
Abstract
Anticipatory postural adjustments (APAs) in preparation for predictable externally induced loading perturbation were studied in children with typically development (TD), hemiplegic (HEMI), and diplegic (DIPL) cerebral palsy. Twenty-seven children (n = 9 in each group) were asked to stand and catch a load dropped from a pre-specified height. Electrical activity of the leg and trunk muscles and center of pressure (COP) displacements were recorded to quantify the APAs. All groups were able to generate APAs prior to the perturbation, but the magnitude was smaller and the onset was delayed in the dorsal (agonist) postural muscles in both HEMI and DIPL as compared to TD. HEMI and DIPL also generated APAs in the antagonist postural muscles. Anticipatory backward COP displacement was significantly different from the baseline value only in the TD and HEMI. HEMI and DIPL displayed a different postural control strategy; HEMI showed no difference in background postural activity from TD, but with diminished APAs in the agonist postural muscles compared to TD, while DIPL showed a higher background postural activity and diminished APAs in the agonist postural muscles compared to TD. These differences are important to consider when designing rehabilitation programs to improve posture and movement control in children with hemiplegic and diplegic cerebral palsy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anticipatory postural adjustments (APAs) are defined as preemptive muscle activity that occurs prior to expected perturbations to the body (Belen’kiĭ et al. 1967). APAs are hypothesized to be generated by the central nervous system to counteract forthcoming perturbations created by voluntary movements or externally applied forces upon the body (Belen’kiĭ et al. 1967; Bouisset and Zattara 1987; Lacquaniti and Maioli 1987; Massion 1992). APAs have been extensively studied in healthy adults using different movement tasks and conditions (see review, Aruin 2002; Bouisset and Do 2008). In healthy adults, APAs are modulated based on the characteristics of the forthcoming perturbation such as direction of the perturbation or movement (Aruin and Latash 1995; Aruin et al. 2001), magnitude of the perturbation (Horak et al. 1984; Bouisset and Zattara 1987; Aruin and Latash 1996), task conditions such as available effective base of support (Gantchev and Dimitrova 1996; Slijper and Latash 2000; Aruin 2003), perceived stability (Adkin et al. 2002), and time constraints (Benvenuti et al. 1997; De Wolf et al. 1998).
Cerebral palsy (CP) is a neurodevelopmental condition caused by a non-progressive brain lesion that occurs before, during, or shortly after birth (Bax et al. 2005; Rosenbaum et al. 2007). Children with CP often present with difficulty maintaining their posture while engaging in functional activities. To better understand how their posture is coordinated during voluntary movements, researchers have examined APAs in individuals with CP. Impairments in APAs have been reported in children and adolescents with diplegic CP (Liu et al. 2007; Tomita et al. 2010b, 2013; Girolami et al. 2011) and recently in children with hemiplegic CP (Girolami et al. 2011). Although individuals with CP demonstrated the ability to generate APAs, the APAs were smaller and the onset was delayed when compared to healthy controls. Individuals with CP also demonstrated decreased ability to modulate APAs with respect to the direction and magnitude of the perturbation (Tomita et al. 2010b, 2013; Girolami et al. 2011). In addition, APAs quantified using center of pressure (COP) measurements show smaller excursions of COP as compared to healthy controls (Liu et al. 2007). In all of the APA studies in individuals with CP while standing, the tasks involved the use of voluntary movements to create perturbations (Liu et al. 2007; Zaino and McCoy 2008; Tomita et al. 2010b; Girolami et al. 2011). Because the magnitude of APAs normally scale with parameters of voluntary movement related to resultant perturbation, diminished and delayed onset of APAs in CP may be a by-product of their impaired movement performance, for example, due to slower and/or smaller movement increments to perform a whole task as compared to their control group (Chang et al. 2005; Liu et al. 2007; Ju et al. 2010). In contrast, in a load-catching paradigm, predictable and standardized external force is applied to the subjects to induce postural perturbation; a specified load is dropped onto a standing subject’s hands from a pre-specified height creating a quick forward rotational moment on body. This task allows for examination of APAs as the ability to predict and prepare for the forthcoming perturbation in a feedforward manner, independent of the individual’s ability to move similarly to that of healthy controls (Latash et al. 1995; Bennis et al. 1996). In healthy adults, this task is associated with anticipatory muscle activity in dorsal trunk and leg muscles just prior to load impact (Latash et al. 1995; Shiratori and Latash 2001). Unlike the previous APA studies in individuals with CP, which used voluntary upper extremity movements (Liu et al. 2007; Zaino and McCoy 2008; Tomita et al. 2010b; Girolami et al. 2011), studying APAs with the catching paradigm also affords the chance to understand how children with CP prepare their posture when interacting with objects in the environment. Catching is an important functional activity in which children frequently engage with peers, and is often a difficult task for children with hemiplegic and diplegic CP to coordinate. It will be important to investigate the differences in APA generation between diagnostic groups in order to develop appropriate intervention strategies.
The purpose of this study was to assess the differences in the anticipatory/feedforward postural adjustments (APAs) generated prior to a predictable external loading perturbation brought about by catching a load in children with typical development and children with hemiplegic and diplegic cerebral palsy.
Methods
Participants
Three groups of nine children between the ages of 7 and 17 years participated in this study (Table 1). The first group comprised of children who were typically developing (TD). The other two groups included individuals with a diagnosis of CP: spastic hemiplegia (HEMI) and spastic diplegia (DIPL). Prior to enrolling subject in the study, an IRB-approved questionnaire was used to conduct a telephone interview with each parent. The study was explained, and the parents were asked to verify that their child had no vision, hearing or cognitive issues that would impact the child’s ability to follow directions. In addition, when the parents and children arrived at the data collection site, each parent signed the consent form and each child read and signed the assent form, both of which were approved by University of Illinois at Chicago IRB. This interaction provided an additional opportunity to verify that vision, hearing and/or cognition would not interfere with the child’s ability to fully participate in the study.
