
Abstract
Tris(2-butoxyethyl) phosphate (TBOEP; 20 µg/kg b.w.) was orally administered to three female and three male volunteers. In urine samples collected for 39 h three metabolites of TBOEP were quantitated. bis(2-butoxyethyl) phosphate (BBOEP), tris(2-(3-hydroxy)butoxyethyl) phosphate (OH-TBOEP), bis(2-butoxyethyl)-(2-hydroxyethyl) phosphate (BBOEHEP) were observed in all urine samples within the first 7 h with highest concentration for BBOEHEP. C max of OH-TBOEP was in the range of 2–4 h and t 1/2 was between 1.5 and 6.1 h. Similar results were obtained for BBOEHEP. In contrast BBOEP showed several maxima within 25 h and, therefore, no toxicokinetic data were calculated. As proof of concept 54 urine samples of children staying at day-care centers in Germany were analysed for all 3 biomarkers. Only BBOEP and BBOEHEP were detected in about 80% of the samples with a median of 0.16 µg/l for BBOEP and 0.18 µg/l for BBOEHEP. A recalculation of daily intake (DI) based on BBOEHEP resulted in a clear undercut of the current reference dose of 50 µg/kg per day. As observed in other studies a calculation of the DI based on the dust concentrations and oral uptake of 20 mg of dust for 8 h for young children results in considerably higher DI but would also not exceed the RfD.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Organophosphate esters (OPs) have both plasticizing and flame retardant properties and claimed a share of 11.5% of the total consumption of flame retardants (ATSDR 2012). Therefore, OPs were used in diverse commercial and industrial products since the 1940s and were worldwide observed in different environmental media (Möller et al. 2012). Tris(2-butoxyethyl) phosphate (TBOEP) is produced by chemical synthesis via condensation of phosphorus oxychloride and butoxyethanol as described elsewhere. It is mainly used as a component in floor polishes, a solvent in some resins, a viscosity modifier in plastisols, an antifoam, and also as a plasticizer in synthetic rubber, plastics and lacquers (Van der Veen and de Boer 2012).
TBOEP has been detected in residences at levels up to several mg/kg, with median concentrations of 0.07–9 900 µg/kg for TBOEP in indoor dust samples (Ali et al. 2012a, b; Bergh et al. 2011; Brommer et al. 2012; Cequier et al. 2014; Dodson et al. 2012; Garcia et al. 2007; Tajima et al. 2014; Van den Eede et al. 2011) and in indoor air of 0.6–1.8 ng/m3 (Bergh et al. 2011; Cequier et al. 2014; Otake et al. 2004; Saito et al. 2007; Staaf and Ostman 2005). Compared with residences, slightly higher values were reported for other indoor environments, such as offices, day-care centers, schools and transport vehicles (Ali et al. 2012b; Bergh et al. 2011; Brandsma et al. 2014; Cequier et al. 2014; Fromme et al. 2014; Hartmann et al. 2004; Staaf and Ostman 2005). Results of TBOEP in diet are very limited. Sundkvist et al. found concentrations from 270 to 1000 ng/g l.w. in freshwater fish near sources, but only values < LOQ (< 3 to < 28 ng/g l.w.) in freshwater fish at background sites and marine fishes (Sundkvist et al. 2010). In 8 pooled breast milk samples from Sweden collected in 1997–2006 a median of 4.7 ng/g l.w. with a range of < LOQ—63 ng/g l.w. was observed from Sundkvist et al. as well. In a more recent study in three Asian countries breast milk samples were collected between 2008 and 2011 (Kim et al. 2014). Higher values were observed for the Philippines (< 0.03—209 ng/g l.w.), but very low concentrations in Japan and especially in Vietnam. In the US FDA total diet study performed between 1986 and 1991 a mean daily intake between 0.9 and 5.2 ng/kg b.w., depending on age group, was calculated for TBOEP (Gunderson 1995). In a more recent study from Sweden using 53 composite samples from 12 food categories collected in 2015 TBOEP was not detected in any sample (Poma et al. 2017).
With regard to environmental and health effects of TBOEP various reviews have summarized the scientific literature especially the Agency for Toxic Substances and Disease Registry (ATSDR 2012). TBOEP has a low acute toxicity with oral LD50 values of 13,278 and 5383 mg/kg were reported in male and female rats (ATSDR 2012). After dermal exposure TBOEP shows a slight to moderate erythema in rabbits with dose-related incidence and severity (ATSDR 2012). TBOEP is nonmutagenic in in vitro tests with prokaryotic organisms (i.e. Salmonella typhimurium) and mammalian cell systems with and without metabolic activation as summarized in (ATSDR 2012). In cell-based transactivation assays against various human nuclear receptors only a dose-dependent activation of the pregnane X receptor (PXR) was observed, but no effect on other receptors such as estrogen, androgen, glucocorticoid, and thyroid hormone receptor (Kojima et al. 2013). Subchronic feeding to Wistar rats resulted in increased liver weights and an increased incidence of periportal hepatocyte swelling and vacuolization in males with NOAELs of 18 and 20 mg/kg b.w. (Saitoh et al. 1994). No endocrine, hematological, renal, or musculoskeletal effects were seen. Neurotoxic effects of TBOEP are inconsistent, but a reduction of nerve conduction velocity was reported (Laham et al. 1984, 1985). TBOEP have been examined in oral studies that included exposure during gestation and in general, these studies did not report fetotoxicity or teratogenicity even at doses that produced maternal toxicity (ATSDR 2012). Some new studies tested TBOEP for endocrine activity (Egloff et al. 2014; Jin et al. 2016).
