
Abstract
Background
Caffeine is a widely used dietary stimulant that can reverse the effects of fatigue on cognitive, motor and oculomotor function. However, few studies have examined the effect of caffeine on the oculomotor system when homeostasis has not been disrupted by physical fatigue. This study examined the influence of a moderate dose of caffeine on oculomotor control and visual perception in participants who were not fatigued.
Methods
Within a placebo-controlled crossover design, 13 healthy adults ingested caffeine (5 mg·kg−1 body mass) and were tested over 3 h. Eye movements, including saccades, smooth pursuit and optokinetic nystagmus, were measured using infrared oculography.
Results
Caffeine was associated with higher peak saccade velocities (472 ± 60° s−1) compared to placebo (455 ± 62° s−1). Quick phases of optokinetic nystagmus were also significantly faster with caffeine, whereas pursuit eye movements were unchanged. Non-oculomotor perceptual tasks (global motion and global orientation processing) were unaffected by caffeine.
Conclusions
These results show that oculomotor control is modulated by a moderate dose of caffeine in unfatigued humans. These effects are detectable in the kinematics of rapid eye movements, whereas pursuit eye movements and visual perception are unaffected. Oculomotor functions may be sensitive to changes in central catecholamines mediated via caffeine’s action as an adenosine antagonist, even when participants are not fatigued.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Caffeine is a widely used stimulant with fatigue-reversing properties. While caffeine is associated with both peripheral and central sites of action (Davis et al. 2003), the positive effects of caffeine (3–6 mg kg−1 body mass) on physical and cognitive performance is attributed to its stimulant effect on the central nervous system (CNS) (Davis et al. 2003; Ferre 2008). In the CNS, caffeine acts as a competitive adenosine antagonist, indirectly upregulating dopamine, and increasing the synthesis and turnover of norepinephrine (Fisone et al. 2004). These caffeine-induced changes in central neurotransmission are associated with improvements in psychomotor performance (Connell et al. 2016b), cognition and mood (Einöther 2013), and lead to overall enhancements in endurance exercise performance (Kovacs et al. 1998) and capacity (Hogervorst et al. 2008).
We have recently shown that prolonged exercise that causes brain-based fatigue in the corticospinal motor system also impairs the oculomotor system. Three hours of strenuous cycling decreased the velocity of rapid eye movements independently of other visual processes (such as dorsal cortical processing stream function) (Connell et al. 2016a, 2017). This finding is curious because the oculomotor system is functionally independent of the corticospinal system and not directly challenged by physical exercise.
These outcomes implicate a ubiquitous brain-based fatigue mechanism, which may be influenced by widespread disruptions in one or more neurotransmitter systems. The most likely neurochemicals involved are the central catecholamines, dopamine and norepinephrine (Taylor et al. 2016). Animal models suggest that these neurotransmitter systems experience significant perturbation during prolonged exercise (Hasegawa et al. 2008; Meeusen et al. 2003) and administration of pharmacological interventions that increase the availability of these catecholamines results in exercise performance improvements in humans (Cordery et al. 2016; Roelands et al. 2012).
In previous work, we have indirectly examined the involvement of catecholamines in fatigue development by administering caffeine during exercise and reporting fatigue-reversing properties in the oculomotor system. A moderate dose of caffeine during 3 h of prolonged exercise prevented fatigue-induced reductions in the velocity of saccades (Connell et al. 2016a, 2017) and the quick phase of optokinetic nystagmus (OKN) (Connell et al. 2017). Saccades are voluntary, high-velocity eye movements that enable rapid changes in fixation, whereas OKN is an oculomotor reflex characterised by alternating periods of slow tracking movements (slow phase) and rapid, resetting eye movements (quick phase) (Garbutt et al. 2001; Leigh and Zee 2006).
We subsequently addressed the role of catecholamines in this phenomenon more directly by comparing caffeine’s action with a dual dopamine-norepinephrine reuptake inhibitor (bupropion) that increases the availability of both monoamines. In these studies, caffeine and bupropion both preserved the velocity of saccades following 3 h of strenuous cycling. Thus, upregulation of catecholaminergic neurotransmission may underpin the fatigue-reversing effects of caffeine on oculomotor control. We also noted that the effects of fatigue and caffeine on oculomotor control appear to be independent from the processes supporting visual attention (Connell et al. 2016a, 2017) and visual perception (Connell et al. 2016a).
All of our work in this area to date has been conducted in the context of exercise-induced fatigue. The influence of caffeine on oculomotor control is yet to be explored comprehensively in unexercised, unfatigued participants. Under these conditions, the function of catecholaminergic neurotransmission is assumed to be optimal for controlling eye movements. It is unclear whether indirectly upregulating catecholamines at rest, via caffeine administration, can alter oculomotor control. The only study that has explored the impact of a small dose of caffeine in unexercised participants reported no change in saccadic latency, peak velocity or acceleration (Smith et al. 2003).
The aim of this exploratory study was to perform a thorough assessment of the influence of caffeine on visual function in well-rested, unfatigued participants. We examined the influence of caffeine on oculomotor control, visual attention and visual perception to determine if caffeine could exert an effect that is detectable in the absence of any significant homeostatic challenge.
In this experiment, saccadic eye movements, smooth pursuit, OKN and global motion and form perception were assessed before and after a 3 h interval. Prosaccade and antisaccade tasks were employed to explore the effect of caffeine on peripherally guided, reflexive saccades versus volitional saccades, respectively (Hallett 1978). Measures of visual attention were incorporated into the saccade tasks using a gap-overlap paradigm (Fischer et al. 1997; Jin and Reeves 2009). By manipulating the temporal relationship between the disappearance of the fixation point and the introduction of the peripheral target, the disengagement of attention is either facilitated or impeded, thereby influencing saccade latency and task performance (Hutton 2008; Jin and Reeves 2009). Thus, a gap-overlap paradigm was included to indicate whether caffeine is capable of modulating the cognitive processes involved in the disengagement or maintenance of visual attention. Smooth pursuit, a tracking eye movement that stabilises moving objects of interest on the retina (Lencer and Trillenberg 2008), was assessed with a simple triangular waveform target. Lastly, OKN was evoked using drifting square wave gratings. To investigate the influence of caffeine on extrastriate visual processing in both the dorsal and ventral streams, psychophysical measures of global motion and global form perception were obtained using a method of constant stimuli procedure (Clavagnier et al. 2016; Goodale 2011; Goodale and Milner 1992; Ungerleider and Haxby 1994).
