role of different sensory systems (visual, vestibular, and proprioceptive) in the organization of the compensatory arm–trunk synergy in reaching are limited. Pigeon and Feldman (1998) and Pigeon et al. (2000) have investigated the role of vision in compensatory arm–trunk coordination during reaching movements and found that subjects are able to compensate for the influence of the trunk motion on the hand trajectory in the absence of visual feedback (see also Adamovich et al. 2001). In the latter study, the authors also analyzed the kinematic responses to sudden arrests of the trunk motion in reaching movements to remembered targets. They found that the hand trajectory remained invariant whether the trunk motion was unobstructed or mechanically blocked. They conclude that proprioceptive and/or vestibular signals related to trunk motion, rather than vision or mechanical factors such as limb inertia play a major role in compensatory arm–trunk coordination during reaching.
The present study focuses on the role of the proprioceptive system in compensatory arm–trunk coordination during reaching movements. Proprioceptively deafferented and healthy, aged-matched individuals performed, in the absence of visual feedback, trunk-assisted reaching movements to remembered targets placed within arm’s reach. On 40% of randomly selected trials, their trunk motion was unexpectedly blocked. We assumed that if proprioceptive signals resulting from hip and spine flexion play a predominant role in coordinating arm and trunk movements, then deafferented subjects, unlike healthy subjects, would be unable to maintain the same hand trajectory in blocked-trunk trials as compared to free-trunk trials. The opposite result would suggest that the vestibular system participates in coordinating the compensatory synergy. Some results from this study have been reported in abstract form (Tunik et al. 2001).
Methods
Subjects
Two individuals, with complete loss of proprioception in the limbs and trunk caudal to the neck due to specific degeneration of the large myelinated sensory fibers, and 12 healthy individuals participated in the study after signing consent forms approved by the ethics committees of Rutgers University and the Rehabilitation Institute of Montreal.
One deafferented subject, G.L. (49 years old), is a right-handed woman and, after two polyneuropathy episodes before 1979, was unable to detect motion of the joints, vibration in all extremities and trunk, and discriminate two points or feel pressure on the skin. Neurological examination revealed intact pain and temperature sensation (small fibers) and strength (efferent), absent stretch and unloading reflexes (Levin et al. 1995), some minor tactile sensation (Olausson et al. 2002), bilaterally intact vestibular function (Dr. Peterka, Clinical Vestibular Laboratory, Good Samaritan Hospital and Medical Center, Portland, USA), and ability to do mirror drawing (Lajoie et al. 1992). For G.L.’s medical history, see http://deafferented.apinc.org/. The other deafferented subject, C.F. (72 years old), was a left-handed man. His illness started in 1989, leading to progressive sensory loss and ataxia over 1 week. Like G.L., he was unable to detect motion of the joints, discriminate two points on the skin, or sense vibration in all extremities and trunk. Strength, pain, and temperature sense was within normal limits. His vestibular function was not clinically tested. Further details of his medical status can be found in Sainburg et al. 1993. For reliability, G.L. was tested in our experiments three times within 2 years. The data of the first and the last test session are termed GL1 and GL2, respectively. C.F. was tested twice in 2000 (termed CF1 and CF2, respectively). GL2 and CF1 data will be shown graphically and the other data will be described in the text and table. Functionally, both were wheelchair bound; however, G.L. required less assistance to ambulate short distances and was less impaired in grasping movements. Their data were compared with those of 12 healthy individuals (67.3±6.9 years old).
Apparatus and procedures
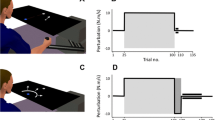
Subjects sat with their dominant arm resting on a tabletop and the index fingertip placed at the initial target located about 30 cm in front of the sternum (Fig. 1). A trial began with the illumination of a far target, cueing the subject to lift their entire arm several centimeters above its resting position. One second later, liquid-crystal glasses, worn by the subjects, became opaque, effectively blocking their vision, and an auditory signal cued the subject to initiate movement to the far target. Subjects were instructed to quickly move the fingertip to the remembered target location without making corrections or touching the table, stop briefly, and return their hand in a self-paced way to the initial position—at which time vision was restored and the arm was allowed to rest on the table until the next trial. Stopping was requested in order to minimize errors in the determination of the final, static hand position in each trial. Touching the table was not allowed to exclude an uncontrollable mechanical factor (the interaction of the hand with the table) influencing the movement. This also deprived the deafferented subjects of using some residual tactile sensitivity in the hand (see above) to identify the end of movement.

Experimental set-up. Targets (T1 and T2) were embedded in the ipsi- and contralateral tabletop workspace. Arm movements to T1 or T2 were performed above the table, with simultaneous sagittal trunk bending. In a pseudorandom fashion (in 40% of the trials), the trunk motion was unexpectedly blocked by the electromagnet
Subjects were required to produce reaching movements simultaneously with an active and robust forward trunk motion. They wore a harness with an electromagnetic plate attached to the back. Before each trial the plate was locked to an electromagnet (Warner Electric) fixed to the wall behind the subject (Fig. 1). On 60% of randomly selected trials, unrestrained trunk motion was allowed by deactivating the electromagnet at the time of the auditory signal (free condition). For the remaining 40% of the trials, trunk motion was unexpectedly blocked (blocked condition) by keeping the electromagnet activated during the trial. The perturbation did not cause any pain to the subjects. Training was conducted using only the free-trunk condition and no knowledge of results was given during the experiment.
One far target (T1) was placed in the workspace of the dominant arm, at a distance of 30 cm from the initial target, and oriented 80° relative to the sagittal axis. The other target (T2) was placed in the workspace of the nondominant arm (15 cm distance at an angle of 45°). The use of these two targets was intended to maximize movement errors in those trials in which the trunk was arrested. In particular, for movements to T1, the trunk moved in the sagittal direction almost orthogonal to the hand movement. If not corrected by appropriate modifications in the arm joint angles, the effect of the trunk arrest on hand motion would be maximal in terms of direction. A similar combination of the trunk and hand movement directions in the contralateral workspace would have been restricted biomechanically. Due to these constraints, the contralateral target was shifted toward the sagittal axis.