Generally OPs were fast hydrolyzed to the corresponding Di-ester and other minor metabolites were formed after oxidation as described for different OPs in mice and rats (Burka et al. 1991; Kurebayashi et al. 1985; Nishimaki-Mogami et al. 1988; Suzuki et al. 1984). Due to the molecular weight of the OPs the metabolites were excreted with urine or feces. No information on the uptake, distribution and elimination of TBOEP in rodents and humans are currently available but the formation of the corresponding Di-ester is very likely especially since the Di-ester was detected in human urine samples as previously described (Fromme et al. 2014). But such hydrolysis may occur under versatile conditions as described especially for phthalates such as DEHP and, therefore, Di-ester of TBOEP may not be so specific for the internal exposure (Mittermeier et al. 2016). Therefore, secondary metabolites for example oxidized or hydroxylated metabolites may be more specific metabolites of TBOEP. Recently for TBOEP a hydroxylated metabolite could be detected after using human liver microsomes and human liver S9 fractions (Van den Eede et al. 2013a). In addition the group of Covaci quantitated in 59 urine samples of adults several metabolites of different OPs (Van den Eede et al. 2013b). For TBOEP only the Di-ester was quantified with a low detection frequency and a median near the limit of detection of 0.15 ng/ml. These findings raise questions concerning the bioavailability of TBOEP and its metabolism in humans.
Therefore, the objective of this study is to obtain basic toxicokinetic parameters for males and females after the administration of a single oral dose of TBOEP. The obtained results of the excretion of typical metabolites in urine should be further used in human biomonitoring studies for the recalculation of the exposure of humans.
Material and method
Exposure of subjects
The basic characteristics of three female subjects (F1, F2, F3) and three male subjects (M1, M2, M3) are given in Table 1. The volunteers were between 37 and 58 years old, weighed 62–109 kg, and lived in Munich or the surrounding areas. Subjects were healthy as judged by medical examination with clinical blood chemistry a few days before the start of the study. The study was carried out according to the Declaration of Helsinki and the study protocol was approved by the ethical committee of the Bavarian Medical Association (no.: 14030). After being verbally informed and in written form about the aims, background and extent of health risks all voluntarily participating subjects provided their written informed consent.
A dose of 20 µg/kg b.w. TBOEP was orally administered in an olive oil to the six participants. Urine samples from the subjects were collected in intervals starting 1 h after administration up to 39 h with the exception of one male volunteer who collected urine for 46 h. After urine volume was measured, samples were stored at – 20 °C using sterile polyethylene specimen cups.
In addition 54 urine samples from children were investigated for the metabolites of TBOEP, collected in 2011/12 in day-care centers as described in detail elsewhere (Fromme et al. 2013, 2014). The children were 20–80 months old and weighed 10–39 kg, median and mean 18 kg. All the parents provided their written informed consent. The urine samples were collected after staying some hours in the centers.
Chemicals
TBOEP (tris(2-butoxyethyl) phosphate, purity ≥ 95%) was provided by Tokyo Chemical Industry Co., Ltd. (TCI) Deutschland GmbH (Eschborn, Germany). Tris(2-(3-hydroxy)butoxyethyl) phosphate (OH-TBOEP), bis(2-butoxyethyl)-(2-hydroxyethyl) phosphate (BBOEHEP), bis(2-butoxyethyl) phosphate (BBOEP) and the corresponding internal standards d4-tris(2-(3-hydroxy)butoxyethyl) phosphate (d4-OH-TBOEP), d4-bis(2-butoxyethyl)-(2-hydroxyethyl) phosphate (d4-BBOEHEP) d4-bis(2-butoxyethyl) phosphate (d4-BBOEP) (purities ≥ 95% determined with 1H-NMR) were synthesized by Dr. Belov, Max-Planck Institute for Biophysical Chemistry Göttingen, Germany.
Acetonitrile (LC–MS grade) was purchased from Fisher Scientific (Loughborough, UK), methanol (HiPerSolv) was from VWR (Ismaning, Germany) and ammonium acetate p.a. was from Honeywell Riedel-de-Haën AG (Seelze, Germany).
Beta-glucuronidase from Helix pomatia, Type H-2, [CAS 9001-45-0), Enzyme Commission (EC) Number 3.2.1.31], aqueous solution, ≥ 85.000 units/ml was purchased from Sigma-Aldrich Chemie GmbH (Steinheim, Germany).
Ultrapure water (18.2 MΩ ≤ 3 ppb TOC) was obtained from a Milipore Milli-Q Integral 3 Elix water purification instrument from Merck (Molsheim, France).