Experimental procedures
Participants
Thirteen participants (seven females) with healthy cardiovascular function (maximal aerobic capacity 56 ± 7 ml kg min−1), a mean age of 23 (20–26) years and body mass of 72 ± 15 kg volunteered to participate. Average daily caffeine consumption was 54 mg (range, 0–231 mg day−1). One participant was a moderate caffeine user (170–400 mg day−1), nine were low caffeine users (<100 mg day−1), while the remainder had tried caffeine before, but did not consume habitually. Classifications of caffeine use are those outlined by Addicott et al. (2009). Participants gave written informed consent and visited the laboratory on three occasions to participate in a protocol conducted in accordance with the Declaration of Helsinki and approved by the University of Auckland Human Ethics Committee.
Experimental design
A moderate dose of caffeine (2 × 2.5 mg kg−1 body mass doses) or placebo (maltodextrin) was administered by capsule within a double-blind, placebo-controlled, repeated measures, randomised crossover design. Based on the average body mass dose (180 mg), this amount of caffeine is comparable to a 354 ml serving of brewed (~190 mg) or espresso-based coffee (e.g. Caffè Americano, ~150 mg) from popular US coffeehouse chains. Participants completed two experimental trials with a minimum of 5 days between crossover phases. In experimental trials, participants performed a battery of visual tasks (see below, ‘Visual performance measures’ section) immediately prior (pre) and upon completion (post) of a 180 min test interval. Treatment doses were received immediately before collection of pre-measures and 90 min into the test interval. Peak plasma concentrations of caffeine occur approximately 1 h after ingestion and the typical time of action is 4 to 6 h (Fredholm et al. 1999; Magkos and Kavouras 2005; Nehlig et al. 1992). The administration strategy was chosen to promote the effects of caffeine on subjective sensations consistently throughout the 180 min test interval and to ensure that the peak action of caffeine coincided with post-measures.
Preliminary tests
At least 1 week before the first experimental trial, participants were familiarized with study protocols. This involved becoming accustomed to the tasks within the visual test battery (see below, ‘Visual test battery’ section). Participants also performed a maximal cardiopulmonary exercise test on an electromagnetically braked cycle ergometer (Velotron Dynafit Pro, Seattle, WA, USA) with respiratory gas analysis equipment (pneumotachometer, MLT1000L, ADInstruments; paramagnetic oxygen analyser, S-3A/I, AEI Technologies; infrared carbon dioxide analyser, CD-3A, AEI Technologies) to measure peak oxygen uptake (VO2 peak) and estimate cardiorespiratory fitness (VO2 max).
Experimental protocol
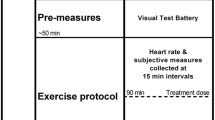
Participants arrived at the laboratory at 8 am following a 12 h overnight fast. Participants were instructed to abstain from caffeine for 24 h before each experimental trial. Upon arrival, the first treatment dose was consumed with a breakfast cereal. The quantity of breakfast was self-selected on the first visit and repeated for the second trial. Immediately after breakfast, the visual test battery was administered (see ‘Visual test battery’ section). Participants then waited for 180 min (test interval). At 90 min, the second treatment dose was administered. Participants drank water ad libitum throughout. During the test interval, participants engaged in self-selected sedentary activities such as reading, computer browsing or watching television. Heart rate was recorded at 15-min intervals along with self-rated arousal and mood assessed using visual analogue scales. At 180 min, participants completed the visual test battery. Figure 1 provides a schematic overview of the experimental protocol.

Experimental workflow. Thirteen participants were recruited. A familiarization session accustomed participants with the visual test battery. The two experimental sessions involved completion of the visual test battery at two time points, separated by a test interval lasting 180 min. Treatment doses were administered immediately prior to initial performance of the visual test battery (pre-measures) and at 90 min into the test interval
Visual test battery
The visual test battery consisted of six discrete tasks and took approximately 50 min to complete. The results from one of these tasks are reported elsewhere (Connell et al. 2016b). Stimuli were presented on a cathode ray tube monitor (Philips 109S2; 1280 × 1024 pixel resolution, 85 Hz refresh rate) at a viewing distance of 660 mm. Participants were comfortably seated in a quiet, darkened room. Head movements were minimised using a chin and forehead rest. Eye movements were tracked with a 400-Hz infrared eye tracker (ViewPoint Eye Tracker; Arrington Research Systems, Scottsdale, USA). A 16-point calibration procedure was carried out before the beginning of each eye movement task.
Antisaccade
The start of each trial was marked with the presentation of a black, central, circular fixation point subtending a visual angle of 0.5°. A black, circular peripheral target stimulus (0.5° diameter) then appeared ±10° to the left or right of the central fixation point, where it remained visible for 1000 ms. Participant instructions were to look away from the peripheral target stimulus to a mirror opposite position on the screen and to move their eyes to that position as quickly and accurately as possible.
The peripheral target was presented in a gap or overlap condition (Fischer et al. 1997). In the gap condition, the central fixation point was presented for 800 ms and extinguished 200 ms before peripheral target presentation. In the overlap condition, the central fixation point remained visible throughout the trial. Each condition was presented 50 times, resulting in a total of 100 trials. The order of gap, overlap, right target location, and left target location was randomised.
Prosaccade
The prosaccade task was identical to the antisaccade task. However, participants were instructed to move their eyes to look at the target stimulus as quickly and accurately as possible.
Smooth pursuit
A circular black dot (0.8° diameter) was presented in the centre of the screen (0°) for a duration of 1000 ms at the beginning of each trial. Following fixation, the target moved horizontally from the centre of the screen to one side until it reached ±15°, where it reversed direction abruptly and moved to the opposite side. On each trial, target speed was ramped to one of three velocities (5, 10 and 30° s−1). A trial consisted of 5.5 passes of the target across the display screen. Each target velocity was presented 7 times, resulting in 21 total trials. The sequence of target velocity and initial ramp direction were randomised. Participants were instructed to follow the target with their eyes as accurately as possible.