The inclusion criteria for individuals with CP were the following: a medical diagnosis of cerebral palsy, Gross Motor Function Classification System (GMFCS) of I or II (children who can stand and ambulate without the use of an assistive device) (Palisano et al. 2008), no surgical or Botox interventions for 6 months prior to enrollment, and the ability to understand the procedures and follow directions. The children with CP were grouped by diagnosis and GMFCS based on a study by Damiano et al. (2006). This study objectively demonstrated that while children with different diagnoses may be placed in the same GMFCS level criteria, their performance on standardized functional measures is significantly different. Based on these findings, Damiano et al. (2006) strongly recommended that children be grouped first by diagnosis and then by GMFCS level. In our previous publication, we also reported differences in APAs generated by children in different diagnostic groups (Girolami et al. 2010). We feel that this may have implications for developing intervention paradigms.
Children in the TD group had no history of neurological or orthopedic conditions.
The side used for handwriting was designated as the dominant side for all subjects. For individuals in HEMI group, the dominant side was the less affected side. There were no significant group differences with respect to the height, weight, or age of the subjects.
Instrumentation
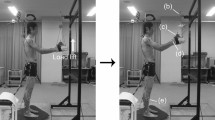
Figure 1 illustrates the experimental setup. The subjects performed the task while standing barefoot on a force platform (OR-6, AMTI, USA). The force platform was used to measure center of pressure displacements in the sagittal plane. A miniature unidirectional accelerometer (PCB Piezotronics, USA) was attached on the dominant hand with the axis of sensitivity oriented in the direction of the perturbation.

Experimental setup
Bipolar surface electromyographic activity (EMG) was recorded on the right and left sides of the body from the following muscles: erector spinae (ES, at the first lumbar level), rectus abdominis (RA, at the umbilicus level), biceps femoris (BF, half way on the line from ischial tuberosity to the lateral condyle of tibia), rectus femoris (RF, half way on the line from the ASIS to the caudal edge of patella), and medial soleus (SOL, at 2/3 to the line between the medial femoral condyle and the medial malleolus of tibia). The skin was cleaned with alcohol wipes, and pairs of disposable electrodes (8 mm diameter, Ag/AgCl, 20 mm inter-electrode distance) were placed over the muscle bellies on locations described in the literature (Basmajian 1980). A ground electrode was placed on the lateral condyle of the tibia. EMG signals were filtered and amplified (10–500 Hz, gain 2000) prior to digitization using an EMG system (Myopac, RUN Technologies, USA). The force platform, accelerometer and EMG signals were then digitized with a 16-bit resolution at 1000 Hz using customized LabView software (National Instruments, USA) and stored on a computer for future processing.
Procedure
The subjects were instructed to stand on the force platform with their bare feet placed shoulder width apart. Foot position was outlined with chalk on the force platform to ensure consistent foot placement during the data collection.
Subjects stood with arms outstretched in front of the body at shoulder height, while holding a 0.4 kg rectangular plastic basin with handles (Fig. 1). A load weighing 4 % of the subject’s body weight was hung on an external frame so that the bottom of the load was directly over the handheld basin, with a drop height of 0.245 m. The subjects were able to see the load at all times. A computer-generated tone indicated the load was about to be released. The load was dropped within 2 s after the tone. The subjects were instructed to catch the load that fell into the basin and maintain the standing posture for at least 3 s after the load landed in the basin. Each task consisted of 8 trials with a 10 s interval between each trial. The participants practiced 2–4 times prior to the data collection to familiarize themselves with the experimental task. All of the children with the diagnosis of CP were able to maintain the described position for the duration of the data collection with minimal verbal cueing from the experimenter.
Data processing
Offline analysis was performed using customized LabView software (National Instruments, USA) and MATLAB (Mathworks, USA).
The EMG signals were full-wave rectified and filtered using a second-order low-pass Butterworth filter with zero phase shift set at 100 Hz. Every trial was then viewed on a PC monitor and aligned based on the first deflection of the accelerometer signal, designated as time zero (T0). This time, detected by the accelerometer attached to the hand, marked the impact of the load. The aligned trials were then averaged for each subject.
The force platform and accelerometer signals were filtered using a 20-Hz low-pass, second-order Butterworth filter with zero phase shift.
EMG data
All the measurements below were obtained for each of the recorded muscles, for each subject.
The EMG integral indices were calculated from the averaged trials for each subject to quantify the magnitude of muscle activity for each muscle during 1) baseline EMG activity while standing with the plastic basin (∫EMGBL), which was defined as the integral of EMG activity during the period of −500 ms to −400 ms before the load impact (T0) and 2) anticipatory changes in muscle activity immediately prior to the load catch (∫EMGAPA), which was defined as the integral of EMG activity occurring from −150 ms to T0.
To compare baseline muscle activity among groups, ∫EMGBL was normalized to maximum EMG activity during the task performance in each muscle (n∫EMGBL). The maximum EMG activity from each trial per muscle for each subject was obtained, and these values were then averaged across trials to obtain maximal EMG value for each muscle per subject (maxEMG).