Analysis of metabolites
After thawing two volumes of 200 µl urine were each transferred into 2 ml Eppendorf vials and spiked with 10 µl internal standard mix (containing a concentration of 1 ng/µl d4-BBOEP, d4-OH-TBOEP and d4-BBOEHEP). A volume of 65 µl 0.1 M ammonium acetate and 5 µl of beta-glucuronidase were added to the samples which were then sealed and vortex mixed.
All samples were treated in a thermomixer (MHR 23, HLC Biotech, Bovenden, Germany) for 17 h at 37 °C.
After the treatment a volume of 250 µl acetonitrile was added for protein denaturation. The samples were mixed thoroughly before they were centrifuged at 16,048g for 10 min.
After the centrifugation the supernatant fluid of each sample was transferred into its own HPLC glass vial and mixed with 470 µl of ultrapure water.
Standard preparation
A stock solution (100 ng/µl) for all analytes was prepared in methanol/water (50/50, v/v) and then further diluted with methanol/water (50/50, v/v) to obtain standard mix working solutions with concentrations of 1, 10 and 100 pg/µl as well as 1 and 10 ng/µl.
Calibration
For the calibration solutions with different concentrations (0, 0.01, 0.05, 0.10, 0.50, 1.00, 5.00, 10.00, 40.00, 70.00 and 100.00 µg/l) were prepared as follows:
A volume of 200 µl of a native corresponding calibration standard was mixed with 70 µl of 0.1 M ammonium acetate, 10 µl internal standard mix (1 ng/µl), 250 µl acetonitrile and 470 µl ultrapure water to get the different concentrations described before. At least two samples were prepared and measured for every concentration.
Quantitation
An internal standard method based on isotope labelled standards was used for quantitation. For calibration the ratio of the peak area of standard to internal standard was plotted versus the concentration by Multiquant 3.0.2 software with a suitable regression type and a 1/x weighting.
Liquid chromatography
An UltiMate™ 3000 (Thermo Scientific, Dreieich, Germany) was used for separation by high pressure liquid chromatography and the column oven temperature was set to 35 °C.
The auto sampler introduced 200 µl of the sample into the system. Pump 1 (HPG-3200SD, Thermo Scientific, Dreieich, Germany) carried the mobile phase (100% 2 mM ammonium acetate buffer solution, A) to load the sample onto the trap column (Oasis® HLB, 25 µm, 2.1 mm × 20 mm, Waters, Eschborn, Germany) with a flow rate of 1 ml/min. After 2 min the sample loading and elimination of matrix components were completed and then the 10-port valve (Thermo Scientific, Dreieich, Germany) switched into the elution position. Pump 2 (HPG-3200SD, Thermo Scientific, Dreieich, Germany) flushed the trapped analytes back from the trap column onto the analytical column (SunShell C18, 2.6 µm, 2.1 mm × 100 mm, ChromaNik Technologies Inc., Osaka, Japan with a Security Guard column C18, 4 mm × 2 mm, Phenomenex, Aschaffenburg, Germany) with a flow rate of 200 µl/min and a composition of 60% methanol (B) and 40% 2 mM ammonium acetate buffer (A). The composition and flow were kept constant for 4.2 min followed by a gradient to 95% methanol (B) and 5% 2 mM ammonium acetate within 0.24 min. This final composition was kept constant and after 13 min the valve switched back to its first position.
Mass spectrometry
All quantitations were performed using a 5500 QTRAP™ mass spectrometer from SCIEX (Darmstadt, Germany). Following settings were used to record the spectral data: polarity: positive; CAD gas: medium (N2); curtain gas: 35 (N2); collision gas: medium; ion spray voltage: 5000 V (for more details see Table 2).
Precision
To determine the intraday and inter day precision three times 1.5 ml was taken from a pooled urine sample. Two of the 1.5 ml volumes of urine were spiked at different concentrations while the third one was left untreated. For every concentration six samples were analyzed on two different days. These samples were handled as described before. Recoveries and coefficient of variation were specified. Recovery rates were calculated as the quotient of spiked concentration to measured concentration multiplied with 100; in case of any content in the non-spiked samples, the “measured concentration” was corrected for this value.
Limit of detection and quantitation
Limits of detection were defined as three times the standard deviation of the calculated concentration of five different blank samples. Limits of quantitation were defined as three times of the limit of detection.
Statistical
The statistical analyses were performed with Microsoft Excel 2010. Exponential regression modelling based on log-lin plots was used to calculate k after C max for each volunteer as previously described (Kessler et al. 2012). k is the metabolite-specific renal excretion constant (log C(t)/C(0) = −k Δt). Half times were calculated with natural logarithm of two divided by k (t 1/2 = ln 2/k).
Results
Quality control
For a concentration of 0.5 µg/l of each metabolite tested in urine an intraday coefficient of variation (C V) (n = 6) of < 6% and accuracy between 82 and 101% were obtained. Inter day C V (n = 3) was < 5% and accuracy was between 80 and 99%.
Toxicokinetics
The aim of this study was to verify proposed (Van den Eede et al. 2013a) metabolites in human volunteers administered a controlled dose of TBOEP (20 µg/kg b.w.). After quantitation of detected metabolites in urine toxicokinetic data were calculated and based on these results the exposure of humans should be recalculated in ongoing and prospective human biomonitoring studies. Therefore, no blood samples were collected. Based on the experience of many toxicokinetic studies an enzymatic hydrolysis was performed to get the unconjugated metabolites. With some samples from the toxicokinetic study it was tested whether conjugated metabolites occur and afterwards it was tested after what time the hydrolysis was complete. As expected both hydroxylated metabolites are nearly quantitatively conjugated and after 17 h the hydrolysis was complete.