Optokinetic nystagmus (OKN)
Participants viewed a 100% contrast drifting square wave grating with a fundamental spatial frequency of 0.833 cycles per degree. Gratings were presented for a duration of 20 s per trial at two velocities (5 and 10° s−1) and two stimulus directions (right to left, or left to right) for two trials each, resulting in eight total trials. The stimulus speeds were slower than those often used in OKN studies, but were selected based on previous work that included assessment of both OKN and smooth pursuit eye movements (Kapoula et al. 2010; Konen et al. 2005). Participants were instructed to watch the screen, keeping the stimulus in focus. The objective of these instructions was to encourage a ‘stare’ OKN. Participants completed task practice sessions in the preliminary testing session for OKN, smooth pursuit and saccade tasks to ensure they were familiar with stimulus presentation, experimental setup and task requirements.
Global form and global motion perception
Perceptual thresholds for global orientation and global motion were measured using the method of constant stimuli. The stimulus was constructed from 100 Gabor elements distributed within an 8° aperture (Fig. 2). The elements within the aperture possessed both an orientation and a movement direction. Coherent (signal) elements had a consistent orientation (horizontal or vertical) and movement direction (left or right) whereas noise elements were random in their orientation and movement. On each trial, participants judged both the global orientation and motion direction of the stimulus, following a two-alternative-forced-choice procedure for each stimulus attribute. Task difficulty was modulated by varying the proportion of signal elements presented. Based on pilot observations, five stimulus intensities (percent signal elements) were presented for orientation (3, 12, 22, 31, 40%) and motion (5, 15, 25, 35, 45%). These were pre-allocated into 25 ordered pairs to ensure that all possible combinations of orientation and motion coherence stimulus intensities were presented. Participants completed a total of 250 trials (10 trials per ordered pair) presented in randomised order. Auditory feedback was provided. Elements did not travel within the central 1° of the stimulus aperture. Element diameter was 0.24°, speed was 2° s−1 and central fixation point diameter was 0.3°. Stimulus duration was 1000 ms. Elements had a limited lifetime where there was a 5% chance of the element being deleted and redrawn in a random location on each frame; this was to prevent participants tracking an individual element and, therefore, encouraged global integration of the stimuli. To acquaint participants with this task before experimental trials, a task demo was completed in the familiarization session. Participants were required to achieve a baseline level of competency. In the task demo, signal intensities were presented at 40, 60, 80, 100% (orientation) and 45, 65, 85, 100% (motion). A proportion correct >80% when presented with signal elements of 40 and 45% for global orientation and motion was required. If necessary, participants repeated the task until the required level of competency was attained.

Global orientation and motion stimulus properties. The stimulus for the global orientation and motion task consisted of 100 Gabor elements distributed within an 8° aperture. The elements within the aperture possessed both an orientation and a movement direction. The figure displays a stimulus presented with an orientation coherence of 31%
Data treatment and analysis
Stimulus presentation, data collection and data analysis were performed using custom software written in Matlab (MathWorks R2010b, Massachusetts, USA). All eye movement traces were visually inspected. Due to technical difficulties, the oculomotor data from one participant was not analysed. Similarly, the global form and motion perception data from a second participant were unavailable. Thus, n = 12 for all oculomotor tasks and the global motion and form task, while n = 13 for subjective measures (arousal, valence, heart rate). Final sample sizes for saccade, OKN, smooth pursuit and subjective measures satisfied a priori power analyses. This was estimated using an expected effect size of 0.4, derived from a previous study investigating eye movement kinematics within a similar experimental design (Connell et al. 2016a). Previous research suggests a high correlation (0.62–0.97) across repeated measures for saccades and smooth pursuit (Roy-Byrne et al. 1995). With power set to 0.95, p <0.05 and a correlation among repeated measures of 0.62, a sample size of 12 participants was estimated to provide appropriate statistical power for eye movement kinematic measures.
Prosaccades and antisaccades
Initiation of a saccade was automatically identified using a combined spatial (deviation of >1° from fixation) and a velocity criterion (≥30° s−1). The end of the saccade was detected by a drop in the saccade velocity below 30° s−1 (Ettinger et al. 2003; Hutton et al. 1998). Anticipatory saccades (latencies less than 70 ms) were excluded from analysis (Allman et al. 2012). Dependent variables derived from the saccade tasks were latency (ms), amplitude (°), peak velocity (° s−1) and task performance (percentage of saccades in the correct direction). For kinematic measures, only saccades performed in the correct direction were included in statistical analysis.
Smooth pursuit
Pursuit gain (eye velocity/target velocity) was the dependent measure of the smooth pursuit task. Saccades and blinks during pursuit were identified by computing a velocity signal from the horizontal eye position during each trial and applying a velocity criterion (≥64° s−1). Sections of pursuit containing saccades and blinks were removed before applying a linear interpolation to the remaining data to calculate eye velocity. Eye velocity was used to derive pursuit gain. The initial ramp in which the target only completed a pass across half of the screen was not included in analysis.
Optokinetic nystagmus
Quick phases were identified using the same velocity criterion employed for smooth pursuit analysis. Amplitude (°) and peak velocity (° s−1) were derived from the quick phases. Quick phase identification served as a basis for slow phase determination, as slow phases were assumed to occur between quick phases. Eye velocity during slow phases was calculated by applying a linear interpolation to the slow phase, thus permitting the calculation of slow phase gain.
Global form and global motion perception
Proportion correct for each stimulus intensity was calculated for the motion and form tasks separately. Global orientation coherence thresholds and global motion coherence thresholds (stimulus intensity at which the participant achieved 75% correct) were estimated by fitting Weibull functions to the proportion correct data with the tails fixed at 50 and 100% using a maximum-likelihood criterion procedure implemented in Palamedes toolbox (Prins and Kingdom 2009). Goodness-of-fit was assessed with a bootstrap analysis consisting of 500 simulations. This provided a p value representing the proportion of simulated deviance values greater that the deviance value of the fit for the collected data (Prins and Kingdom 2009). In the case where goodness-of-fit analysis resulted in p <0.05, the thresholds calculated for the corresponding participant were excluded from statistical analysis.