Arm–trunk kinematics were derived from position data obtained by an optoelectronic 3-camera system (Optotrak, Northern Digital; sampling rate 200 Hz) localizing six infrared-emitting diodes (IRED) attached to bony landmarks of the sternum, acromion processes of both shoulders, lateral epicondyle of the elbow, wrist styloid, and index fingertip. IRED data were low-pass filtered at 12 Hz and analyzed offline using customized LabView (National Instruments) and MatLab software.
Trials were excluded from analysis if: (a) missing markers prevented the analysis of that trial, or (b) there was an aberrant motion of the hand or trunk not consistent with the requirements of the task (e.g., an impoverished sagittal or excess lateral trunk motion that fell outside 2 SD from the mean excursion for the same condition for that subject). Between 90 and 110 trials were collected per healthy subject. Of the total 1,217 trials collected for all healthy subjects, 8% were excluded due to criterion a and 2% due to criterion b. No difference was found in the proportion of excluded trials between the free and blocked conditions (t=0.606, P=0.5476). No difference was found between the proportion of excluded trials that comprised the first three movements and the last three movements (t=0.492, P=0.625). Because deafferented subjects were tested more than once, the cumulative number of trials for G.L. or C.F. is greater than for a given healthy subject. Each testing session for each deafferented subject was analyzed independently rather than being pooled. In G.L.’s case, of the 241 trials, 11 trials were excluded, and 10 of these were due to criterion a. Two of eleven excluded trials occurred in the first three movements of a block and 1 occurred in the last three movements. For C.F., of the 144 trials, 5 were excluded and, of these, 3 were due to criterion a. One trial occurred in the last three movements while none occurred in the first three movements of either blocked or free conditions. Thus, trial exclusion did not introduce any bias into the data analysis.
Kinematic measures
Movement time (MT) was defined as the time between the points at which the hand tangential velocity first exceeded and then fell below 5% of the peak velocity. Each hand path was then spatially normalized and divided into four segments situated between the points representing 0, 25, 50, 75, and 100% of the normalized hand trajectory. To characterize the changes in the direction of the hand trajectory during the movement, the points demarcating each segment were connected by a line and a deviation angle between each pair of lines associated with adjacent segments was computed (three angles for each trajectory). To characterize the final direction of the hand trajectory in the external workspace, we computed the angle between the line of the last (4th) segment and the x-axis, orientation angle. To estimate whether or not the trunk perturbation influenced the hand trajectory, the four angles were compared between the two conditions.
Similarly, invariance in tangential hand velocity profiles was tested by dividing them into 4 equal segments in normalized time, computing the velocity at each of the 3 points of transition from one segment to the next, and comparing these values across conditions.
We also compared: 2D error, the absolute distance the between the final hand position and the target in the horizontal plane; azimuth error, the angle between the vectors connecting the initial position with the target and the initial hand position with the final hand position in the horizontal plane; radial error, the difference in length between the vectors connecting the initial and final hand positions and the initial position with the target; sagittal error, the difference in length between the final hand position and the target along the sagittal axis; peak velocity, the maximum hand velocity; and time to peak velocity, time elapsed between movement onset and the attainment of peak hand velocity.
We assumed that invariance of the hand trajectories could only be achieved by condition-dependent changes in elbow and shoulder coordination. To quantify this capacity, elbow flexion/extension was measured as the angle between the line connecting the wrist and elbow markers and that connecting the shoulder and elbow markers. Horizontal shoulder abduction/adduction was measured as the angle between the line connecting the left and right shoulder markers and that connecting the shoulder and elbow markers of the moving arm. Angle profiles were also used in identifying the latency of the compensatory response. For this, perturbation onset was defined as the time at which the deviation in the mean trunk velocity exceeded and remained outside 1 SD of that in the blocked condition. The latency of the compensatory response, therefore, was the time interval between the onset of the perturbation and the time at which the mean distance between the free and blocked angle–angle curves exceeded 1SD of those in the free condition.
Statistics
Between-conditions comparisons of measured variables were used to estimate a subject’s ability to compensate for the perturbation. Specifically, no difference in hand trajectories between conditions would suggest that the subject successfully compensated for the perturbation. In contrast, significant differences in trajectories between conditions would reflect lack of compensation. In addition, between-groups comparisons were used to determine general motor-control deficits related to deafferentation, irrespective of compensatory abilities. Thus, if a deafferented subject differed from control subjects on both free-trunk and blocked-trunk trials, then the deficit would be related to general motor-control impairments rather than specifically reflecting impairments in compensating for the perturbation.
For between-conditions analysis of the 12 healthy subjects, a two-way repeated measures analysis of variance (ANOVA) with condition (free- and blocked-trunk) and target (ipsi- and contralateral) as factors was performed. Each deafferented subject’s data were analyzed as a separate data set, consistent with other, similar multicase designs (Sainburg et al. 1993; Ghez et al. 1995; Lajoie et al. 1996). A nonparametric, Mann-Whitney U-test, was chosen for the within deafferented-subject analysis, since this test could be applied not only to normal but also to other types of distributions and could be used in cases of smaller sample sizes. The change in the performance on a particular measure, depending on the condition, was considered significant if P<0.05. To reduce the probability for type I error in cases of repeated measurements, the significance level (0.05) was divided by the number of measures (4 angles for the hand trajectory and 3 values for the velocity curve). Thus, the corrected values of significance levels were 0.0125 and 0.016, respectively.
For between-group analysis, the angle characterizing the hand trajectory for each blocked-condition trial was subtracted from the respective mean angle in the free condition. A t-test was then used to compare each deafferented subject with the control group at the corrected significance level. To test whether the performance of the deafferented subjects was more variable than healthy subjects, we performed a one-group (one-sample) t-test on the coefficient of variation (SD/mean) between each deafferented subject and the control group.
Although subjects did not have knowledge of results during the experiment, we analyzed whether each subject’s performance changed across trials, which might indicate that they adapted to the perturbation. For this, the difference between free- and blocked-condition deviation measures was compared for the first three and the last three trials. For healthy subjects, a two-way repeated-measures ANOVA (target × trial position) was performed and, for each deafferented subject, a Student’s t-test was used.