Besides bis(2-butoxyethyl) phosphate (BBOEP) two hydroxylated metabolites tris(2-(3-hydroxy)butoxyethyl) phosphate (OH-TBOEP) and bis(2-butoxyethyl)-(2-hydroxyethyl) phosphate (BBOEHEP) were detected in urine samples of all volunteers within the first hours. As shown in Figs. 1, 2 and 3 only for OH-TBOEP and BBOEHEP a typical elimination curve with highest concentrations within the first 5 h were observed. In contrast BBOEP provides some maxima within 25 h and only after this time a smooth decline in concentrations could be observed. At time 0 h, before administration OH-TBOEP could not be detected in any sample with a limit of quantitation (LOQ) of 0.03 µg/l and both BBOEHEP and BBOEP were only observed in a few samples near to the LOQ of 0.04, respectively, 0.1 µg/l.

Concentration-time courses of BBOEP in urine after a single oral dose of 20 µg/kg b.w. (TBOEP) mean values ± SD

Concentration-time courses of BBOEHEP in urine after a single oral dose of 20 µg/kg b.w. (TBOEP) mean values ± SD

Concentration-time courses of OH-TBOEP in urine after a single oral dose of 20 µg/kg b.w. (TBOEP) mean values ± SD
The maximum concentrations C max of BBOEHEP and OH-TBOEP were observed between 1 and 3 h for all volunteers (Table 3). For a single subject, the corresponding t 1/2 values were between 2.4 and 5.3 h for BBOEHEP and 1.5 and 6.1 h for OH-TBOEP. As displayed in Table 3 the mean of half times of the females was shorter compared to males, especially for OH-TBOEP. For BBOEP more than four C max were obtained as shown in Fig. 1 and, therefore, it is not reasonable to calculate t 1/2 values. However, the first maxima were reached after 1–4 h (t max; Table 3). A mean of C max of the first maxima was 0.024 nmol/kg b.w. (Table 3).
As already visible in Figs. 1, 2 and 3, the excreted amounts of each metabolite is quite different so for BBOEHEP highest concentration up to 3700 pmol/kg b.w., for OH-TBOEP only up to 3.6 pmol/kg b.w. and for BBOEP up to 69 pmol/kg b.w were obtained. As displayed in Table 4 a mean of 8.3% of the administered dose was obtained for BBOEHEP, 0.8% for BBOEP and 0.02% for OH-TBOEP. However, especially for BBOEHEP the percentage of excretion varies largely from 2.1 to 21.5% for all 6 participants (Table 4). The variation was larger in females compared to males but the median were similar with 5.2% for females and 6.4% for males.
Quantitation of TBOEP metabolites in real urine samples
As proof of concept the new biomarkers observed in the toxicokinetic study were quantitated in 54 urine samples of young children. As expected OH-TBOEP could not be detected in any sample above the LOQ of 0.03 µg/l. BBOEHEP and BBOEP could be quantitated in 78 and 80% of the samples, respectively. For BBOEHEP a median (95th percentile) of 0.18 µg/l (1.29 µg/l) was observed and for BBOEP a median (95th percentile) of 0.16 µg/l (1.55 µg/l) was calculated, respectively (Table 5). With a factor of urinary excretion (F ue) the daily intake could be calculated using the equation:
with C urine for the concentration of the metabolite in μg/l and UVexcr for the daily excreted urinary volume of 22.2 ml/kg b.w. per day for children (Miller and Stapleton 1989), F ue for the molar fraction of urinary excretion and the molecular weights (MW) of the compound (c) and the corresponding metabolite (m) as described elsewhere.
As shown in Table 5 the median (95th percentile) DI of TBOEP was 0.05 µg/kg b.w. (0.40 µg/kg b.w.) using a F ue of 0.0838. In contrast to BBOEHEP with BBOEP a DI of 0.6 µg/kg b.w. (median) and 5.9 µg/kg b.w. (95th percentile) was calculated.
Calculation based on uptake via dust ingestion
All 54 urine samples of the children were collected after they attended one of the 16 day-care centers. As described previously in all facilities dust samples were collected simultaneously. A median concentration of 412 µg/g TBOEP dust was obtained and a mean of 858 µg/g, respectively, a 95th percentile of 3517 µg/g were calculated. With a mean ingestion of 20 mg of dust within 8 h as suggested by the US-EPA (EPA 2011) an approximately ninefold higher DI compared to the calculation with BBOEHEP was obtained but the results are similar to the calculation with BBOEP as shown in Table 5.
In addition means were calculated for the urine samples from each day-care center (n = 12 of 16) with 3 and more samples. The correlation of the mean values with the concentrations of TBOEP in each day-care center is displayed in Fig. 4 for BBOEHEP. A relatively good correlation with R 2 = 0.77 was obtained. For BBOEP a correlation with R 2 = 0.68 was found.