To compare the APAs among groups, baseline EMG activity was subtracted from the anticipatory EMG activity of each muscle as follows: ∆APA = ∫EMGAPA−1.5*∫EMGBL. The ∆APA value represents APA activity which is above or below the baseline muscle activity; no change in muscle activity from the baseline to APA phase is defined as 0. For group comparison of APA magnitude, ∆APA was also normalized with maxEMG (n∆APA). Muscle onset was obtained for each muscle within the time window from −500 ms to +500 ms with respect to T0, based on the averaged trials for each subject. Onsets were identified using a computer software program and visual inspection. The criteria for identifying the muscle onset was defined as the instant at which the EMG amplitude was greater than the baseline mean plus two standard deviations for at least 30 ms (Shiratori and Latash 2001). When the onset did not satisfy the above criteria, the onset was visually set (less than 6 % of the total trials).
COP data
Anticipatory COP displacement (COPAPA) was defined as the difference between the COP value at T0 and the baseline (500–400 ms before T0). COPAPA was also normalized with respect to each subject’s height (nCOPAPA)
Statistical analysis
All EMG measurements (∫EMGBL, ∫EMGAPA, ∆APA, n∫EMGBL, n∆APA, APA onset) were first analyzed to test whether there are differences in activity between the two body sides (dominant/non-dominant). Repeated measures analysis of variance (ANOVA) with factors GROUP (TD, HEMI, DIPL) × BODY SIDE (non-dominant, dominant) for each muscle (ES, RA, BF, RF, SOL) was run for each of the EMG measurements. All EMG measurements showed no statistically significant differences between the body sides for any of the participant groups. Therefore, the EMG measurements obtained from both sides of the body were pooled for further analysis.
To test whether there was a significant change in EMG activity between the baseline and APA phases for each muscle (ES, RA, BF, RF, SOL) within group, dependent t test was used to compare the muscle activities during baseline and APA phases (∫EMGBL and ∫EMGAPA) for each group.
To analyze whether there are group differences in the magnitude of baseline muscle activity (∫EMGBL, n∫EMGBL), APAs (∆APA, n∆APA) generated prior to load catching, and onset of APA activity (APA onset) in the muscles, one-way ANOVA was used for each of these measurements and for each muscle. Significant effects were further analyzed using post hoc Tukey’s HSD test.
To assess whether anticipatory COP displacement (COPAPA, nCOPAPA) was significantly different from the baseline value, a sample t test was used for within-group comparison. Comparison of COPAPA among groups was analyzed using one-way ANOVA. Significant effects were further analyzed using post hoc Tukey’s HSD test.
Statistical significance was set at p < 0.05.
Results
Acceleration
Of all the trials performed across subjects (8 trials/subject × 27 subjects = 216 trials), 7 trials were discarded due to unclear or abnormal acceleration signal which hindered the alignment of trials (3 % of total trials across subjects).
There were no between-group differences in the peak acceleration of hand immediately after the load impact (F (2,24) = 0.45, p = 0.65).
EMG profiles
Figure 2 shows the EMG traces during the performance of the catching task averaged across trials for a representative subject in each group: TD, HEMI, and DIPL. The EMG traces are of the dominant side. The child from the TD group showed a clear increase in the dorsal muscle activity (ES, BF, SOL) just prior to load impact, indicated with the vertical line at time 0. The child from the HEMI group showed smaller increase in the dorsal muscles prior to the load impact. The child from the DIPL group showed higher baseline activity and a slight increase in anticipatory activity in dorsal muscles, as well as increase in the ventral RF muscle activity.

EMG, COP, and acceleration traces of representative subjects in TD, HEMI, and DIPL groups performing the catching task. The vertical line at time zero (T0) indicates the instant of load impact. Activities of the ES, BF, and SOL (dorsal muscles) are indicated on the left y-axis, with positive activity projected upward. Activities of the RA and RF (ventral muscles) are shown on the right y-axis, with positive activity projected downward. The EMG traces are from the dominant side. The EMGs were collected in arbitrary units. Abbreviations—ES erector spinae, RA rectus abdominis, BF biceps femoris, RF rectus femoris, SOL soleus. COP backward displacement is in the negative direction
Baseline muscle activity
Inspection of individual EMG traces revealed that baseline EMG activity was higher for some of the children in DIPL group than for children in the TD or HEMI groups (see Fig. 2, ES, BF, and RF). To quantify the observation, baseline muscle activity (∫EMGBL) was compared among groups. The DIPL group generated significantly or close to significantly larger ∫EMGBL in the ES, BF, and RF muscles as compared to the TD and/or HEMI groups (see Table 2a for statistical results). In particular, baseline muscle activity was significantly higher for DIPL as compared to TD in the ES. DIPL group also had significantly higher and close to significantly higher baseline activity as compared to the HEMI for RF and BF muscles, respectively. To further test this effect, normalization of ∫EMGBL to a referent value was necessary. We tested the appropriateness of maximum EMG activity generated in each muscle for each person during the catch task (maxEMG) as a normalizing factor by comparing the value among groups. Significant group difference in maxEMG was only observed in RF muscle (one-way ANOVA, effect of GROUP, F (2,24) = 3.72, p < 0.05); thus, normalized RF values should be interpreted with caution. ∫EMGBL of all muscles except for RF was normalized to the maxEMG and compared among groups (n∫EMGBL). Significant group difference in n∫EMGBL values was still observed in ES and BF as well as RA, where DIPL had higher n∫EMGBL in these muscles compared to both TD and/or HEMI groups (See Table 2b for statistical results).