Statistical analyses
Repeated measures analyses of variance (ANOVA) with factors treatment (caffeine/placebo) and timepoint (pre/post) were used to determine the effect of treatment on global motion and global orientation thresholds. Condition (gap/overlap) was added as a factor to statistical analyses for dependent measures from the prosaccade and antisaccade tasks. Similarly, stimulus speed was added as a factor to statistical analyses for smooth pursuit gain (5, 10 and 30° s−1) and OKN slow and quick phases (5 and 10° s−1). There was no influence of stimulus direction, so this was not included as a factor in the statistical analysis.
To explore the influence of treatment on subjective experiences and heart rate, the number of levels within timepoint was extended to 13.
Due to the repeated measures design of the experiment, there was a possibility of task learning influencing our dependent variables. This was explored using the same repeated measures ANOVAs described above, with the factor trial (first vs. second) used in place of treatment. The presence of a task learning effect is identified where relevant.
Where necessary, interaction effects were explored using within-subject paired comparisons. The multiple comparison type I error rate was controlled using a false discovery rate criterion procedure (Benjamini et al. 2001). In cases where sphericity was violated, the Greenhouse-Geisser correction was used. Statistical significance was set at α = 0.05. Results are reported as mean ± standard deviation (SD) unless otherwise stated.
Results
Visual performance measures
Caffeine significantly influenced peak saccade velocity in the prosaccade task (main effect of treatment, F 1, 11 = 5.01, p < 0.05), with higher velocities in the caffeine treatment (472 ± 60° s−1) compared to placebo (455 ± 62° s−1). This increase occurred across both gap and overlap conditions (condition, F 1, 11 = 0.145, p = 0.71). Although velocity appeared to vary across time point depending on treatment (Table 1), an interaction between treatment × timepoint failed to reach statistical significance (F 1, 11 = 4.61, p = 0.055).
The influence of caffeine on peak prosaccade velocity was inspected further by collapsing the data across the factors condition and timepoint and calculating effect sizes for each participant. This allowed for a judgement of the magnitude of the difference between caffeine and placebo while accounting for within-subject variability. Eight of twelve participants exhibited higher saccade velocities with caffeine compared to placebo, with an average effect size of 0.3 ± 0.2 (range, 0.2–0.6). Two of the remaining four participants did not exhibit any difference in peak prosaccade velocity between placebo and caffeine, while the last two were faster in placebo compared to caffeine (effect sizes, 0.1 and 0.2). Figure 3a displays average peak prosaccade velocities in gap and overlap conditions collected for each participant.

Prosaccade peak velocity and latency for placebo (left) and caffeine (right) treatments. a Average peak prosaccade velocity (collapsed across gap and overlap trials) pre- and post-rest in placebo and caffeine treatments. Each point represents mean peak prosaccade velocity ± 95% CI for each participant. Dashed lines represent participants that exhibited faster prosaccade velocities with caffeine. b Prosaccade latency for gap and overlap conditions pre- and post-rest in placebo and caffeine. Significance labelling between gap and overlap conditions indicate a main effect of condition (*p < 0.05). Data represent mean ± SE
Given the small magnitude difference between peak velocities in caffeine compared to placebo treatments, an additional exploratory analysis was performed to investigate whether the effect of caffeine on prosaccade velocity was still evident when accounting for the variation of prosaccade amplitudes. The peak velocities of prosaccades in the caffeine and placebo treatments were compared using a linear mixed-effects model. This analysis method was selected because, for most participants, the amplitude range (1–15°) of prosaccades collected was too small to fit functions characterising the main sequence between amplitude and peak velocity. Prosaccades were collapsed across timepoint and condition and grouped in amplitude ranges of <7, 8 ± 1, 10 ± 1 and >11°. treatment and amplitude range were added to the model as fixed effects, while participant was considered a random effect. At the four amplitude ranges, faster peak velocities were observed in the caffeine treatment compared to placebo (main effect, treatment, F 3, 4569 = 15.16, p < 0.05). Furthermore, this effect was modulated by amplitude range (interaction effect, treatment × amplitude range, F 3, 4569 = 4.64, p < 0.05). Post hoc comparisons revealed significantly higher peak velocities in caffeine compared to placebo at the 8 ± 1° amplitude range, while there was no significant difference in peak velocity at the remaining amplitude ranges. This is unsurprising given that the largest number of saccades collected fell within the 8 ± 1° amplitude range (caffeine, 1249; placebo, 1350). The second largest number of saccades fell within the 10 ± 1° amplitude range (caffeine, 784; placebo, 855), followed by the <7° amplitude range (caffeine, 157; placebo, 122). Only 29 and 39 saccades resided in the >11° amplitude range for caffeine and placebo, respectively.
A robust main effect of condition was observed for prosaccade latency (F 1, 11 = 21.73, p < 0.01) and task performance (F 1, 11 = 6.66, p < 0.05), whereby prosaccades in the overlap condition were performed with longer latency and with better task performance compared to the gap condition. No changes were observed across time point or between treatments for prosaccade latency, amplitude or task performance.
Caffeine did not appear to influence the peak velocity of antisaccades (treatment, F 1, 11 = 1.788, p = 0.21). However, peak antisaccade velocity was significantly faster in the gap compared to the overlap condition (main effect of condition, F 1, 11 = 8.82, p < 0.05). This effect was present even when accounting for variations in saccade amplitude by assessing the data using a linear mixed-effects model. Condition also influenced antisaccade latency (F 1, 11 = 16.17, p < 0.01) and task performance (F 1, 11 = 28.68, p < 0.001), with longer latencies and higher performance in the overlap compared to the gap condition. These main effects were not accompanied by any interaction with time point or treatment. Furthermore, no alterations in antisaccade amplitude occurred. A task learning effect was uncovered in antisaccade latencies, whereby participants responded with shorter saccade latencies in the second experimental trial compared to the first (main effect of trial, F 1, 11 = 18.63, p < 0.01).
Smooth pursuit gain was unaffected by treatment and did not differ across time point. As expected, pursuit gain did differ depending on stimulus speeds (main effect of stimulus speed, F 2, 18 = 97.96, p < 0.001), with gains close to unity for the slowest stimulus speed (5° s−1), and progressively declining for faster stimulus speeds (10 and 30° s−1).