Correlation between urinary concentrations of BBOEHEP in children from day-care centers and TBOEP concentration in dust of the corresponding day-care center (n = 12)
Risk assessment
The National Sanitation Foundation (NSF) derived a reference dose (RfD) of 0.05 mg/kg per day from a human equivalent BMDL10 of 15 mg/kg per day http://www.techstreet.com/nsf/standards/nsf-tris-2-butoxyethyl-phosphate-2012?product_id=1857403. BMDL10 based on periportal hepatocellular hypertrophy in Sprague–Dawley rats orally administered TBOEP for 18 weeks (Reyna and Thake 1987). No chronic study was available to assess progression of the hypertrophic response. Therefore, NSF applied an uncertainty factor of 300 (10 to account for intraspecies extrapolation, 10 to account for interspecies extrapolation, and 3 for subchronic to chronic extrapolation and incomplete database) to derive the RfD of 0.05 mg/kg b.w. per day.
Median, mean and 95th percentile values of DI calculated from the 54 urine samples analysed in the study are clearly below at least a factor of eight of the RfD of 50 µg/kg b.w. per day (Table 5). Especially the values calculated from BBOEHEP as the most reasonable biomarker of TBOEP (see discussion for more details) are more than 100-fold below the RfD.
Discussion
Metabolism and toxicokinetics
To our knowledge no data are available on the kinetics or metabolism of TBOEP neither in animals nor humans. Using the toxicokinetic data it is possible to calculate a total daily intake from exploratory studies.
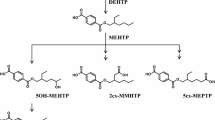
As described before some metabolites of TBOEP were proposed due to the detection in human urine samples and in in vitro metabolism assays. Three of these proposed metabolites were commercially synthesized and used in the human exposure study.
All 3 metabolites could be quantitated in the first hours after administration of the dose of 20 µg/kg b.w. which is below the current RfD of 50 µg/kg b.w. per day. RfD is defined as the maximum acceptable oral dose of a toxic substance by US-EPA. As expected both hydroxylated metabolites BBOEHEP and OH-TBOEP are quantitatively conjugated to glucuronides as known from BPA or several secondary phthalate metabolites also in young children (Völkel et al. 2011, 2014). In contrast to the monoester derivatives of phthalates for the diester derivative BBOEP of TBOEP no conjugated metabolite was detected in urine samples. Similar results were described for diethyl phosphate as diester metabolite of chlorpyrifos (Bicker et al. 2005) and glucuronide conjugates of hydroxyl triphenyl phosphate of the flame retardant and plasticizer triphenyl phosphate (Su et al. 2016).
For diethyl phosphate Bicker et al. calculated half times in a biphasic kinetic model of 25.1 h in a so called fast elimination phase and of 141.5 h in a so called slow elimination phase (Bicker et al. 2005) which seems similar to the multiphasic elimination curve of BBOEP within 39 h displayed in Fig. 1. Therefore, a higher percentage of excretion of BBOEP is most likely if samples would be collected for a longer time as described in the case study of Bicker et al. (Bicker et al. 2005). However, the excretion of BBOEP with urine will be in the low percent range since levels decrease with time as displayed in Fig. 1. Although variations between volunteers (coefficient of variation; C V = 20%) are small compared to BBOEHEP with a C V of 82% (Table 4). BBOEP isn’t the most suitable biomarker to recalculate the daily intake (DI) of TBOEP due to the low percentage of excretion. OH-TBOEP and BBOEHEP show short t 1/2 (< 6 h) and should be reasonable biomarker for DI calculations but the excretion rate of OH-TBOEP is so low that in unintentionally exposed people a detection of OH-TBOEP could not be expected as shown for 54 urine samples of unintentionally exposed children. So the most suitable biomarker of TBOEP is BBOEHEP.
Human biomonitoring to calculate DI
Both BBOEHEP and BBOEP could be quantitated in about 80% of urine samples of children (n = 54). Also similar are the statistical data such as median, etc. If only F ue of both compound are considered this is really surprising because BBOEHEP shows approximately 11-fold (F ue BBOEHEP/F ue BBOEP) higher levels compared to BBOEP (Table 5). As discussed before the long half time of BBOEP explains this observation and provides for each individual person a concentration in urine much higher as expected. Therefore, it is difficult to calculate the DI based on BBOEP and explains the fact that DI displayed in Table 5 are so different. If a steady state concentration of BBOEP in urine would be determined, an adjusted F ue could be used to calculate DI of TBOEP, but a constant supply of TBOEP would be necessary to get this steady state. Such a steady state concentration would be very individual and very difficult to determine. Therefore, the calculation of DI based on BBOEHEP is the most appropriate method and should reach the “real” value as close as possible.