APA activity
Table 3 summarizes the statistical results comparing the muscle activity between baseline and APA phase (∫EMGBL, ∫EMGAPA) for each muscle and in each group. There is a statistically significant increase in muscle activity from the baseline phase to APA phase in all dorsal muscles (ES, BF, SOL) in TD, only in BF for HEMI, and in BF and SOL for DIPL. Only the CP groups showed changes in muscle activity from baseline to APA phase in the ventral muscles: HEMI showed an increase in RF from baseline to APAs phase, while DIPL showed a significant increase in both RA and RF muscles (See Table 3 for statistical results). In summary, both CP groups increased muscle activity from baseline to APA phase in BF and RF, indicating co-contraction in the BF-RF muscle pairs.
Figure 3 shows the group comparison of APA activity ∆APA and n∆APA for each muscle. For ∆APA, group differences were observed in all recorded muscles except for RA (GROUP effect indicated with † symbol next to the muscles, Fig. 3). Specifically, the TD group had significantly larger ∆APA in all the dorsal muscles as compared to the HEMI group. TD group also had a significant or close to significantly larger ∆APA in the dorsal muscles compared to the DIPL group in ES and BF. In contrast, DIPL group had significantly larger ∆APA in the ventral RF muscle as compared to TD and close to significantly larger ∆APA in RF compared to HEMI. The significant and close to significant post hoc group comparisons are indicated in Fig. 3.

a Mean and standard deviation of ∆APA for the 3 groups in the dorsal and ventral postural muscles. b Mean and standard deviation of n∆APA for the 3 groups in the dorsal and ventral postural muscles. For abbreviations, see Fig. 2. † Next to muscle labels on the x-axis indicates statistical significant GROUP effect with † p < 0.05, †† p < 0.005; * and brackets indicate significant post hoc group comparison with *p < 0.05, **p < 0.005
Group comparison of APA activity was also analyzed with normalized ∆APA value (n∆APA, see Fig. 3b). Group differences were still observed in the dorsal ES and BF muscles where TD group had significantly larger n∆APA than the two CP groups (see Fig. 3b for statistical results). RF muscle results for n∆APA should be interpreted with caution, as normalizing factor maxEMG was different among groups for this muscle.
Muscle onset
Table 4 shows mean onsets for each muscle. Negative and positive numbers represent the time before or after T0 (the instant of load impact) . TD group demonstrated significantly earlier onset in the ES and BF muscles as compared to the DIPL and/or HEMI groups (ES: GROUP effect, F (2,24) = 7.67, p < 0.005; post hoc, TD < HEMI, p < 0.05, TD < DIPL, p < 0.005. BF: GROUP effect, F(2,24) = 4.71, p < 0.05; post hoc, TD < HEMI, p = 0.05, TD < DIPL, p < 0.05).
Anticipatory COP displacement
In Fig. 4, representative subjects from each group show a posterior displacement of the COP, sustained until after the load impact (T0), followed by an anterior COP shift, and finally by another posterior shift of the COP. Anticipatory posterior COP shift prior to the load catch was observed for all subjects in TD, all except 1 subject in HEMI group, and all except 2 subjects in DIPL group. TD and HEMI groups showed significant changes in COPAPA from the baseline value (indicated with * on Fig. 4), while DIPL did not. However, there was no group difference in the COPAPA (F (2,24) = 1.04, p = 0.37). The results remained the same when the COPAPA was normalized to each subject’s height (nCOPAPA).

Mean anticipatory COP shift (COPAPA) and standard deviation for the three groups. Statistically significant posterior COPAPA shift from the baseline was observed for TD and HEMI, but not in DIPL group. Statistical significance is indicated by ** for p < 0.005 and * for p < 0.05. However, there are no statistical differences among the groups
Discussion
The purpose of this study was to characterize anticipatory postural adjustments in children with typical development and with cerebral palsy (spastic hemiplegia and spastic diplegia) in preparation for a predictable, externally induced, loading perturbation. The use of a load catch paradigm to study APAs in children with CP offers the possibility to better standardize the perturbation magnitude as compared to tasks which use voluntary movement to generate postural perturbations. The results of this study indicate that APAs are generated prior to an externally induced perturbation in children and adolescents with CP (GMFSC level I and II), as well as in typically developing children. However, the timing, quantity, and the recruited muscles for APAs as well as COP displacements prior to perturbation were different between groups.
APAs in children with CP
Catching a load in front of the body while standing is associated with an increase in dorsal trunk and leg muscle activity just prior to the load impact in healthy adults (Latash et al. 1995; Shiratori and Latash 2001). This preparatory muscle activity has been hypothesized to reduce the effect of the quick forward rotational moment produced by impact of the load on body posture (Lavender et al. 1993; Aruin et al. 2001; Shiratori and Latash 2001). In this study, the perturbation was delivered by dropping a load which was 4 % of the subject’s body weight from a height of 0.245 m above the bottom surface of a basin held by the subject. Significant changes in muscle activity were seen from baseline to the anticipatory phase in all 3 groups. Specifically, typically developing children demonstrated significant increase in dorsal (agonist) postural muscle activity (ES, BF, SOL), while children with CP showed significant increases in some dorsal and ventral muscles just prior to load impact. In addition, children with CP generated smaller changes in muscle activity from baseline to APA phases in the dorsal muscles, and the onset of anticipatory muscle activity was delayed compared to the healthy controls. In addition, anticipatory COP displacement was significantly different from baseline in TD and HEMI groups, but not in DIPL group.