Caffeine was associated with alterations in amplitude and peak velocity of the quick phases of OKN. Quick phase amplitude was significantly influenced by caffeine (main effect of treatment, F 1, 11 = 7.12, p < 0.05) with slightly larger amplitudes with the caffeine treatment compared to placebo. Treatment also modulated the peak velocity of quick phases, which were significantly faster with caffeine (main effect of treatment, F 1, 11 = 9.85, p < 0.01). Larger amplitude quick phases occurred in response to the 10° s−1 stimulus compared to the 5° s−1 stimulus (main effect of stimulus speed, F 1, 11 = 21.10, p < 0.01). Similarly, quick peak velocities were higher in response to the 10° s−1 stimulus speed compared to the 5° s−1 stimulus speed (main effect of stimulus speed, F 1, 11 = 12.61, p < 0.01). Like smooth pursuit, OKN slow phase gain was unaffected by treatment and did not differ across time point. Additionally, there was no influence of stimulus speed on slow phase gain. These data, along with an example OKN trace from one participant, are illustrated in Fig. 4a–c.

Kinematic characteristics of OKN quick phases. a Sample eye movement traces of optokinetic nystagmus after caffeine (top traces) or placebo (bottom traces) in response to 10° s−1 (left traces) and 5° s−1 (right traces) stimulus speeds. b Mean amplitude of OKN quick phases in placebo and caffeine treatments. Each symbol represents one participant, while the shape of the symbol corresponds to one stimulus velocity: 5° s−1 (circle) and 10° s−1 (square). The diagonal unity line represents no difference between placebo and caffeine. c Mean peak velocity of OKN quick phases in placebo and caffeine. d Mean peak velocity of OKN quick phases for a given amplitude range in placebo and caffeine. Significance labelling indicates a significant difference in peak velocity in caffeine and placebo at the indicated amplitude, as revealed by post hoc comparisons (*p < 0.05). Data represent mean ± SE
Given the slightly larger quick phase amplitudes with caffeine (5°) compared to placebo (4°, refer to Table 1), an additional exploratory analysis was performed to investigate whether the higher peak velocities with caffeine result simply from an increase in amplitude. A linear mixed-effects model was used to compare the peak velocities of OKN quick phases in the caffeine treatment with those of the same amplitude in the placebo treatment. This analysis method was selected as the amplitude range of the quick phases collected for the majority of participants was too small to fit curves characterising the main sequence between amplitude and peak velocity. A linear relationship between quick phase amplitude and velocity was assumed as quick phases were less than 15° in amplitude (Bahill et al. 1975). Quick phases were collapsed across stimulus speed and timepoint and grouped in amplitude ranges of 2.5 ± 0.25°, 5.0 ± 0.5°, 7.5 ± 0.75° and 10.0 ± 1.0° (Wang et al. 2005). treatment and amplitude range were added to the model as fixed effects, while participant was considered a random effect. At the four amplitude ranges, significantly faster peak velocities were observed in the caffeine treatment compared to placebo. However, this effect was magnified at larger quick phase amplitudes (interaction effect, treatment × amplitude range, F 3, 72 = 2.79, p < 0.05). Post hoc comparisons revealed significantly higher peak velocities in the caffeine treatment compared to placebo at 5, 7.5 and 10° amplitude ranges, while there was no difference in peak velocity at the 2.5° amplitude range. These data are shown in Fig. 4d while kinematic and task performance data from all eye movement tasks are reported in Table 1.
One participant’s data was excluded from analysis of global orientation coherence, and data from three participants were excluded from global motion coherence analysis due to unacceptable fits. There were no effects of treatment on global orientation or global motion thresholds. A main effect of time point was detected for global motion threshold (F 1, 8 = 12.34, p < 0.01), with thresholds improving across time point, irrespective of treatment. These data are illustrated in Fig. 5a. Additional analyses suggested that this improvement reflected a within-trial task learning effect, as decreases in motion perception threshold were restricted to time points and not influenced by trial order (trial, F 1, 8 = 4.36, p = 0.07). For example, in trial one, motion coherence threshold improved from 24 ± 7 to 19 ± 5 and in trial two coherence thresholds decreased from 21 ± 6 to 19 ± 5, pre- and post-test interval, respectively. Global orientation thresholds also exhibited a learning effect. However, this occurred across trials as opposed to within trials (main effect of trial, F 1, 10 = 18.50, p < 0.01). Orientation thresholds decreased significantly from 19 ± 7 in trial one to 15 ± 6 in trial two.

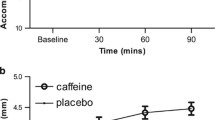
Motion perception, orientation perception, arousal and valence for placebo (white fill) and caffeine (black fill). a Motion and orientation coherence threshold (minimum motion or orientation signal required to discriminate coherent motion or orientation from random noise). Significance labelling with comparator represents a main effect of time point from pre-test to post-test coherence (*p < 0.05). b Felt arousal and valence across the 180-min rest duration in placebo and caffeine. Data represent mean ± SE
Subjective experiences
Heart rate differed significantly over the 180-min test interval depending on treatment and time point (F 12, 144 = 3.26, p < 0.001). This interaction stemmed from higher heart rates at the onset of the test interval with placebo compared to caffeine. As time progressed, heart rate slowed to a rate similar to the caffeine trial. As illustrated in Fig. 5b, self-reported mood and arousal was not influenced by treatment (mood, F 1, 12 = 1.25, p = 0.29; arousal, F 1, 12 = 2.78, p = 0.12), but both measures did increase over the course of the test interval, irrespective of treatment (main effect of timepoint, mood, F 2.70, 32.26 = 10.00, p < 0.001; arousal, F 1.98, 23.81 = 4.41, p < 0.05).
Discussion
This study demonstrates, for the first time, that caffeine can alter oculomotor function in unexercised, unfatigued participants. These changes manifest as detectable increases in the velocity of rapid eye movements (saccades and OKN quick phases), while visual attention and extrastriate visual function are unaffected by caffeine. This outcome is novel as existing evidence (Smith et al. 2003) suggested that caffeine (at a lower dose) has no influence on saccade kinematics in rested humans (Smith et al. 2003).