Dust samples to calculate DI
As previously described the urinary samples were collected in day-care centers and in addition levels of different xenobiotics such as organophosphates were determined in collected dust samples for details see (Fromme et al. 2013, 2014). Therefore, it is possible to calculate the uptake of TBOEP within 8 h (length of stay of children in day-care centers). Based on a mean of 60 mg uptake of dust within 24 h a child ingested 20 mg within 8 h and in median 0.46 µg/kg b.w. of TBOEP would be ingested by a child (Table 5) (EPA 2011). This is in the same range as calculated via BBOEP but clearly higher as calculated based on BBOEHEP (Table 5). To best of our knowledge the assessment of the amount of ingested dust is the assessment of the US-EPA, but in the body of experts this assessment of 60 mg per day is critically discussed and many experts believe that the real value should be clearly lower. For example the calculation of dust intake for di-isononyl cyclohexane-1,2-dicarboxylate (DINCH®) results in an obvious overestimation of at least factor 2 of the intake (Fromme et al. 2016). Therefore, as discussed before the DI calculated from BBOEHEP should be the appropriate method up to now and, therefore, uptake of dust should be clearly lower.
In addition to dust ingestion an intake via air will also occur. As previously described by Fromme et al. for a child staying 6 h in a day-care center about 120 ng of TBOEP (2.5 m3 of air × 49 ng/m3) will be inhaled in median (Fromme et al. 2014). After adjustment to the body weight with at least 10 kg the DI may be only in the low ng/kg b.w. range.
The most significant route of exposure of the general population seems via ingestion of food or water (ATSDR 2012). An FDA total diet study reported results for 1986–1991 for several age groups (Gunderson 1995). Mean daily intakes for male and female ranging from 0.0009 to 0.004 µg/kg b.w. with the highest mean daily intake 0.005 µg/kg b.w. for 6–11 years old children. In comparison to the levels shown in Table 5 again the calculation of DI based on BBOEHEP is more realistic.
Only few human biomonitoring data for TBOEP metabolites are available. For a Norwegian mother–child cohort BBOEP was observed in 32% of urine samples of children and < 1% of the mothers (Cequier et al. 2015). Highest concentration was 1 µg/l in children and median below 0.18 µg/l (LOD). Van den Eede reported in different pooled urine samples the detection of BBOEP in about 6% of all pooled samples with a highest concentration of 0.53 µg/l (Van den Eede et al. 2015). A higher detection frequency of 90% was reported by Fromme et al. with highest concentration of 24.9 µg/l (median 2 µg/l) in urine samples of children (n = 312) of different day-care centers (Fromme et al. 2014). In contrast to Cequier et al., van den Eede et al. and the study presented here using LC–MS techniques Fromme et al. used a GC–MS/MS method after derivatization of the metabolites. This may partially explain the different results. Therefore, 20 of 54 urine samples presented here were also analysed by Fromme et al. In 19 of these samples Fromme et al. observed clearly higher levels (median 4.4 versus 0.19 µg/l) compared to the levels presented here. Up to now a conclusive explanation is not available but van den Eede wrote “no sensitive and selective MRM transitions were found on GC–MS/MS after derivatization” (Van den Eede et al. 2013b). A first test of the applied GC–MS/MS for BBOEP confirmed the results of van den Eede (data not shown).
Using the data of Fromme et al. for BBOEP and the F ue obtained in the described toxicokinetic study DI of 7.6 (median) and 40.7 µg/kg b.w. (95th percentile) were obtained but highest level of 24.9 µg/l would result in a DI of 94.7 µg/kg b.w.
This dose would exceed the current RfD of 50 µg/kg b.w. almost twofold but as discussed the GC–MS/MS method and BBOEP as biomarker are not very reliable and, therefore, further research on this topic will be necessary in future.
References
Ali N, Dirtu AC, Van den Eede N et al (2012a) Occurrence of alternative flame retardants in indoor dust from New Zealand: indoor sources and human exposure assessment. Chemosphere 88(11):1276–1282. doi:10.1016/j.chemosphere.2012.03.100
Ali N, Van den Eede N, Dirtu AC, Neels H, Covaci A (2012b) Assessment of human exposure to indoor organic contaminants via dust ingestion in Pakistan. Indoor Air 22(3):200–211. doi:10.1111/j.1600-0668.2011.00757.x
ATSDR (2012) Toxicological profile for phosphate ester flame retardants. In: U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES PHS, Agency for Toxic Substances and Disease Registry (ed). Agency for Toxic Substances and Disease Registry, Atlanta, pp 1–431. https://www.atsdr.cdc.gov/toxprofiles/tp202.pdf