Results
Healthy subjects
Ipsi- and contralateral targets
Typical hand and trunk kinematics of reaches toward T1 and T2 are shown for one healthy subject (J.D.) in Fig. 2. The sagittal trunk displacement was reduced from 19.3 cm in the free condition to 4.2 cm in the blocked condition (Fig. 2B, F; group mean, across targets). The residual trunk motion in perturbed trials occurred due to the compression of the soft tissues by the harness. Despite the reduction in the trunk movement, the difference in sagittal hand displacement between conditions was small (group mean, across targets 3.7 cm), though significant (F 1, 11=103.0, P=0.0001). A significant condition-target interaction was present (F 1, 11=8.33, P=0.0148). Post hoc analysis revealed that this was attributed to significant between-condition differences for movements to T2 (t=−4.1, P=0.0005) but not to T1 (t=−0.835, P=0.4126). 2D and radial errors did not differ significantly between conditions (F 1, 11=4.801, P=0.0509, and F 1, 11=2.838, P=0.0991, respectively; Table 1). Again a significant condition-target interaction was present (F 1, 11=6.385, P=0.0281). Post hoc testing revealed that this was attributed to significant between-condition differences for movements to T2 (t=−2.416, P=0.024) but not to T1 (t=−0.324, P=0.7488).

A representative control subject’s (JD) arm–trunk kinematics for movements to T1 (A–D) and T2 (E–H). Hand and trunk trajectories (top row) and tangential velocities (bottom row) for all trials and their respective means ±1 SD in the free (gray lines) and blocked condition (black lines). The difference between the free- and blocked-condition hand trajectories at angles 1–4 are shown in the inset B and F. The difference between hand velocity values at 25%, 50%, and 75% of movement time are shown in the inset of D and H. Whiskers represent ±1 SD. Triangles mark initial and final target locations. The time scale between circles in B and F is 50 ms
Figure 2 (top row) shows that hand trajectories remained largely invariant with discrepancies between the free and blocked conditions occurring at the end of movements. Insets in these panels show that the deviation angles 1–3 characterizing the incremental changes in the direction of hand trajectories did not exceed 10°. The condition-dependent changes in these angles were not significant (e.g., for angle 3, F 1, 11=2.840, P=0.1201). The final direction of the hand trajectory with respect to the x–axis (see Methods) did not differ between conditions (F 1, 11=6.451, P=0.0275).
Despite marked reductions in both the extent and velocity of the trunk motion (Fig. 2D, H; lower traces), the perturbation had no effect on the hand velocity profiles (calculated at three instants of movements; see Methods; e.g., for values at 75% of the movement time, F 1, 11=0.048, P=0.8309). The same was true for the movement time (0.84 and 0.86 s; F 1, 11=0.595, P=0.4568) and the normalized time to peak velocity (39% and 37%; F 1, 11=0.595, P=0.4568). Thus, healthy subjects successfully preserved the spatial and temporal aspects of the hand movement, despite the effects of the perturbation on the trunk motion.
Deafferented subject G.L.
Ipsilateral target
During trunk-assisted reaches toward T1, G.L.’s sagittal trunk motion was reduced by a mean 11.8 cm due to the perturbation (Fig. 3B). Despite this, the mean condition-dependent change in the hand movement displacement in the sagittal direction was only 1.5 cm. The condition-dependent changes in the direction of the hand path measured at its 4 points (see Methods) did not exceed 5° and were nonsignificant (e.g., for the final direction of the hand trajectory, U=445, P=0.8017). Analysis of the radial error showed that the length of G.L.’s hand path in the blocked condition was significantly greater than in the free condition (e.g., by 6 cm in GL1, U=229; P=0.034), a pattern opposite to that of healthy subjects (Table 1). Overall, the perturbation resulted in a substantial decrease in the peak trunk velocity (Fig. 3D), from 0.33 to 0.09 m/s. The hand velocity also decreased, but this was only significant at 25% of the normalized hand movement time (for this point, velocity decreased from 1.08 to 0.83 m/s). Such findings are suggestive of incomplete compensation and are complementary with those of spatial kinematics, where certain measures (e.g., radial error) were also found to be significantly different between conditions, while the changes in the hand trajectory were not at any of the 4 points of measurement.

Deafferented subject’s (GL) arm and trunk kinematics for movements to T1 (A–D) and T2 (E–H). Hand and trunk trajectories (top row) and tangential velocities (bottom row) for all trials and their respective means ±1 SD in the free (gray lines) and blocked condition (black lines). The difference between the free- and blocked-condition hand trajectories at angles 1–4 are shown in the inset B and F. The difference between hand velocity values at 25%, 50%, and 75% of movement time are shown in the inset D and H. Whiskers represent ±1SD. Triangles mark initial and final target locations. The time scale between circles in panels B and F is 50 ms
Contralateral target
When G.L. reached toward T2 (Fig. 3E–H), her sagittal trunk motion was reduced by a mean 9.6 cm due to the perturbation, with very little change in the sagittal hand displacement between conditions (0.6 cm; U=327; P=0.2098). The condition-dependent changes in the direction of the hand path (deviation angles) did not exceed 10° for the first two angles and then rose to 20° for the 3rd angle. The final direction of the hand trajectory (orientation angle) changed by 22°. However, all these changes in the hand trajectory were not significant between free and blocked conditions (e.g., for the change in the orientation angle, U=400, P=0.9126). In general, the final part of the hand trajectory was characterized by very variable, hook-like deviations, possibly associated with deficits in stabilization of the final hand position (drift) and/or in interjoint coordination, a phenomenon noticed in other studies of movements in deafferented subjects (Sainburg et al. 1993, 1995). The perturbation, in addition to reducing trunk displacement, also reduced the magnitude of the trunk velocity, from 0.35 m/s in the free condition to 0.12 m/s in the blocked condition. Thereby, the hand velocity was also significantly reduced, but only at 50% of the normalized movement time (U=176; P=0.0003).