Diminished and delayed APAs in agonist postural muscles of children with CP prior to voluntary movements such as bilateral shoulder flexion (Tomita et al. 2010b; Girolami et al. 2011) and shoulder extension (Girolami et al. 2011) while standing as compared to the healthy control groups have been previously reported. In addition, decreased anticipatory COP displacements have also been reported in bilateral shoulder flexion and extension tasks (Girolami et al. 2011) and in forward reaching task (Liu et al. 2007) while standing. Thus, the outcome of the current study taken together with the literature suggests that irrespective of whether APAs were generated in preparation for an external perturbation or for a self-initiated movement, children with CP demonstrate decreased and delayed onsets of APAs in the agonist postural muscles and smaller changes in anticipatory COP displacement than typically developing children.
It is notable that patients with Parkinson’s disease (Viallet et al. 1987; Latash et al. 1995), stroke (Garland et al. 1997; Slijper et al. 2002), and multiple sclerosis (Krishnan et al. 2012; Aruin et al. 2015), all demonstrated decreased and delayed APA activity in the agonist muscles. Thus, it appears that altered anticipatory postural adjustments are a feature displayed by patient populations with balance disorders.
Postural control in children with hemiplegic and diplegic CP
In standing functional tasks such as reaching or catching a ball, standing postural control provides a foundation for performing voluntary movements or resisting forces and torques that will be applied to the body. Thus, it is reasonable to consider that the postural control and associated muscle activity adopted during stance affect the generation of subsequent postural control mechanisms, including APAs.
Standing postural control has shown to be different between groups with CP and healthy controls. Individuals with cerebral palsy demonstrate decreased postural stability as compared to healthy controls during quiet standing (Ferdjallah et al. 2002; Donker et al. 2008; Saxena et al. 2014). In addition, postural stability deteriorates with decreased or conflicted sensory information more so in individuals with CP as compared to healthy controls (Cherng et al. 1999; Barela et al. 2011), suggesting that standing postural control is organized differently in CP than in healthy subjects.
However, in all of the studies looking at anticipatory muscle activation in CP, baseline activity during standing or sitting has been used to normalize the APA magnitude and was not used to characterize the activity itself or the impact it may have on the resultant anticipatory postural adjustments (Tomita et al. 2010b, 2011, 2013; Bigongiari et al. 2011; Girolami et al. 2011). Although our main purpose was to describe APAs in the three groups, we felt it was important to analyze the baseline muscle activity because there was a noticeable difference between the baseline muscle activity in the DIPL group as compared to the TD and HEMI groups. There is no agreement on methodology to normalize EMG data (Burden 2010), especially for groups with neuromuscular or neurodevelopment disorders (Hsu et al. 2006; Damiano et al. 2000). Hence, in this study, baseline and APAs activities have been analyzed using two quantification methods. We first used un-normalized values to describe what was seen on the EMG traces, followed by normalized values. Since both the non-normalized and normalized analysis methods may bias interpretations, we focused on results which were consistent in both analyses. As such, both analyses indicated that dorsal ES and BF muscles and possibly some ventral muscles are generating higher background activity during standing in the DIPL group as compared to TD. Subsequently, the APAs generated by the DIPL group were smaller in the dorsal ES and BF muscles as compared to TD in both non-normalized and normalized analyses. This higher baseline muscle activity and smaller APAs in the agonist postural muscles may have contributed to decreased anticipatory muscle activity and COP change in the DIPL group.
The higher baseline muscle activity generated by DIPL group in some postural muscles during standing could be a compensation strategy for their impaired ability to quickly activate the muscles (Moreau et al. 2012; Geertsen et al. 2015) to generate the anticipatory force necessary to sustain their posture and balance in preparation for the anticipated perturbation.
Alternatively, it could also be interpreted that the higher baseline postural muscle activity during standing is a default strategy adopted by children with diplegia and it is not specific to the direction of the forthcoming perturbation. The higher baseline muscle activity utilized to sustain standing posture in DIPL may have resulted in requiring small increase in APA activity in the dorsal postural muscles to counteract the forthcoming perturbation. It was reported that muscle activity in the leg and trunk muscles is less modulated with the demands of the standing postural task in children with diplegic CP compared to their control group (Tomita et al. 2010a). In our previous study looking at APAs in preparation for bilateral shoulder flexion and extension movements, baseline dorsal muscle activity was also consistently higher irrespective of the direction of the forthcoming voluntary movement for individuals with diplegic CP as compared to TD and HEMI groups (Girolami et al. 2011). Further investigation is required to discern whether standing posture in DIPL is adapted to the forthcoming requirement of the task or whether it is a default strategy that may aid or hinder the generation of subsequent postural adjustments.
Children with hemiplegic CP, on the contrary, generated baseline muscle activity no differently than the TD group in both analyses (non-normalized and normalized values). However, HEMI group generated significantly smaller magnitudes of APA activity in ES and BF dorsal muscles compared to the children in the control group for non-normalized and normalized values. Hence, the postural strategy used by the HEMI group, that of overall low muscle activity during the standing and APA phase, likely results in high reliance on the feedback postural control mechanisms to recover balance. This is a strategy normally adopted by healthy adults when the forthcoming perturbation is unpredictable (Toussaint et al. 1998; Santos et al. 2010). The results of the current study suggest that individuals with hemiplegia and diplegia differ in postural control strategies. Children with diplegic CP adopted a ‘less compliant’ postural control strategy for stance and as a result have decreased activity during the APA phases, while the children with hemiplegic CP group adopted a ‘more compliant’ postural control strategy during both stance and APA phases.