Bergh C, Torgrip R, Emenius G, Ostman C (2011) Organophosphate and phthalate esters in air and settled dust—a multi-location indoor study. Indoor Air 21(1):67–76. doi:10.1111/j.1600-0668.2010.00684.x
Bicker W, Lammerhöfer M, Genser D, Kiss H, Lindner W (2005) A case study of acute human chlorpyrifos poisoning: novel aspects on metabolism and toxicokinetics derived from liquid chromatography-tandem mass spectrometry analysis of urine samples. Toxicol Lett 159(3):235–251. doi:10.1016/j.toxlet.2005.05.013
Brandsma SH, de Boer J, van Velzen MJ, Leonards PE (2014) Organophosphorus flame retardants (PFRs) and plasticizers in house and car dust and the influence of electronic equipment. Chemosphere 116:3–9. doi:10.1016/j.chemosphere.2014.02.036
Brommer S, Harrad S, Van den Eede N, Covaci A (2012) Concentrations of organophosphate esters and brominated flame retardants in German indoor dust samples. J Environ Monit 14(9):2482–2487. doi:10.1039/c2em30303e
Burka LT, Sanders JM, Herr DW, Matthews HB (1991) Metabolism of tris(2-chloroethyl) phosphate in rats and mice. Drug Metab Dispos 19(2):443–447
Cequier E, Ionas AC, Covaci A, Marce RM, Becher G, Thomsen C (2014) Occurrence of a broad range of legacy and emerging flame retardants in indoor environments in Norway. Environ Sci Technol 48(12):6827–6835. doi:10.1021/es500516u
Cequier E, Sakhi AK, Marce RM, Becher G, Thomsen C (2015) Human exposure pathways to organophosphate triesters—a biomonitoring study of mother-child pairs. Environ Int 75:159–165. doi:10.1016/j.envint.2014.11.009
Dodson RE, Perovich LJ, Covaci A et al (2012) After the PBDE phase-out: a broad suite of flame retardants in repeat house dust samples from California. Environ Sci Technol 46(24):13056–13066. doi:10.1021/es303879n
Egloff C, Crump D, Porter E et al (2014) Tris(2-butoxyethyl)phosphate and triethyl phosphate alter embryonic development, hepatic mRNA expression, thyroid hormone levels, and circulating bile acid concentrations in chicken embryos. Toxicol Appl Pharmacol 279(3):303–310. doi:10.1016/j.taap.2014.06.024
EPA US (2011) Exposure Factors Handbook U.S. Environmental Protection Agency, Washington, DC
Fromme H, Lahrz T, Kraft M et al (2013) Phthalates in German daycare centers: occurrence in air and dust and the excretion of their metabolites by children (LUPE 3). Environ Int 61:64–72. doi:10.1016/j.envint.2013.09.006
Fromme H, Lahrz T, Kraft M et al (2014) Organophosphate flame retardants and plasticizers in the air and dust in German daycare centers and human biomonitoring in visiting children (LUPE 3). Environ Int 71:158–163. doi:10.1016/j.envint.2014.06.016
Fromme H, Schütze A, Lahrz T et al (2016) Non-phthalate plasticizers in German daycare centers and human biomonitoring of DINCH metabolites in children attending the centers (LUPE 3). Int J Hyg Environ Health 219(1):33–39. doi:10.1016/j.ijheh.2015.08.002
Garcia M, Rodriguez I, Cela R (2007) Microwave-assisted extraction of organophosphate flame retardants and plasticizers from indoor dust samples. J Chromatogr A 1152(1–2):280–286. doi:10.1016/j.chroma.2006.11.046
Gunderson EL (1995) FDA Total Diet Study, July 1986–April 1991, dietary intakes of pesticides, selected elements, and other chemicals. J AOAC Int 78(6):1353–1363
Hartmann PC, Burgi D, Giger W (2004) Organophosphate flame retardants and plasticizers in indoor air. Chemosphere 57(8):781–787. doi:10.1016/j.chemosphere.2004.08.051
Jin Y, Chen G, Fu Z (2016) Effects of TBEP on the induction of oxidative stress and endocrine disruption in Tm3 Leydig cells. Environ Toxicol 31(10):1276–1286. doi:10.1002/tox.22137
Kessler W, Numtip W, Völkel W et al (2012) Kinetics of di(2-ethylhexyl) phthalate (DEHP) and mono(2-ethylhexyl) phthalate in blood and of DEHP metabolites in urine of male volunteers after single ingestion of ring-deuterated DEHP. Toxicol Appl Pharmacol 264(2):284–291. doi:10.1016/j.taap.2012.08.009
Kim JW, Isobe T, Muto M et al (2014) Organophosphorus flame retardants (PFRs) in human breast milk from several Asian countries. Chemosphere 116:91–97. doi:10.1016/j.chemosphere.2014.02.033
Kojima H, Takeuchi S, Itoh T, Iida M, Kobayashi S, Yoshida T (2013) In vitro endocrine disruption potential of organophosphate flame retardants via human nuclear receptors. Toxicology 314(1):76–83. doi:10.1016/j.tox.2013.09.004
Kurebayashi H, Tanaka A, Yamaha T (1985) Metabolism and disposition of the flame retardant plasticizer, tri-p-cresyl phosphate, in the rat. Toxicol Appl Pharmacol 77(3):395–404
Laham S, Long G, Schrader K, Szabo J (1984) Induction of electrophysiological and morphological changes in Sprague-Dawley rats fed tributoxyethyl phosphate. J Appl Toxicol 4(1):42–48
Laham S, Szabo J, Long G, Schrader K (1985) Dose-response toxicity studies on tributoxyethyl phosphate orally administered to Sprague-Dawley rats. Am Ind Hyg Assoc J 46(8):442–448. doi:10.1080/15298668591395139