Like healthy subjects, G.L. managed, to a certain degree, to preserve the spatial path despite the trunk perturbation. On the other hand, radial overshoots in the blocked condition for movements toward T1, end-of-movement deviations for movements toward T2, and transient differences in hand-velocity values suggest that the trunk perturbation had some influence on G.L.’s arm kinematics, implying that compensation for the influence of trunk motion on the hand trajectory was incomplete in this subject.
Deafferented subject C.F.
Ipsilateral target
Because deafferented subject C.F. was left-handed, T1 was positioned in his left workspace (Fig. 4A–D). Like in other subjects, the perturbation markedly reduced his sagittal trunk motion (mean 15.2 cm). Despite this, the mean condition-dependent change in the hand movement displacement along the sagittal direction was less than 0.5 cm (Table 1; U=257, P=0.7012). The inset in Fig. 4B further shows that condition-dependent differences in the trajectory deviation angles did not exceed 8° and were nonsignificant at all four angles. The observation that C.F. preserved the direction of the hand path in free and blocked conditions suggests that he was able to compensate for the effect of the trunk arrest on the hand path. This compensation, however, was only partial, similar to G.L. For example, the radial distance of hand paths in the blocked condition was systematically and significantly greater than in the free condition (mean 8.7 cm; U=76, P<0.0001 for CF1; see Table 1).

Deafferented subject’s (C.F.) arm and trunk kinematics for movements to T1 (A–D) and T2 (E–H). Hand and trunk trajectories (top row) and tangential velocities (bottom row) for all trials and their respective means ±1SD in the free (gray lines) and blocked condition (black lines). The difference between the free and blocked-condition hand trajectories at angles 1–4 are shown in the inset B and F. The difference between hand velocity values at 25%, 50%, and 75% of movement time are shown in the inset D and H. Whiskers represent ± 1SD. Triangles mark initial and final target locations. The time scale between circles in B and F is 50 ms
The perturbation caused a marked reduction in the peak trunk velocity (Fig. 4D, lower traces), from 0.34 to 0.11 m/s. Hand kinematics were also affected by the perturbation; e.g., MT increased significantly (by ~146 ms) and the time to peak hand velocity was reached significantly later (by 8%) in the blocked condition. Further, both MT and the time to peak hand velocity of both conditions were greater than those of the healthy subjects and of G.L. Changes in the hand velocity were nonsignificant at each of the three points of measurement, although such changes could not be estimated in a reliable way because of the marked variability of the hand velocities (Fig. 4C), which significantly exceeded that of healthy subjects. Such deficits in the temporal characteristics of C.F.’s movements were complemented by the presence of multiple velocity peaks and irregular velocity shape in both conditions (Fig. 4C).
Contralateral target
The perturbation reduced the sagittal trunk displacement and velocity by 17.9 cm and 0.33 m/s, respectively. In contrast, nearly 50% of the hand trajectory remained similar; e.g., the condition-dependent change in the 1st deviation angle did not exceed 12° and was not significant (Fig. 4F). The hand path of the blocked condition began to deviate from that of the free condition at about 750 ms after movement onset, and the mean condition-dependent change in the 2nd deviation angle was 25°; t=3.582, P=0.0014). At the end of movement, the azimuth difference between the hand trajectories was substantial (Table 1, 37.8°; U=0, P=0.0034). The perturbation also led to a reduction in the peak hand velocity (by 0.31 m/s, U=1; P=0.0054) and an increase in the time to peak hand velocity (Fig. 4H; by 21%; U=5, P=0.0281).
Analysis of adaptation
To determine whether subjects adapted to the perturbation across trials, each subject’s first and last three trials were compared with one another. In healthy subjects no significant main effect was found in angles 1–4 between the first three and last three trials of the experiment (e.g., for angle 1: F 1, 11=0.239, P=0.6348). Similarly, no difference between early and late trials was found in deafferented subject G.L. or C.F. for any of the 4 angles (e.g., movements to T1 for G.L. and C.F. at angle 1, respectively: t=−1.337, P=0.3129; t=0.132, P=0.9070). These results suggest that adaptation to the perturbation did not occur in any of the subjects.
Between-group differences
The 4 angles for the hand trajectory in the free and blocked conditions for C.F. were compared with those of the healthy subjects (see Methods). For movements to T1, angle 1 for C.F. at the first testing session differed from that of healthy subjects (t=−33.963, P<0.0001), with no further differences at other angles in either session. For movements to T2, between-group differences were noted at each angle, in both sessions. The coefficient of variation (CV) was significant at the 1st deviation angle in both testing sessions and in both free and blocked conditions (e.g., for CF2 toward T2: blocked, t=3.908, P=0.0024; free, t=10.317, P<0.0001). His hand velocities were also more variable than in healthy subjects (e.g., CV for CF2 toward T2 at 25% movement time: blocked, t=−8.008, P<0.0001; free, t=−38.29, P<0.0001).
The findings were similar for G.L. For movements to T1, only angle 2 in her second testing session was significantly different from that of healthy subjects (t=−4.024, P=0.002), while other angles in either session were not. For movements to T2, between-group differences were significant at all four angles in her first session, but only angle 4 was different from healthy subjects in her second session. Hand trajectories in GL1 were more variable than those of healthy subjects predominantly at the 1st deviation angle (e.g., CV toward T2: blocked, t=−5.525, P=0.0002; free, t=−17.313, P<0.0001), while in GL2 such effects were predominant at the 4th angle. Her hand velocities were more variable in both free and blocked conditions predominantly at 50% of movement time (e.g., CV in GL2 toward T2: blocked, t=−4.924, P=0.0005; free, t=−8.597, P<0.0001).
Joint kinematics
Healthy subjects
To prevent deviations in the hand paths resulting from the perturbation, subjects had to make compensatory changes in the elbow and shoulder angles. Such changes were observed in healthy subjects (Fig. 5 top panels). Compared with motion to T2, the almost orthogonal orientation between the hand paths to T1 and the sagittal trunk movements required more substantial changes in joint angles to maintain the hand trajectory despite the trunk arrest. As a consequence, the divergence of shoulder–elbow profiles in the two conditions was more distinctive for movements to T1 (compare top panels in Fig. 5). Because of this, measurements of the latency of angular deviations were more reliable for movements to T1 than T2. Compensatory changes in the elbow and shoulder angles were initiated within 50 ms in 8 of 12 healthy subjects when reaching to the ipsilateral target (group range, 40–150 ms).