Our study is the second to report on APAs in individuals with hemiplegic CP during a standing postural task (Girolami et al. 2011). Much less is known about standing postural control, anticipatory or corrective postural adjustments during standing in this group as compared to diplegic CP. It has been reported that children with hemiplegia demonstrate body side asymmetry during voluntary movement, as well as asymmetry in muscle activity, strength, and associated biomechanical measures (Brown and Frank 1987; Dickstein et al. 2004; Feng et al. 2014). Therefore, we initially expected to find asymmetry in muscle activity during standing and APA phases in our study. However, in our study, children with hemiplegia did not demonstrate such asymmetries during the baseline (∫EMGBL, n∫EMGBL) and APAs (∫EMGAPA, ∆APA, n∆APA, APA onset) phases. In addition, no muscle activity asymmetry was observed between the dominant and non-dominant sides of DIPL or TD groups. This outcome could be related to the catching task itself. The catching task did not require the subject to perform overt voluntary movement. Rather, children were asked to stand and hold a lightweight basin in front of the body and to catch a load which was dropped into the center of the basin (midway between the right and left sides of the body). Thus, the posture adopted for this task and the nature of the perturbation may not have produced asymmetry in baseline or APA muscle activities between the affected and less affected sides of the body. It should be noted that the children in the HEMI group showed significant increase in EMG muscle activity from baseline to APA phase only in the BF-RF muscle pair as compared to other groups which showed APAs in other agonists (TD) and agonist/antagonist muscles (DIPL). Also, the HEMI group demonstrated that the magnitude of APAs was significantly smaller in all ES, BF, and SOL as compared to TD for the ∆APA, and in ES and BF for the n∆APA value, suggesting that there is smaller utilization of APAs for postural control as compared to TD or DIPL groups. It could be hypothesized that APAs are less utilized in children with hemiplegic CP due to the inherent asymmetric motor control; producing asymmetric APAs to symmetrical perturbation is counterproductive, leading to larger asymmetric body perturbation in all planes of motion after the perturbation is delivered to body posture. To our knowledge, there are no studies which quantified the asymmetry in muscle activity between body sides during stance or APAs in children with hemiplegia and warrants further investigation.
Posture and movement dysfunction in cerebral palsy significantly impact their daily function, participation, and quality of life (Rosenbaum et al. 2007). Although individuals with cerebral palsy receive rehabilitative services to improve and/or maintain movement and postural control, there is a lack of rehabilitation guidelines describing how to address movement and postural dysfunction in CP (Dewar et al. 2015). It would be beneficial to further expand our understanding of the interrelationship between postural control in sitting or standing and subsequent postural adjustments (APAs, compensatory postural adjustments (CPAs), and voluntary balance recovery) that occur with voluntary movement or externally induced perturbations. This would aid in developing comprehensive theoretical and clinically relevant evidence-based knowledge to more effectively develop treatment interventions for children with cerebral palsy. Postural control mechanisms are likely interconnected and influence each other; associations between APAs and CPAs have only recently started to be investigated (Santos et al. 2010). Therefore, the recommendation for rehabilitation at this time might include not only addressing each component of postural control (i.e., maintenance of standing/sitting postures, feedforward, feedback postural adjustments) in isolation, but also to incorporate interventions to address combined postural control interactions in rehabilitation programs for children with CP.
Limitations
We would like to acknowledge several limitations of this study. To be more descriptive regarding the upper extremity function of the children with cerebral palsy, we feel the Manual Assessment Classification Scale (MACS) (Eliasson et al. 2006) would have been a helpful addition to the classification protocol. This tool was published shortly after the onset of our data collection. However, this classification may be useful in future studies where arm movements or upper extremity functional skills are investigated. In addition, we did not use a standardized test to assess spasticity in our subjects with CP, such as the Ashworth Scale. Rather than using a measure of impairment, we chose to use a functional classification (GMFCS) as our experiment focused on APA generation in subjects who are independent walkers. It might be informative, however, to investigate whether spasticity measures correlate with APA generation in children with hemiplegia and diplegia. In future studies, we can consider this as part of our assessment protocol.
Conclusion
Individuals developing typically and individuals with hemiplegic and diplegic cerebral palsy (GMFCS I and II) were able to generate APAs in the leg and trunk muscles in preparation for a predictable externally induced loading perturbation. However, the APA magnitudes in the agonist dorsal postural muscles were smaller, and the onsets of APAs were delayed in children with CP as compared to children with typical development. Children with CP also generated APAs in the antagonist ventral postural muscles. In addition, there was a significant backward anticipatory shift in the COP in the children with typical development and children with hemiplegic CP, but the change in COP was not as substantial in children with diplegic CP. Notably higher baseline muscle activity was observed in some leg and trunk muscles in the children with diplegic CP as compared to typically developing children and/or children with hemiplegic CP. Future studies to understand the interrelationships between the components of postural control (standing balance, APAs, CPAs, and balance recovery from perturbations) is necessary to further elucidate the differences in postural control strategies adopted by children with hemiplegic and diplegic cerebral palsy.