Miller LA, Stapleton FB (1989) Urinary volume in children with urolithiasis. J Urol 141(4):918–920
Mittermeier A, Völkel W, Fromme H (2016) Kinetics of the phthalate metabolites mono-2-ethylhexyl phthalate (MEHP) and mono-n-butyl phthalate (MnBP) in male subjects after a single oral dose. Toxicol Lett 252:22–28. doi:10.1016/j.toxlet.2016.04.009
Möller A, Sturm R, Xie Z, Cai M, He J, Ebinghaus R (2012) Organophosphorus flame retardants and plasticizers in airborne particles over the Northern Pacific and Indian Ocean toward the Polar Regions: evidence for global occurrence. Environ Sci Technol 46(6):3127–3134. doi:10.1021/es204272v
Nishimaki-Mogami T, Minegishi K, Tanaka A, Sato M (1988) Isolation and identification of metabolites of 2-ethylhexyl diphenyl phosphate in rats. Arch Toxicol 61(4):259–264
Otake T, Yoshinaga J, Yanagisawa Y (2004) Exposure to phthalate esters from indoor environment. J Expo Anal Environ Epidemiol 14(7):524–528. doi:10.1038/sj.jea.7500352
Poma G, Glynn A, Malarvannan G, Covaci A, Darnerud PO (2017) Dietary intake of phosphorus flame retardants (PFRs) using Swedish food market basket estimations. Food Chem Toxicol 100:1–7. doi:10.1016/j.fct.2016.12.011
Reyna MS, Thake DG (1987) Eighteen week feeding study of tributoxyethyl phosphate (TBEP) administered to Sprague-Dawley rats. In: Laboratory MEH (ed) Submitted to the U.S. EPA under TSCA Section 8D. EPA Document No. 86-910000297; OTS0530087, St Louis
Saito I, Onuki A, Seto H (2007) Indoor organophosphate and polybrominated flame retardants in Tokyo. Indoor Air 17(1):28–36. doi:10.1111/j.1600-0668.2006.00442.x
Saitoh M, Umemura T, Kawasaki Y et al (1994) Subchronic toxicity study of tributoxyethyl phosphate in Wistar rats. Eisei Shikenjo Hokoku 112:27–39
Staaf T, Ostman C (2005) Organophosphate triesters in indoor environments. J Environ Monit 7(9):883–887. doi:10.1039/b506631j
Su G, Letcher RJ, Yu H, Gooden DM, Stapleton HM (2016) Determination of glucuronide conjugates of hydroxyl triphenyl phosphate (OH-TPHP) metabolites in human urine and its use as a biomarker of TPHP exposure. Chemosphere 149:314–319. doi:10.1016/j.chemosphere.2016.01.114
Sundkvist AM, Olofsson U, Haglund P (2010) Organophosphorus flame retardants and plasticizers in marine and fresh water biota and in human milk. J Environ Monit 12(4):943–951. doi:10.1039/b921910b
Suzuki T, Sasaki K, Takeda M, Uchiyama M (1984) Metabolism of tributyl phosphate in male rats. J Agric Food Chem 32(3):603–610
Tajima S, Araki A, Kawai T et al (2014) Detection and intake assessment of organophosphate flame retardants in house dust in Japanese dwellings. Sci Total Environ 478:190–199. doi:10.1016/j.scitotenv.2013.12.121
Van den Eede N, Dirtu AC, Neels H, Covaci A (2011) Analytical developments and preliminary assessment of human exposure to organophosphate flame retardants from indoor dust. Environ Int 37(2):454–461. doi:10.1016/j.envint.2010.11.010
Van den Eede N, Maho W, Erratico C, Neels H, Covaci A (2013a) First insights in the metabolism of phosphate flame retardants and plasticizers using human liver fractions. Toxicol Lett 223(1):9–15. doi:10.1016/j.toxlet.2013.08.012
Van den Eede N, Neels H, Jorens PG, Covaci A (2013b) Analysis of organophosphate flame retardant diester metabolites in human urine by liquid chromatography electrospray ionisation tandem mass spectrometry. J Chromatogr A 1303:48–53. doi:10.1016/j.chroma.2013.06.042
Van den Eede N, Heffernan AL, Aylward LL et al (2015) Age as a determinant of phosphate flame retardant exposure of the Australian population and identification of novel urinary PFR metabolites. Environ Int 74:1–8. doi:10.1016/j.envint.2014.09.005
Van der Veen I, de Boer J (2012) Phosphorus flame retardants: properties, production, environmental occurrence, toxicity and analysis. Chemosphere 88(10):1119–1153. doi:10.1016/j.chemosphere.2012.03.067
Völkel W, Kiranoglu M, Fromme H (2011) Determination of free and total bisphenol A in urine of infants. Environ Res 111(1):143–148. doi:10.1016/j.envres.2010.10.001
Völkel W, Kiranoglu M, Schuster R, Fromme H (2014) Phthalate intake by infants calculated from biomonitoring data. Toxicol Lett 225(2):222–229. doi:10.1016/j.toxlet.2013.12.012
Acknowledgements
The project was funded by a grant from the Bavarian State Ministry of the Environment and Public Health. The authors would like greatly thank all volunteers and the participating children, caregivers, and parents for their valuable support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Völkel, W., Fuchs, V., Wöckner, M. et al. Toxicokinetic of tris(2-butoxyethyl) phosphate (TBOEP) in humans following single oral administration. Arch Toxicol 92, 651–660 (2018). https://doi.org/10.1007/s00204-017-2078-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00204-017-2078-7