Elbow–shoulder joint kinematics of a control subject (top panels), deafferented subject G.L. (middle panels), and C.F. (lower panels). Angle–angle kinematics for T1 are shown in the left column and for T2 in the right column. Gray lines and black lines represent the means (±1 SD) of the free and blocked conditions, respectively. x–y axes represent horizontal shoulder abduction–adduction and elbow extension (degrees), respectively. All joint angles are measured as changes from the initial joint values. The first and second open circles (arrows) in the left column represent the time at which the trunk velocities diverge and the time at which the elbow–shoulder profiles diverge, respectively. The open marker (arrow) in the bottom right panel depicts the time (800 ms) at which C.F.’s hand path of the blocked condition diverges from the free condition when reaching to T2 (see Fig. 4F). Time scale between circles, 50 ms
Deafferented subjects
Following the perturbation, changes in the trunk kinematics in G.L., as in healthy subjects, became evident 30 ms after the onset of trunk motion (Fig. 3D, and first open circle in left middle panel). As in healthy subjects, the condition-dependent divergence in G.L.’s shoulder–elbow angle profiles started within 50 ms after that (Fig. 5 left middle panel, second open circle) leading to the preservation of the hand path (Fig. 3B). In addition to the latency of the compensatory response, the qualitative changes in the shoulder–elbow profiles were similar to those of the healthy subjects for both conditions (compare Fig. 5 left top and middle panels).
In movements to the ipsilateral target, C.F. (like G.L.) initiated compensatory changes in joint angles within 50 ms after the perturbation. In movements to T2, C.F.’s joint coordination in the blocked condition changed from one in which there was a proportional excursion of the elbow and shoulder during the first half of the movement to one of almost exclusive elbow extension (Fig. 5 bottom right panel). The transition (open circle) occurred at about the time when the hand trajectories in the two conditions began to diverge (at about 750 ms; Fig. 4F). Thus C.F. was unable to maintain an adequate compensation beyond this time. In addition, whereas healthy subjects and G.L. extended the elbow by ~40° in the blocked condition for reaches to T2, C.F. extended the elbow almost twice that amount.
Discussion
Basic findings
We investigated trunk-assisted reaching movements in deafferented and aged-matched healthy subjects. In healthy subjects, the hand trajectory and velocity profiles remained invariant when the active trunk flexion was unexpectedly blocked. In movements toward target T1, the invariance was achieved by substantial changes in the elbow and shoulder angles initiated at latencies of 50 ms or less in 8 of the 12 healthy subjects. These findings resemble those previously reported for younger, healthy subjects (Adamovich et al. 2001).
The focus of the present study was to analyze between-condition kinematics, which allowed us to infer whether the trunk perturbation was compensated for at the hand. Additionally, however, we analyzed between-group differences, which, when present in both free and blocked conditions, are suggestive of general motor control deficits, not necessarily related to the subjects’ ability to compensate for the perturbation. Deafferented subjects had more variable spatial and temporal kinematic measures than healthy subjects in both conditions. This finding supports and complements previous literature describing the general motor control deficits related to proprioceptive loss (Sainburg et al. 1993, 1995). Although C.F. was clearly more impaired than G.L., both deafferented subjects showed the presence of terminal hook-like deviations in movements to T2 in both the free and blocked conditions. Such deficits, predominantly in the terminal phase of the movement paired with findings of increased between-group variability likely arise as a consequence of proprioceptive loss. Additionally, certain kinematic measures differed between conditions. For example, both deafferented subjects showed significantly different radial errors to T1 between the blocked and free conditions (typically greater hand movement extents in the blocked condition) and both showed significantly larger azimuth errors to T2 in the blocked than in the free condition. Such between-condition differences suggest that the trunk perturbation was not fully compensated for at the hand. However, a major result of this study is that despite these motor deficits, both subjects also showed important elements of compensation. For example, hand deviations and velocities remained relatively invariant between free and blocked conditions in G.L. and, in the case of trajectories to T1, for C.F. Although C.F. was unable to provide adequate compensation after 750 ms into the movement to T2, the hand paths in the early portion of that movement (e.g., closer to the time of trunk perturbation) showed invariance between conditions. Interjoint coordination data suggests that deafferented subjects were able to substantially diminish the influence of the unexpected trunk perturbation on the hand trajectory and, importantly, for movements toward T1, initiate compensatory changes in the arm joint angles at latencies as early as 50 ms after the trunk perturbation, i.e., at latencies comparable to those of healthy subjects.
Compensatory arm–trunk coordination in healthy and deafferented subjects
Ghafouri et al. (2002) showed that trunk-assisted pointing movements to motionless targets are produced in an allocentric frame of reference, while movements to targets moving with the trunk are produced in an egocentric frame of reference. Thereby, compensatory changes in the arm joint angles were observed in the former but not in the latter case though hand trajectories remained invariant in both cases, but in the respective frames of reference. In addition, when reaching to targets placed beyond arm’s length, the degree (gain) of the compensatory arm–trunk coordination was attenuated to allow the trunk to contribute to the hand movement extent (Rossi et al. 2002). These findings suggest that the nervous system can introduce, grade, or exclude compensatory arm–trunk coordination depending on task demands. These findings also imply that, in healthy subjects, mechanical factors, like arm inertia and/or joint-interaction torques, may not be fully responsible for compensation. Rather, these factors might be responsible for small differences in the hand trajectory and velocity profiles of free and blocked conditions, mainly noticeable at the terminal phase of the hand movement. In addition, these mechanical factors are acceleration- and velocity- dependent and cannot predetermine the final arm–trunk configuration (Adamovich et al. 2001). The finding of a substantial difference in the final arm–trunk configuration between the two conditions in the previous and in the present study thus implies that reflex and/or intentional control processes, rather than passive mechanical factors, were responsible for the condition-dependent transition from one configuration to the other.