Eye movements in the prosaccade task were faster with a moderate dose of caffeine compared to placebo. Concurrent changes in amplitude were not observed. Thus, increases in peak velocity were not simply attributable to alterations in the distance travelled during the saccade. Eight of twelve participants exhibited higher prosaccade peak velocities in the caffeine treatment compared to placebo with an average effect size of 0.3. An effect size of this magnitude suggests that caffeine confers a small but detectable effect on peak velocity. Whether an increase in saccade velocity of this magnitude confers a beneficial effect on overall visual performance is unknown and is only likely to confer a positive benefit if saccadic duration (not reported here) is also shortened thereby allowing longer periods of fixation during search of the visual field. A previous study of saccades after a 1.5 mg kg−1body mass dose of caffeine found no changes in eye movement kinematics (Smith et al. 2003), suggesting there may be a minimum effective caffeine dose required to influence oculomotor control.
Similarly, the quick phases of OKN had significantly higher peak velocities in the caffeine treatment. However, this was accompanied by a concurrent increase in amplitude with caffeine. Additional analysis suggested that quick phases larger than 2.5° in amplitude exhibited a more pronounced increase in velocity with caffeine compared to quick phases of similar amplitudes in placebo. This is consistent with the increase in prosaccade peak velocity observed with caffeine. Saccadic eye movements are governed by a network of structures located within the cerebellum, frontal cortex and brainstem such as the frontal eye fields, superior colliculus and paramedian pontine reticular formation. Peak saccadic velocity is thought to indicate the function of a well-defined group of neurons located within the brain stem reticular formation. These neurons are also thought to be involved in the generation of OKN quick phases (Cohen 1972; Keller 1974). Thus, the alterations in peak velocity observed for prosaccades and OKN quick phases could possibly reflect a central influence of caffeine on the brainstem structures responsible for the generation of reflexive, rapid eye movements. However, we acknowledge that this interpretation is speculative as we have not used neurophysiological measures to directly examine the neural basis of the observed effects.
Nevertheless, this finding is congruent with the notion that the velocity component of rapid eye movements is especially sensitive to alterations in central nervous system activation (Galley 1989). For example, reductions in the peak velocity of saccades have been observed following the ingestion of sedative drugs (Busettini and Frölich 2014) and after periods of sleep deprivation ranging from one night to 64 h (Rowland et al. 2005; Zils et al. 2005). Additionally, the sedative drug diazepam reduces the amplitude and velocity of OKN quick phases (Wang et al. 2005). Conversely, administration of the stimulant drug methylphenidate has the opposite effect on rapid eye movements, increasing saccadic peak velocity (Allman et al. 2012).
Unlike prosaccades and quick phases, antisaccade kinematics were unaffected by caffeine. This may have been influenced by the difference in saccade dynamics between antisaccades and prosaccades (Bell et al. 2000; Smit et al. 1987). Antisaccades are commonly dysmetric and slower than prosaccades (Amador et al. 1998; Bell et al. 2000; Smit et al. 1987)—an effect also seen in this study. These differences have been attributed to the involvement of different neuronal subsystems to generate the appropriate saccade command given the task conditions (McDowell et al. 2008), as well as the absence of a target to direct the eyes towards in the antisaccade task (Olk and Kingstone 2003). The lower peak speeds and larger variations in amplitude observed with antisaccades may have influenced the sensitivity of this measure to the caffeine treatment, as even in prosaccades, which have higher peak velocities than antisaccades, only a small magnitude change in peak velocity with caffeine was detected.
We have previously reported a decrease in the velocity of 10° saccades following 3 h of exercise in a group of participants with a similar age range (20–31 years) and level of cardiorespiratory fitness (57 ± 1 ml kg min−1) to the present group (Connell et al. 2016a). No significant decline in prosaccade peak velocity over time occurred in the placebo treatment of the present study, suggesting that, in unfatigued participants, saccade velocity is stable over a 3 h period. Furthermore, no alterations across time were observed in the placebo treatment for other measures of oculomotor control in the prosaccade, antisaccade, smooth pursuit or OKN tasks. This is in line with previous research reporting that eye movement kinematics, including prosaccades, antisaccades and smooth pursuit, generally have high within-session temporal stability in rested, alert participants (Ettinger et al. 2003).
Visual attention was unaffected by the administration of caffeine, as a clear effect of gap and overlap conditions, similar in magnitude across treatments, was observed for saccade latency and task performance. Saccade latencies in the gap condition, for both prosaccade and antisaccade trials, were significantly shorter than those in the overlap condition, while task performance was higher in the overlap condition of both tasks. The gap condition facilitated a release of visual fixation due to the presence of a temporal gap between the offset of the fixation point and the onset of the peripheral target, thereby promoting faster saccade latencies and a higher proportion of direction errors (lower task performance). Conversely, in the overlap trials, the persistence of the fixation point during the onset of the peripheral target resulted in persistent fixation-related neural activity after target appearance, causing slower saccade latencies and fewer direction errors (Hutton 2008). Given that this gap-overlap effect on latencies and task performance was not modulated by caffeine, it appears that caffeine does not selectively influence the release or maintenance of visual fixation, nor does it exert a general effect on the mechanisms underlying disengagement and re-engagement of visual attention. However, in the antisaccade task, there is the possibility that an influence of caffeine was masked by a task learning effect. Self-rated arousal and mood was not influenced by caffeine, with levels of arousal and mood similar over the duration of the time interval in both treatments. Given this, it is unlikely that the visual performance measures were confounded by disturbances in mood and arousal.
Visual processing within the dorsal and ventral streams, the extrastriate areas supporting global motion and global orientation processing, were also unaffected by a moderate dose of caffeine. This is consistent with our previous finding that global motion detection and dorsal stream function are robust to exercise-induced fatigue with or without caffeine (Connell et al. 2016a). Furthermore, the task employed in the present study was more demanding than the global motion task used previously, as participants were required to process both orientation and motion components of the stimulus. It has been shown that healthy individuals are capable of judging the orientation and motional components of the stimulus without interaction, suggesting that the processes informing these judgements are largely independent (Clavagnier et al. 2016). Caffeine does not exert an effect on performance in this task either via heightened attention or by influencing processes within the dorsal and ventral streams to improve global motion and global orientation perception, respectively. The within- and between-trial improvements observed in global motion and global orientation threshold are likely to be a consequence of task learning despite the provision of a familiarization session before the first experimental measurement. However, it should be noted that the global orientation and motion perception data were underpowered based on the a priori power calculation. This was because participants with poor psychometric function fits were excluded.
