
Abstract
Introduction and hypothesis
The main objective of this study was to compare the effectiveness of pelvic floor muscle training, and vitamin D replacement in the treatment of urinary incontinence in the postpartum period of pregnant women with vitamin D deficiency.
Methods
The study was planned as an ancillary study of a study on the determination of the relationship between vitamin D deficiency and urinary incontinence in third-trimester pregnant women. Total 61 women who defined urinary incontinence at postpartum 8th week were included in the study. The participants were divided into two groups: the vitamin D replacement group and the pelvic floor muscle training (PFMT) group. Participants in both groups received appropriate treatment for 12 weeks. İnitial evaluations of which Pelvic Organ Prolapse-Quantification stage, International Consultation on Incontinence Modular Questionnaire on Female Lower Urinary Tract Symptoms (ICIQ-FLUTS) query, and pelvic floor muscle strength were repeated after 12 weeks of treatment for each patient.
Results
In the vitamin D replacement group, there was a significant increase in Oxford scores measured after treatment compared with pre-treatment and a significant decrease in ICIQ-FLUTS scores. In the comparison of the groups, it was determined that the changes in the Oxford and ICIQ-FLUTS scores of the vitamin D group after treatment were significantly higher than those of the PFMT group. In this pilot study, it was determined that the effectiveness of vitamin D replacement in the treatment of pelvic floor dysfunction in pregnant women with hypovitaminosis D was significantly higher than PFMT.
Conclusion
Vitamin D replacement may be useful in the treatment of urinary incontinence in pregnant women with hypovitaminosis D.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Urinary incontinence is a common health problem affecting 5–70% of the female population [1]. It has been reported that urinary incontinence complaints occur in 35–58% of women during pregnancy, especially during the third trimester. The most common types of incontinence during pregnancy are stress urinary incontinence (31–60%) and urge urinary incontinence (2–35%) [2–4].
Pregnancy and childbirth are among the most important risk factors for the development of urinary incontinence in women. Increased intra-abdominal pressure, hormonal changes, and changes in connective tissue during pregnancy may adversely affect pelvic floor muscle strength and sphincter functions [5–7].
Vitamin D receptors are found in various organs and tissues of the body. In addition to its essential role in the regulation of calcium metabolism, vitamin D also significantly affects pelvic floor muscle strength and functions and detrusor activity through its receptors in the pelvic floor muscles and bladder [8–12]. Various studies have reported that vitamin D deficiency also poses a risk for pelvic floor dysfunction, such as urinary incontinence and lower urinary tract symptoms. However, there is no complete consensus on this issue in the literature [12–16].
Although studies investigating the relationship between vitamin D status and pelvic floor dysfunction generally examine the perimenopausal female population, preliminary studies evaluating the relationship between urinary incontinence and vitamin D deficiency in pregnant women have been published recently [17–19]. Pelvic floor weakness due to decreased muscle strength, increased osmotic diuresis secondary to impaired calcium metabolism and increased detrusor irritability are the theories proposed in the literature to explain the relationship between vitamin D deficiency and UI. In a recently published meta-analysis, it was reported that vitamin D supplementation has positive effects in the treatment of lower urinary tract symptoms in the female population [20]. The aim of this study is to compare the effectiveness of pelvic floor muscle training, which is the standard initial treatment, and vitamin D replacement, which is not included in the standard treatment protocol, in the treatment of urinary incontinence in the postpartum period of pregnant women with vitamin D deficiency.
Materials and methods
Our study was planned as a continuation of the cross-sectional thesis study on the determination of the relationship between vitamin D deficiency and urinary incontinence in third-trimester pregnant women [21]. Serum 25(OH)D3 concentrations were measured by ELISA (Global Diagnostics & Medical Solutions KAP1971/GDMS, 13E27/2, Mortsel, Belgium ) in the third trimester of pregnancy. Serum 25(OH)D3 concentrations below 20 ng /ml were classified as a deficiency (intra-assay coefficient variability: 5.7%, interassay coefficient variability: 4.7%). In the study in question, 210 pregnant women who were found to have vitamin D deficiency and were older than 18 years of age, had no cognitive problems, had no gestational or pregestational diabetes or connective tissue diseases, had no previous history of pelvic floor dysfunction, and had a single pregnancy at 28 weeks of gestation and above, constituted the universe of our study. Our study was approved by the Katip Çelebi University Faculty of Medicine Local Ethics Committee (IRB 2021-43).