Indeed, the arm inertia and interactive torques may influence the dynamics of the transition from the initial to a final posture. Therefore, successful reaching movements necessitate minimization of their influence on the hand. Healthy subjects can achieve this without specific learning under natural movement conditions or after some period of learning if arm movements are complicated by mechanical perturbations (Gribble and Ostry 1998, 1999; Sainburg et al. 1999). Incorporating a trunk movement into a reach does not reduce the ability of the system to minimize the influence of inertia and interactive torques on the hand trajectory (Ma and Feldman 1995). The performance of the healthy subjects in the present study extends this capacity to the situation when the trunk motion is obstructed. Note, however, that if the joint kinematics remained the same, an appropriate increase in arm muscle stiffness and damping might be sufficient to preserve the shape but not the direction of the hand trajectory in the blocked condition (see Ghafouri et al. 2001). The condition-dependent changes in the arm joint angles observed in the previous and present study were thus necessary to prevent changes in hand movement direction.
It has been suggested that proprioceptive and vestibular signals, rather than independent central commands, are responsible for compensatory changes during trunk-assisted reaching (Pigeon and Feldman 1998; Adamovich et al. 2001). The latencies of compensatory reactions at the joint level measured in our healthy subjects (70 ±33 ms) are consistent with the idea of afferent-based compensation. In our study, subjects made movements in the absence of vision but the possibility remains that compensation in healthy subjects is based on the proprioceptive and/or vestibular signals related to the head and trunk motion and transmitted to motoneurons of arm muscles. Our analysis of compensation in proprioceptively deafferented subjects with virtually intact, though possibly more sensitive vestibular systems (see below) is a first step in addressing this issue.
Compared with healthy subjects, multijoint movements of deafferented individuals are impaired in several respects (Sainburg et al. 1993, 1995; Nougier et al. 1996). For example, Sainburg et al. (1995) investigated how well deafferented individuals performed reaches to targets resembling our ipsi- and contralateral targets. Movements to the contralateral target that required a higher degree of coordination of shoulder and elbow motions were substantially impaired. Such empirical data supports the role of proprioception in the control of multijoint movements. The lack of compensation for joint interaction torques that, in healthy subjects, is likely mediated by intermuscular proprioceptive influences might therefore be responsible for the deteriorated movements of deafferented subjects.
In our study, the reaching task was complicated by the active involvement of the trunk and a concomitant perturbation. Like in the study by Sainburg et al. (1995), deficits in the performance of deafferented patients, such as terminal hook-like deviations in the hand trajectory (most prominent in C.F. but absent in healthy subjects) were especially obvious for movements to the contralateral target. Making reaches to the ipsilateral target, deafferented subjects systematically increased the movement extent in trials in which the trunk motion was blocked whereas healthy subjects tended to do the opposite or maintained the same extent. Another deficit associated with deafferentation is a substantial increase in the variability of movements, as observed not only in the present but also in other studies (Ghez et al. 1995; Gordon et al. 1995). Taken together, the deficits imply a multifaceted role of proprioceptive reflexes in posture and movement regulation, possibly including the assistance in braking the arm motion (Cooke et al. 1985; Forget and Lamarre 1987).
Thus, our results showed that the required compensatory responses to mechanical perturbations during trunk-assisted reaching were deficient on some kinematic measures in the deafferented subjects. Comparisons between the healthy and deafferented subjects allow inferences into the role of proprioception in motor coordination. In order to make inferences about the deficits related to compensating for the perturbation, we performed detailed analyses between conditions, for each subject. The presence of spatial (G.L. and C.F.) and temporal (G.L.) invariance in the hand kinematics, particularly during the early portion of the movement, implies that proprioceptive feedback is not solely responsible for the compensatory arm–trunk synergy in deafferented individuals.
Possible mechanisms of arm–trunk compensation in the absence of proprioception
Since the compensation was only partially impaired in deafferented subjects, other afferent systems might be responsible for coordinating the compensatory arm–trunk synergy. Vision was blocked in the present experiment but a role of vestibular signals related to the head and trunk motion cannot be ruled out.
The vestibular system may influence posture and movement via vestibulospinal and vestibulo-reticulo-spinal projections to alpha- and gamma-motoneurons, propriospinal neurons, and interneurons (Wilson and Maeda 1974; Wilson et al. 1999; Li et al. 2001). Vestibular stimulation (galvanic, auditory, and/or head taps) elicits relatively short latency electromyographic responses in leg (~34–70 ms) and arm and neck (~20–41 ms) muscles (Botzel et al. 2001; Watson and Colebatch 1998a, 1998b; Horak et al. 1994; Baldissera et al. 1990; Britton et al. 1993). The latencies of electromyographic responses are usually smaller (by about 20 ms) than those measured from kinematic responses and thus consistent with latencies of compensatory responses in the present study in healthy and deafferented subjects.
The vestibular system likely exerts a coordinated influence over multiple muscles of a limb (synergies) as suggested by the observation that galvanic vestibular stimulation can alter the direction of arm reaching movements (Bresciani et al. 2002; Mars et al. 2003). Further, the effects of artificial vestibular stimulation can be noted in more distributed networks as implied by the observation of perceptual shifts in body posture and movement (Karnath et al. 1994; Inglis et al. 1995; Lobel et al. 1998). Lastly, descending vestibular influences have been shown to reset the threshold of the stretch reflex of extensor muscles (Feldman and Orlovsky 1972). This implies a hierarchical, rather than parallel organization of descending influences of the two afferent systems on motoneurons. Such organization is consistent with the suggestion that the loss of either system can result in ataxic postural responses, though via different mechanisms (Inglis and Macpherson 1995; Stapley et al. 2002). These interactions suggest that not only can different sensory channels influence the same motor function, but that a given channel can become more sensitive when deprived of input from other channel(s) (Horak et al. 1996; Horak and Hlavacka 2001; Welgampola and Colebatch 2001). This suggestion is supported by empirical observations that under no-vision conditions, a deafferented subject’s postural response to galvanic vestibular stimulation was an order of magnitude greater than that of a healthy individual (Day and Cole 2002). Plastic changes following chronic deprivation of somatosensory systems in deafferented subjects is indeed known to occur at different central (cortical and subcortical) levels (Weeks et al. 1999).