A limitation of the current study is the homogeneity of the sample. The characteristics of the participants fell within a relatively narrow range of ages, levels of cardiorespiratory fitness and caffeine intakes. While these traits may have increased our ability to detect an effect of caffeine due to the possible reduction of population-related variance, the extent to which these results can be applied to a wider population is yet to be determined. The dietary caffeine intake of our cohort was low, and it is possible that higher caffeine intakes could differentially influence oculomotor control. This is a potential direction for future studies given that long-term exposure is known to modify the efficacy of caffeine on cognition and physical performance (Sokmen et al. 2008). Additionally, while the interpretation of caffeine effects has largely focused on central mechanisms, caffeine is also associated with a range of peripheral actions, including increases in intracellular calcium mobilisation and inhibition of phosphodiesterases (Nehlig et al. 1992), which may alter the contractile properties of skeletal muscle (Lopes et al. 1983). This peripheral action of caffeine could influence saccade velocity if the extra-ocular muscles were similarly affected and warrants further investigation.
In conclusion, this study provides evidence that it is possible to increase the velocity of rapid eye movements in unfatigued humans with caffeine. A moderate dose of caffeine caused detectable changes in oculomotor control, demonstrating that caffeine can alter normal oculomotor function. These stimulant effects may occur via upregulation of central catecholaminergic activity (Connell et al. 2017). The findings further our understanding of visual function and oculomotor control in the context of dietary caffeine intake.
References
Addicott MA, Yang LL, Peiffer AM, Laurienti PJ (2009) Methodological considerations for the quantification of self-reported caffeine use. Psychopharmacology 203(3):571–578. doi:10.1007/s00213-008-1403-5
Allman A-A, Ettinger U, Joober R, O’Driscoll GA (2012) Effects of methylphenidate on basic and higher-order oculomotor functions. J Psychopharmacol 26(11):1471–1479
Amador N, Schlag-Rey M, Schlag J (1998) Primate antisaccades. I. Behavioral characteristics. J Neurophysiol 80(4):1775–1786
Bahill AT, Clark MR, Stark L (1975) The main sequence, a tool for studying human eye movements. Math Biosci 24(3):191–204
Bell AH, Everling S, Munoz DP (2000) Influence of stimulus eccentricity and direction on characteristics of pro- and antisaccades in non-human primates. J Neurophysiol 84(5):2595–2604
Benjamini Y, Drai D, Elmer G, Kafkafi N, Golani I (2001) Controlling the false discovery rate in behavior genetics research. Behav Brain Res 125(1–2):279–284
Busettini C, Frölich MA (2014) Effects of mild to moderate sedation on saccadic eye movements. Behav Brain Res 272:286–302. doi:10.1016/j.bbr.2014.07.012
Clavagnier S, Polito V, Hess R (2016) How independent are global form and global motion processings? J Vis 16(12):185–185. doi:10.1167/16.12.185
Cohen B (1972) Origin of quick phases of nystagmus. Prog Brain Res 37:544–545
Connell CJW, Thompson B, Kuhn G, Claffey MP, Duncan S, Gant N (2016a) Fatigue related impairments in oculomotor control are prevented by caffeine. Scientific Reports 6:26614
Connell CJW, Thompson B, Kuhn G, Gant N (2016b) Exercise-induced fatigue and caffeine supplementation affect psychomotor performance but not covert visuo-spatial attention. PLoS One 11(10):e0165318
Connell CJW, Thompson B, Turuwhenua J, Srzich A, Gant N (2017) Fatigue-related impairments in oculomotor control are prevented by norepinephrine-dopamine reuptake inhibition. Scientific Reports 7:42726
Cordery, P., Peirce, N., Maughan, R. J., & Watson, P. (2016). Dopamine/noradrenaline reuptake inhibition in women improves endurance exercise performance in the heat. Scandinavian Journal of Medicine and Science in Sports.
Davis JM, Zhao Z, Stock HS, Mehl KA, Buggy J, Hand GA (2003) Central nervous system effects of caffeine and adenosine on fatigue. American Journal of Physiology: Regulatory, Integrative and Comparative Physiology 284(2):R399–R404
Einöther ST (2013) Caffeine as an attention enhancer: reviewing existing assumptions. Psychopharmacology 225(2):251–274. doi:10.1007/s00213-012-2917-4
Ettinger U, Kumari V, Crawford TJ, Davis RE, Sharma T, Corr PJ (2003) Reliability of smooth pursuit, fixation, and saccadic eye movements. Psychophysiology 40(4):620–628
Ferre S (2008) An update on the mechanisms of the psychostimulant effects of caffeine. J Neurochem 105(4):1067–1079
Fischer B, Gezeck S, Hartnegg K (1997) The analysis of saccadic eye movements from gap and overlap paradigms. Brain Res Protocol 2(1):47–52
Fisone G, Borgkvist A, Usiello A (2004) Caffeine as a psychomotor stimulant: mechanism of action. Cell Mol Life Sci 61(7–8):857–872
Fredholm B, Bättig K, Holmén J, Nehlig A, Zvartau E (1999) Actions of caffeine in the brain with special reference to factors that contribute to its widespread use. Pharmacol Rev 51(1):83–133
Galley N (1989) Saccadic eye movement velocity as an indicator of (de) activation. A review and some speculations. J Psychophysiol 3(3):229–244
Garbutt S, Harwood M, Harris C (2001) Comparison of the main sequence of reflexive saccades and the quick phases of optokinetic nystagmus. Br J Ophthalmol 85(12):1477–1483
Goodale MA (2011) Transforming vision into action. Vis Res 51(13):1567–1587
Goodale MA, Milner D (1992) Separate visual pathways for perception and action. Trends Neurosci 15(1):20–25
Hallett PE (1978) Primary and secondary saccades to goals defined by instructions. Vis Res 18(10):1279–1296. doi:10.1016/0042-6989(78)90218-3