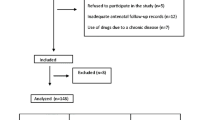
Eighty-nine of the cases (42.4%) who defined urinary incontinence were included in the present study. The patients included in the study were invited to the clinic at the end of the postpartum 8th week and their baseline evaluations were made. Eleven people who did not attend the first evaluation visit, 14 people who stated that they did not have urinary incontinence at the moment, and 3 people who had pelvic organ prolapse >stage 2 were excluded from the study (Fig. 1). Informed consent was obtained from the participants before the initial evaluation. In the baseline evaluation, all cases were evaluated by the same investigator (SA), and pelvic floor muscle strength measurement and POP-Q evaluation were performed. Three patients with stage 3 or higher pelvic organ prolapse were excluded from the study. Pelvic floor muscle strength was evaluated on a scale of 1–5 according to the Oxford scale. The Turkish version of the International Consultation on Incontinence Modular Questionnaire on Female Lower Urinary Tract Symptoms (ICIQ-FLUTS) questionnaire, to which Turkish validity and reliability was provided by Uğurlucan et al. [22] were applied to all participants. In this Questionnaire, the participants were asked a total of 12 questions about the frequency or severity of urinary incontinence and they were asked to score these questions between 0 and 4. The maximum score that the participants can get from this questionnaire form is 48. As the severity of incontinence increases, the ICIQ-FLUTS score increases.

Study population
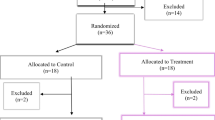
After this evaluation, the participants were divided into two groups according to the simple randomization method: the vitamin D replacement group and the Pelvic Floor Muscle Training (PFMT) group. A standard dose of 1200 IU daily vitamin D replacement was given to 31 subjects in the vitamin D replacement group for 12 weeks. Turkish Ministry of Health recommended 1200 units/day vitamin D replacement for pregnant women; thus, in our study we administered 1,200 units of vitamin D. On the other hand, 30 patients in the PFMT group underwent PFMT for 12 weeks, in a 20- to 30-min session per week, accompanied by a physiotherapist. PFMT sessions were planned to create contraction–relaxation sets of 5 min standing and 10 min lying down and not creating contractions in the abdominal wall muscles. Participants were asked to repeat these exercise sessions taught by the physiotherapist for at least 20 min each day. The compliance of the participants in the exercise program was checked by a physiotherapist at least once during the study using the telemedicine method. One patient from the vitamin D group and 2 patients from the PFMT group were excluded from the study owing to treatment incompatibility. All evaluations were repeated after 6 weeks of treatment. The data of 57 patients who completed the treatment process were evaluated.
The data were evaluated in the statistical package program IBM SPSS Statistics Standard Concurrent User V 26 (IBM, Armonk, NY, USA). Descriptive statistics were given as number of units (n), percentage (%), median, minimum, maximum, and interquartile range. The normal distribution of the data of numerical variables was evaluated with the Shapiro–Wilk test of normality. The Mann–Whitney U test was used for the comparison of Oxford and ICQ scores between groups, and the Wilcoxon test was used for within-group comparisons. Chi-squared test and Fisher's exact test were used for the comparison of POP-Q distributions according to the treatment applied, and McNemar–Bowker test was used for in-group comparisons. A p value of <0.05 was considered statistically significant.
Results
Vitamin D replacement (n=29) and PFMT (n=28) groups were found to be similar in terms of demographic data, mode of delivery, and birth weight (Table 1). Intragroup and intergroup comparisons were made for pelvic floor muscle strength and ICIQ-FLUTS scores before and after treatment in both groups. In intragroup evaluations, the increase in pelvic floor muscle strength values after treatment in the PFMT group was not statistically significant. Similarly, the decrease in the ICIQ-FLUTS score after treatment in the PFMT group was not significant. There was a statistically significant difference between the groups' pre-treatment Oxford scores (Table 2). Although it seems to be a negative situation in terms of comparison of treatment results, we thought that the lower average Oxford score of the vitamin D replacement group than the PFMD group will not have a negative effect on the evaluation of the success of vitamin D replacement treatment. In the vitamin D replacement group, there was a significant increase in Oxford scores measured after treatment compared with pre-treatment and a significant decrease in ICIQ-FLUTS scores (Table 2).
In the comparison between the groups, it was determined that the changes in the Oxford and ICIQ-FLUTS scores of the vitamin D group after treatment were significantly higher than those of the PFMT group (Table 2).