Consider our results by taking into account the plasticity of the nervous system in adapting to new conditions. One possibility might be that in healthy subjects, the proprioceptive system is predominantly responsible for the condition-dependent compensatory changes in the arm joint angles. Then, following deafferentation, the vestibular system might replace the proprioceptive system in this function. Another possibility is that the proprioceptive and vestibular systems cooperate in modulating the compensatory changes in joint angles and, after deafferentation, the latter system becomes predominant in the modulatory role. Plastic changes in the nervous system are implied by either of the hypotheses. Indeed, plasticity of the descending vestibular projections to the motoneurons of arm muscles, and cortical and subcortical reorganization, especially in regions involved in visual processing, may occur after deafferentation and progress over time. These changes may allow G.L. and C.F. to effectively use vision for movement precision (even in simple, single-joint tasks) and postural stabilization (Ghez et al. 1995; Levin et al. 1995). In the present task, however, deafferented subjects were capable, without vision, without previous experience of trunk-assisted reaching under unexpected perturbation conditions (subjects were trained only on free-trunk trials), and practically without learning, to make satisfactory compensatory changes in joint angles to largely preserve the hand trajectory in the first experimental session. Our results, that G.L. and, to a lesser degree C.F., partially compensated, combined with other literature demonstrating the presence of vestibular influence on arm–trunk movements, suggest that the vestibular and proprioceptive systems, at the very least, share their responsibility for control of the compensatory arm–trunk synergy in healthy subjects. Following deafferentation, this role of the vestibular system may have been preserved and possibly strengthened due to plasticity-induced sensitization.
In conclusion, our results suggest that 1) proprioceptive deafferentation leads to motor deficits in arm–trunk coordination. Compared with control subjects in both free and blocked, conditions, each deafferented subject was impaired on some (albeit not all) of the spatial and temporal compensatory measures and each showed greater variability than controls in both conditions. 2) In conditions of chronic deafferentation, human subjects can partially compensate for unexpected changes in trunk displacements, though their performance may depend on the biomechanical constraints of the task associated with reaching the ipsilateral and contralateral targets. Given that proprioceptive and visual inputs were not available to the patients in our experiment, our findings suggest that the vestibular system can play an important role in the compensatory synergy. This hypothesis should be verified more directly by testing individuals with vestibular pathology. It may also be addressed by studying arm–trunk coordination in deafferented individuals after caloric or galvanic vestibular stimulation. 3) Finally, most of the healthy and both of the deafferented subjects showed compensatory changes in joint kinematics (for movements to T1) as early as 50 ms after the onset of the perturbation. This finding suggests that the compensatory synergy can be modulated at relatively low levels in the neuraxis thereby avoiding the longer delays inherent in cortical loops.
Our data also partially support the hypothesis that some basic rules governing arm–trunk coordination during reaching resemble those guiding the eye-head coordination during fixation or shifts in gaze (Pigeon and Feldman 1998). Despite essential biomechanical differences between the two systems, the resemblance in the basic rules might be seen, in particular, in that the eye-head coordination also has two functionally distinct components—the saccade (corresponding to arm transport) and the vestibulo-ocular reflex (corresponding to the compensatory arm–trunk synergy). A gain control exists in both systems (Guitton 1992; Johnston and Sharpe 1994; Rossi et al. 2002). The resemblance between the two systems would be stronger if it appeared that vestibular signals were responsible for the coordination in both systems.
References
Adamovich SV, Archambault PS, Ghafouri M et al. (2001) Hand trajectory invariance in reaching movements. Exp Brain Res 138:288–303
Baldissera F, Cavallari P, Tassone G (1990) Effects of transmastoid electrical stimulation on the triceps brachii EMG in man. Neuroreport 1(3–4):191–193
Bernstein NA (1967) The coordination and regulation of movements. Pergamon, Oxford
Botzel K, Feise P, Kolev O, Krafczyk S, Brandt T (2001) Postural reflexes evoked by tapping forehead and chest. Exp Brain Res 138:446–451
Bresciani JP, Blouin J, Popov K et al. (2002) Galvanic vestibular stimulation in humans produces online arm movement deviations when reaching toward memorized visual targets. Neurosci Lett 318(1):34–38
Britton TC, Day BL, Brown P et al. (1993) Postural electromyographic responses in the arm and leg following galvanic vestibular stimulation in man. Exp Brain Res 94(1):143–151
Cooke JD, Brown S, Forget R, Lamarre Y (1985) Initial agonist burst duration changes with movement amplitude in a deafferented patient. Exp Brain Res 60:184–187
Day BL, Cole JC (2002) Vestibular-evoked postural responses in the absence of somatosensory information. Brain 125:2081–2088
Feldman AG, Orlovsky GN (1972) The influence of different descending systems on the tonic stretch reflex in the cat. Exp Neurol 37:481–494
Forget R, Lamarre Y (1987) Rapid elbow flexion in the absence of proprioceptive and cutaneous feedback. Hum Neurobiol 6:27–37
Ghafouri M, Archambault PS, Adamovich SV, Feldman AG (2002) Pointing movements may be produced in different frames of reference depending on the task demand. Brain Res 929(1):117–128
Ghez C, Gordon J, Ghilardi MF (1995) Impairments of reaching movements in patients without proprioception. II. Effects of visual information of accuracy. J Neurophysiol 73:1;361–372
Gordon J, Ghilardi MF, Ghez C (1995) Impairments of reaching movements in patients without proprioception. I. Spatial errors. J Neurophysiol 73:1;347–360