Hasegawa H, Piacentini MF, Sarre S, Michotte Y, Ishiwata T, Meeusen R (2008) Influence of brain catecholamines on the development of fatigue in exercising rats in the heat. J Physiol 586(1):141–149
Hogervorst E, Bandelow S, Schmitt J, Jentjens R, Oliveira M, Allgrove J et al (2008) Caffeine improves physical and cognitive performance during exhaustive exercise. Med Sci Sports Exerc 40(10):1841–1851. doi:10.1249/MSS.0b013e31817bb8b7
Hutton SB (2008) Cognitive control of saccadic eye movements. Brain Cogn 68(3):327–340
Hutton SB, Crawford TJ, Puri BK, Duncan LJ, Chapman M, Kennard C et al (1998) Smooth pursuit and saccadic abnormalities in first-episode schizophrenia. Psychol Med 28(3):685–692
Jin Z, Reeves A (2009) Attentional release in the saccadic gap effect. Vis Res 49(16):2045–2055. doi:10.1016/j.visres.2009.02.015
Kapoula Z, Yang Q, Vernet M, Bonfils P, Londero A (2010) Eye movement abnormalities in somatic tinnitus: fixation, smooth pursuit and optokinetic nystagmus. Auris Nasus Larynx 37(3):314–321. doi:10.1016/j.anl.2009.10.004
Keller E (1974) Participation of medial pontine reticular formation in eye movement generation in monkey. J Neurophysiol 37(2):316–332
Konen CS, Kleiser R, Seitz RJ, Bremmer F (2005) An fMRI study of optokinetic nystagmus and smooth-pursuit eye movements in humans. Exp Brain Res 165(2):203–216. doi:10.1007/s00221-005-2289-7
Kovacs EM, Stegen J, Brouns F (1998) Effect of caffeinated drinks on substrate metabolism, caffeine excretion, and performance. J Appl Physiol 85(2):709–715
Leigh RJ, Zee DS (2006) The neurology of eye movements. Oxford University Press, Oxford
Lencer R, Trillenberg P (2008) Neurophysiology and neuroanatomy of smooth pursuit in humans. Brain Cogn 68(3):219–228
Lopes JM, Aubier M, Jardim J, Aranda JV, Macklem PT (1983) Effect of caffeine on skeletal muscle function before and after fatigue. J Appl Physiol 54(5):1303–1305
Magkos F, Kavouras SA (2005) Caffeine use in sports, pharmacokinetics in man, and cellular mechanisms of action. Crit Rev Food Sci Nutr 45(7–8):535–562
McDowell JE, Dyckman KA, Austin BP, Clementz BA (2008) Neurophysiology and neuroanatomy of reflexive and volitional saccades: evidence from studies of humans. Brain Cogn 68(3):255–270
Meeusen R, Sarre S, De Meirleir K, Ebinger G, Michotte Y (2003) The effects of running speed and running duration on extracellular dopamine levels in rat striatum, measured with microdialysis. Medicina Sportiva 7(1):E29–E36
Nehlig A, Daval JL, Debry G (1992) Caffeine and the central nervous system: mechanisms of action, biochemical, metabolic and psychostimulant effects. Brain Res Rev 17(2):139–170
Olk B, Kingstone A (2003) Why are antisaccades slower than prosaccades? A novel finding using a new paradigm. Neuroreport 14(1):151–155
Prins, N., & Kingdom, F. A. A. (2009). Palamedes: Matlab routines for analyzing psychophysical data. Retrieved from http://www.palamedestoolbox.org
Roelands B, Watson P, Cordery P, Decoster S, Debaste E, Maughan R, Meeusen R (2012) A dopamine/noradrenaline reuptake inhibitor improves performance in the heat, but only at the maximum therapeutic dose. Scand J Med Sci Sports 22(5):e93–e98
Rowland LM, Thomas ML, Thorne DR, Sing HC, Krichmar JL, Davis HQ et al (2005) Oculomotor responses during partial and total sleep deprivation. Aviat Space Environ Med 76(7):C104–C113
Roy-Byrne P, Radant A, Wingerson D, Cowley DS (1995) Human oculomotor function: reliability and diurnal variation. Biol Psychiatry 38(2):92–97
Smit AC, Van Gisbergen JAM, Cools AR (1987) A parametric analysis of human saccades in different experimental paradigms. Vis Res 27(10):1745–1762
Smith A, Brice C, Nash J, Rich N, Nutt DJ (2003) Caffeine and central noradrenaline: effects on mood, cognitive performance, eye movements and cardiovascular function. J Psychopharmacol 17(3):283–292
Sokmen B, Armstrong LE, Kraemer WJ, Casa DJ, Dias JC, Judelson DA, Maresh CM (2008) Caffeine use in sports: considerations for the athlete. Journal of Strength and Conditioning Research 22(3):978–986
Taylor, J. L., Amann, M., Duchateau, J., Meeusen, R., & Rice, C. L. (2016). Neural contributions to muscle fatigue: from the brain to the muscle and back again. Medicine and Science in Sports and Exercise.
Ungerleider LG, Haxby JV (1994) ‘What’and ‘where’ in the human brain. Curr Opin Neurobiol 4(2):157–165
Wang C, Tian J, Liang P, Sun F (2005) Diazepam-induced changes of optokinetic nystagmus fast phase. Exp Brain Res 167(3):446–450. doi:10.1007/s00221-005-0176-x
Zils E, Sprenger A, Heide W, Born J, Gais S (2005) Differential effects of sleep deprivation on saccadic eye movements. Sleep 28(9):1109
Acknowledgements
We thank the participants who volunteered their time to take part in the study. We are grateful to Hayden Green for his assistance in data collection.
Author information
Authors and Affiliations
Contributions
Conceptualization: C.J.W.C., B.T. and N.G.; methodology: C.J.W.C., B.T. and N.G.; software: C.J.W.C., J.T. and R.H.; formal analysis: C.J.W.C.; investigation: C.J.W.C.; resources: N.G.; writing—original draft: C.J.W.C.; writing—review and editing: C.J.W.C., N.G. and B.T.; supervision: N.G.
Corresponding author
Ethics declarations
Competing interests
The authors have no competing financial interests to declare.
Rights and permissions
About this article

Cite this article
Connell, C.J.W., Thompson, B., Turuwhenua, J. et al. Caffeine increases the velocity of rapid eye movements in unfatigued humans. Psychopharmacology 234, 2311–2323 (2017). https://doi.org/10.1007/s00213-017-4638-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-017-4638-1