References
Adkin AL, Frank JS, Carpenter MG, Peysar GW (2002) Fear of falling modifies anticipatory postural control. Exp Brain Res 143:160–170
Aruin AS (2002) The organization of anticipatory postural adjustments. J Autom Control 12:31–37
Aruin AS (2003) The effect of changes in the body configuration on anticipatory postural adjustments. Mot Control 7:264–277
Aruin AS, Latash ML (1995) Direction specificity of the postural muscles in feed-forward postural reaction during fast voluntary arm movements. Exp Brain Res 103:323–332
Aruin AS, Latash ML (1996) Anticipatory postural adjustments during self-initiated perturbations of different magnitude triggered by a standard motor action. Electroencephalogr Clin Neurophysiol Electromyogr 101:497–503
Aruin AS, Shiratori T, Latash ML (2001) The role of action in postural preparation for loading and unloading in standing subjects. Exp Brain Res 138:458–466
Aruin AS, Kanekar N, Lee Y-J (2015) Anticipatory and compensatory postural adjustments in individuals with multiple sclerosis in response to external perturbations. Neurosci Lett 591:182–186
Barela JA, Focks GMJ, Hilgeholt T, Barela AMF, Carvalho RP, Savelsbergh GJP (2011) Perception-action and adaptation in postural control of children and adolescents with cerebral palsy. Res Dev Dis 32:2075–2083
Basmajian JV (1980) Electromyography–dynamic gross anatomy: a review. Am J Anat 159(3):245–260
Bax M, Goldstein M, Rosenbaum P, Leviton A, Paneth N, Dan B et al (2005) Proposed definition and classification of cerebral palsy. Dev Med Child Neurol 47:571–576
Belen’kiĭ VE, Gurfinkel’ VS, Pal’tsev EI (1967) Control elements of voluntary movements. Biofizika 12:135–141
Bennis N, Roby-Brami A, Dufossé M, Bussel B (1996) Anticipatory responses to a self-applied load in normal subjects and hemiparetic patients. J Physiol Paris 90:27–42
Benvenuti F, Stanhope SJ, Thomas SL, Panzer VP, Hallett M (1997) Flexibility of anticipatory postural adjustments revealed by self-paced and reaction-time arm movements. Brain Res 761:59–70
Bigongiari A, Sausa FA, Franciulli F, Neto PM, Araujo RC, Mochizuki L (2011) Anticipatory and compensatory postural adjustments I sitting in children with cerebral palsy. Hum Mov Sci 30:648–657
Bouisset S (2008) Do M-CC. Posture, dynamic stability, and voluntary movement. Neurophysiol Clin 38:345–362
Bouisset S, Zattara M (1987) Biomechanical study of the programming of anticipatory postural adjustments associated with voluntary movement. J Biomech 20:735–742
Brown JE, Frank JS (1987) Influence of event anticipation on postural actions accompanying voluntary movement. Exp Brain Res 67:645–650
Burden A (2010) How should we normalize electromyograms obtained from healthy participants? What we have learned from over 25 years of research. J Electromyogr Kinesiol 20:1023–1035
Chang J-J, Wu T-I, Wu W-L, Su F-C (2010) Kinematical measure for spastic reaching in children with cerebral palsy. Clin Biomech (Bristol, Avon) 20:381–388
Cherng RJ, Su F-C, Chen J-J, Kuan T-S (1999) Performance of static standing balance in children with spastic diplegic cerebral palsy under altered sensory environments. Am J Phys Med Rehab 78:336–343
Damiano DL, Martellotta TL, Sullivan DJ, Granata KP, Abel MF (2000) Muscle force production and functional performance in spastic cerebral palsy: relationship of cocontraction. Arch Phys Med Rehabil 81:895–900
Damiano D, Abel M, Romness M, Oeffinger D, Tylkowski C, Gorton G, Bagley A, Nicholson D, Barnes D, Calmes J, Kryscio R, Rogers S (2006) Comparing functional profiles of children with hemiplegic and diplegic cerebral palsy in GMFCS Levels I and II: are separate classifications needed? Dev Med Child Neurol 48(10):797–803
De Wolf S, Slijper H, Latash ML (1998) Anticipatory postural adjustments during self-paced and reaction-time movements. Exp Brain Res 121:7–19
Dewar R, Love S, Johnston LM (2015) Exercise interventions improve postural control in children with cerebral palsy: a systematic review. Dev Med Child Neurol 57(6):504–520. doi:10.1111/dmcn.12660
Dickstein R, Shefi S, Marcovitz E, Villa Y (2004) Anticipatory postural adjustment in selected trunk muscles in poststroke hemiparetic patients. Arch Phys Med Rehabil 85:261–267
Donker S, Ledebt M, Roerdink M, Savelsberg GJP, Beek PJ (2008) Children with cerebral palsy exhibit greater and regular postural sway than typically developing children. Exp Brain Res 184:363–370
Eliasson AC, Krumlinde Sundholm L, Rösblad B, Beckung E, Arner M, Öhrvall AM, Rosenbaum P (2006) The manual ability classification system (MACS) for children with cerebral palsy: scale development and evidence of validity and reliability. Dev Med Child Neurol 48:549–554
Feng J, Pierce R, Do KP, Aiona M (2014) Motion of the center of mass in children with spastic hemiplegia: balance, energy transfer, and work performed by the affected leg versus the unaffected leg. Gait Posture 39:570–576
Ferdjallah M, Harris G, Smith P, Wertsch JJ (2002) Analysis of postural control synergies during quiet standing in healthy children and children with cerebral palsy. Clinical Biomech (Bristol, Avon) 17:203–210
Gantchev GN, Dimitrova DM (1996) Anticipatory postural adjustments associated with arm movements during balancing on unstable support surface. Int J Psychophysiol 22:117–122
Garland SJ, Stevenson TJ, Ivanova T (1997) Postural responses to unilateral arm perturbation in young, elderly, and hemiplegic subjects. Arch Phys Med Rehabil 78:1072–1077
Geertsen SS, Kirk H, Lorentzen J, Jorsal M, Johansson CB, Nielsen JB (2015) Impaired gait function in adults with cerebral palsy is associated with reduced rapid force generation and increased passive stiffness. Clin Neurophysiol http://www.ncbi.nlm.nih.gov/pubmed/25757398