Gracco VL, Abbs JH (1985) Dynamic control of the perioral system during speech: kinematic analyses of autogenic and nonautogenic sensorimotor processes. J Neurophysiol 54(2):418–432
Gribble PL, Ostry DJ (1998) Independent coactivation of shoulder and elbow muscles. Exp Brain Res 123:355–360
Gribble PL, Ostry DJ (1999) Compensation for interaction torques during single- and multijoint limb movement. J Neurophysiol 82:2310–2326
Guitton D (1992) Control of eye-head coordination during orienting gaze shifts. Trends Neurosci 15(5):174–179
Horak FB, Hlavacka F (2001) Somatosensory loss increases vestibulospinal sensitivity. J Neurophysiol 86:575–585
Horak FB, Shupert CL, Dietz V, Horstmann G (1994) Vestibular and somatosensory contributions to responses to head and body displacements in stance. Exp Brain Res 100:93–106
Horak FB, Lamarre Y, Macpherson JM, Shupert C, Henry SM (1996) Postural control associated with total body somatosensory loss. Soc Neurosci Abstr 22:1632
Inglis JT, Macpherson JM (1995) Bilateral labyrinthectomy in the cat: effects on the postural response to translation. J Neurophysiol 73(3):1181–1191
Inglis TJ, Shupert CL, Hlavacka F, Horak FB (1995) Effect of galvanic vestibular stimulation on human postural responses during support surface translations. J Neurophysiol 73(2):895–901
Johnston JL, Sharpe JA (1994) The initial vestibular-ocular reflex and its visual enhancement and cancellation in humans. Exp Brain Res 99(2):302–308
Karnath HO, Sievering D, Fetter M (1994) The interactive contribution of neck proprioception and vestibular stimulation to subjective “straight ahead” orientation in man. Exp Brain Res 101:140–146
Lajoie Y, Paillard J, Teasdale N, Bard C, Fleury M, Forget R, Lamarre Y (1992) Mirror drawing in a deafferented patient and normal subjects: visuoproprioceptive conflict. Neurology 42(5):1104–1106
Lajoie Y, Teasdale N, Cole JD et al. (1996) Gait of a deafferented subject without large myelinated sensory fibers below the neck. Neurology 47:109–115
Lashley K S (1951) The problem of serial order in behavior. In: Jeffress (ed) Cerebral mechanisms in behavior. Wiley, New York
Latash ML, Scholz JP, Schöner G (2002) Motor control strategies revealed in the structure of motor variability. Exerc Sport Sci Rev 30:26–31
Levin MF, Lamarre Y, Feldman AG (1995) Control variables and proprioceptive feedback in fast single-joint movement Can J Physiol Pharmacol 73(2):316–30
Li L, Steidl S, Yeomans JS (2001) Contributions of the vestibular nucleus and vestibulospinal tract to the startle reflex. Neuroscience 106(4):811–821
Lobel E, Kleine JF, Le Bihan D, Leroy-Willig A, Berthoz A (1998) Functional MRI of galvanic vestibular stimulation. J Neurophysiol 80:2699–2709
Ma S, Feldman AG (1995) Two functionally different synergies during arm reaching movements involving the trunk. J Neurophysiol 73:2120–2122
Mars F, Archambault PS, Paquet N, Feldman AG (2003) Vestibular contribution to arm-trunk coordination during pointing. Exp Brain Res 150:515–519
Nougier V, Bard C, Fleury M et al. (1996) Control of single-joint movements in deafferented patients: evidence for amplitude coding rather than position control. Exp Brain Res 109:473–482
Olausson H, Lamarre Y, Backlund H et al. (2002) Unmyelinated tactile afferents signal touch and project to insular cortex. Nat Neurosci 5:900–904
Pigeon P, Feldman AG (1998) Compensatory arm–trunk coordination in pointing movements is preserved in the absence of visual feedback. Brain Res 802:274–280
Pigeon P, Yahia LH, Mitnitski AB, Feldman AG (2000) Superposition of independent units of coordination during pointing movements involving the trunk with and without visual feedback. Exp Brain Res 131(3):336–349
Rossi E, Mitnitski A, Feldman AG (2002) Sequential control signals determine arm and trunk contributions to hand transport during reaching in humans. J Physiol (Lond) 538(2):659–671
Sainburg RL, Poizner H, Ghez C (1993) Loss of proprioception produces deficits in interjoint coordination. J Neurophysiol 70:5;2135–2147
Sainburg RL, Ghilardi MF, Poizner H, Ghez C (1995) Control of limb dynamics in normal subjects and patients without proprioception. J Neurophysiol 73:2;820–835
Sainburg RL, Ghez C, Kalakanis D (1999) Intersegmental dynamics are controlled by sequential anticipatory, error correction, and postural mechanisms. J Neurophysiol 81:3;1045–41056
Stapley PJ, Ting LH, Hulliger M, Macpherson JM (2002) Automatic postural responses are delayed by pyridoxine-induced somatosensory loss. J Neurosci 22(14):5803–5807
Tunik E, Poizner H, Levin MF et al. (2001) Role of proprioception in arm–trunk coordination during reaching with unexpected perturbation of the trunk (abstract). Program No. 302.10 Abstract Viewer/Itinerary Planner. Society for Neuroscience, Washington, DC
Watson SRD, Colebatch JG (1998a) Vestibular-evoked electromyographic responses in soleus: a comparison between click and galvanic stimulation. Exp Brain Res 119:504–510
Watson SRD, Colebatch JG (1998b) Vestibulocollic reflexes evoked by short-duration galvanic stimulation in man. J Neurophysiol 513(2):587–597
Weeks RA, Gerloff C, Dalakas M, Hallett M (1999) PET study of visually and non-visually guided finger movements in patients with severe pan-sensory neuropathies and healthy controls. Exp Brain Res 128(3):291–302
Welgampola MS, Colebatch JG (2001) Vestibulospinal reflexes: quantitative effects of sensory feedback and postural task. Exp Brain Res 130:345–353
Wilson V, Maeda M (1974) Connections between semicircular canals and neck motoneurons in the cat. J Neurophysiol 37:346–357
Wilson VJ, Zarzecki P, Shor RH et al. (1999) Cortical influences on the vestibular nuclei of the cat. Exp Brain Res 125:1–13
Acknowledgements
The authors thank Philippe Archambault for programming assistance. Special thanks to deafferented subjects C.F. and G.L. for participating. Research supported by NIH grant NS36449 (H.P.) and by grants from the Canadian Institutes for Health Research (CIHR) and from Les Fonds pour la Formation de Chercheurs et l’Aide à la Recherche (FCAR; Y.L., A.G.F., and M.F.L.).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tunik, E., Poizner, H., Levin, M.F. et al. Arm–trunk coordination in the absence of proprioception. Exp Brain Res 153, 343–355 (2003). https://doi.org/10.1007/s00221-003-1576-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-003-1576-4