Girolami GL, Shiratori T, Aruin AS (2010) Anticipatory postural adjustments in children with typical motor development. Exp Brain Res 205(2):153–165
Girolami GL, Shiratori T, Aruin AS (2011) Anticipatory postural adjustments in children with hemiplegia and diplegia. J Electromyogr Kinesiol 21:988–997
Horak FB, Esselman P, Anderson ME, Lynch MK (1984) The effects of movement velocity, mass displaced, and task certainty on associated postural adjustments made by normal and hemiplegic individuals. J Neurol Neurosurg Psychiatry 47:1020–1028
Hsu W-L, Krishnamoorthy V, Scholz JP (2006) An alternative test of electromyographic normalization in patients. Muscle Nerve 33:232–241
Ju YH, You JY, Cherng RJ (2010) Effect of task constraint on reaching performance in children with spastic diplegic cerebral palsy. Res Dev Disabil 31:1076–1082
Krishnan V, Kanekar N, Aruin AS (2012) Anticipatory postural adjustments in individuals with multiple sclerosis. Neurosci Lett 506:256–260
Lacquaniti F, Maioli C (1987) Anticipatory and reflex coactivation of antagonist muscles in catching. Brain Res 406:373–378
Latash ML, Aruin AS, Neyman I, Nicholas JJ (1995) Anticipatory postural adjustments during self inflicted and predictable perturbations in Parkinson’s disease. J Neurol Neurosurg Psychiatry 58:326–334
Lavender SA, Marras WS, Miller RA (1993) The development of response strategies in preparation for sudden loading to the torso. Spine 18:2097–2105
Liu W-Y, Zaino CA, McCoy SW (2007) Anticipatory postural adjustments in children with cerebral palsy and children with typical development. Pediatr Phys Ther 19:188–195
Massion J (1992) Movement, posture and equilibrium: interaction and coordination. Prog Neurobiol 38:35–56
Moreau N, Falvo M, Damiano D (2012) Rapid force generation is impaired in cerebral palsy and is related to decreased muscle size and functional mobility. Gait Posture. 35:154–158
Palisano RJ, Rosenbaum P, Bartlett D, Livingston MH (2008) Content validity of the expanded and revised Gross Motor Function Classification System. Dev Med Child Neurol 50:744–750
Rosenbaum P, Paneth N, Leviton A, Goldstein M, Bax M, Damiano D et al (2007) A report: the definition and classification of cerebral palsy April 2006. Dev Med Child Neurol Suppl 109:8–14
Santos MJ, Kanekar N, Aruin AS (2010) The role of anticipatory postural adjustments in compensatory control of posture: 1. Electromyographic analysis. J Electromyogr Kinesiol 20:388–397
Saxena S, Rao BK, Kumaran S (2014) Analysis of postural stability in children with cerebral palsy and children with typical development. Pediatr Phys Ther 26:325–330
Shiratori T, Latash M (2001) Anticipatory postural adjustments during load catching by standing subjects. Clin Neurophysiol 112:1250–1265
Slijper H, Latash M (2000) The effects of instability and additional hand support on anticipatory postural adjustments in leg, trunk, and arm muscles during standing. Exp Brain Res 135:81–93
Slijper H, Latash ML, Rao N, Aruin AS (2002) Task-specific modulation of anticipatory postural adjustments in individuals with hemiparesis. Clin Neurophysiol 113:642–655
Tomita H, Fujiwara K, Fukuya Y (2010a) Body alignment and postural muscle activity at quiet standing and anteriorposterior stability limits in children with spastic cerebral palsy. Disabil Rehabil 32:1232–1241
Tomita H, Fukaya Y, Honma S, Ueda T, Yamamoto Y, Shionoya K (2010b) Anticipatory postural muscle activity associated with bilateral arm flexion while standing in individuals with spastic diplegic cerebral palsy: a pilot study. Neurosci Lett 479:166–170
Tomita H, Fukuya Y, Ueda T, Honma S, Yamashita E, Yamamoto Y, Mori E, Shionoya K (2011) Deficits in task-specific modulation of anticipatory postural adjustments in individuals with spastic diplegic cerebral palsy. J Neurophys 105:2157–2168
Tomita H, Fukaya Y, Totsuka K, Tsukahara Y (2013) Deficits in anticipatory inhibition of postural muscle activity associated with load release while standing in individuals with spastic diplegic cerebral palsy. J Neurophys 109:1996–2006
Toussaint HM, Michies YM, Faber MN, Commissaris DCM, van Dieën JH (1998) Scaling anticipatory postural adjustments dependent on confidence of load estimation in a bi-manual whole-body lifting task. Exp Brain Res 120:85–94
Viallet F, Massion J, Massarino R, Khalil R (1987) Performance of a bimanual load-lifting task by parkinsonian patients. J Neurol Neurosurg Psychiatry 50:1274–1283
Zaino CA, McCoy SW (2008) Reliability and comparison of electromyographic and kinetic measurements during a standing reach task in children with and without cerebral palsy. Gait Posture. 27:128–137
Acknowledgments
We are thankful to the children and families who generously participated in this study. We thank D. Tan, PT, PCS and S. Joshi, PT, MS, PCS for assistance with data collection, and Ilyse Zultowski, DPT, PT for assistance with manuscript editing. This study was supported in part by a Grant from the Neuro-Developmental Treatment Association and by Pathways.org.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None of the authors have potential conflicts of interest to disclose.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Shiratori, T., Girolami, G. & Aruin, A. Anticipatory postural adjustments associated with a loading perturbation in children with hemiplegic and diplegic cerebral palsy. Exp Brain Res 234, 2967–2978 (2016). https://doi.org/10.1007/s00221-016-4699-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-016-4699-0