When the study groups were evaluated in terms of POP-Q stages, stage 1 POP was found in 10.3% of the cases in the vitamin D group and stage 2 POP in 6.9%. In the PFMT group, 7.1% of the cases had stage 1 POP. Stage 2 POP was not detected in this group. There was no significant difference between intra-group and intergroup comparisons before and after treatment in terms of pelvic organ prolapse degrees of the cases (Table 3).
Discussion
In the present study it was determined that those women who had vitamin D deficiency and urinary incontinence during the postpartum period had a significant improvement in pelvic floor muscle strength and incontinence-related quality of life scores with vitamin D replacement compared with PFMT.
There is a consensus in the literature on the negative effects of pregnancy and childbirth on pelvic floor muscle strength and lower urinary tract symptoms. It has been reported that the prevalence of UI increases, especially in the third trimester and this affects the quality of life significantly, whereas the prevalence decreases significantly (42% vs 6.8%) during the postpartum period [19]. It has been reported that in women with persistent urinary incontinence in the postpartum period, symptoms are particularly evident in the first 4–6 weeks, and then the frequency and severity of symptoms decrease over time [23, 24]. In the presented study, women who still had urinary incontinence at the 8th week postpartum were included in the study, thus minimizing the spontaneous regression effect of UI complaints.
It has been stated in the literature that PFMT is effective in increasing pelvic floor muscle strength [25, 26]. Many researchers have reported that PFMT during pregnancy has a preventive effect on the development of postpartum UI, and it is recommended in the guidelines that all pregnant women do PFMT [27, 28]. On the other hand, there is insufficient evidence for the effectiveness of PFMT in the treatment of UI, even under the control of a physiotherapist [29, 30]. In our study, it was determined that the increase in pelvic floor muscle strength and UI-related quality of life scores with PFMT applied from the postpartum 8th week was not statistically significant.
There is no consensus in the literature on the relationship between vitamin D status and urinary incontinence [31]. In preliminary studies examining the effectiveness of vitamin D replacement in the treatment of urinary incontinence, it has been reported that vitamin D supplementation was generally administered without knowing the vitamin D status of the participants [32]. It has been reported in some studies that vitamin D replacement has a protective effect regarding pelvic floor diseases and that the onset of overactive bladder symptoms is delayed in middle-aged and older women who take high-dose oral vitamin D [12, 33]. In a recent study, it was reported that vitamin D deficiency in mid-trimester pregnant women led to an increase in the frequency of stress incontinence [17]. To the best of our knowledge, the present study is the first to investigate the effectiveness of vitamin D replacement in pregnant women on pelvic floor dysfunction. The strengths of our study are that it was designed prospectively, that it was conducted on women with confirmed hypovitaminosis D and ongoing urinary incontinence. Despite the randomization, the vitamin D group had significantly lower pre-treatment Oxford scores, which may have allowed for a greater improvement after treatment. This situation, the cross-sectional nature, and the limited number of cases are the potential weaknesses of our study
Conclusions
In this pilot study, it was determined that the effectiveness of vitamin D replacement in the treatment of urinary incontinence in pregnant women with hypovitaminosis D was significantly greater than PFMT. During pregnancy, supplementation with vitamin D in addition to PFMT may be beneficial in preventing pelvic floor dysfunction. However, more studies are needed to evaluate the therapeutic efficacy of vitamin D replacement in the treatment of pelvic floor dysfunction in pregnant and puerperal women.
Abbreviations
- BMI:
-
Body Mass Index
- ICIQ-FLUTS:
-
The International Consultation on Incontinence Modular Questionnaire on Female Lower Urinary Tract Symptoms
- PFMT:
-
Pelvic Floor Muscle Training
- POP-Q:
-
Pelvic Organ Prolapse-Quantification
References
Milsom I, Altman D, Cartwright R, et al. Epidemiology of urinary incontinence (UI) and other lower urinary tract symptoms (LUTS), pelvic organ prolapse (POP) and anal (AI) incontinence. In: Abrams P, Cardozo L, Wagg A, Wein A, editors. Incontinence. 6th ed. Paris: Health Publications Ltd; 2016. p. 17–24.
Brown SJ, Donath S, MacArthur C, McDonald EA, Krastev AH. Urinary incontinence in nulliparous women before and during pregnancy: prevalence, incidence, and associated risk factors. Int Urogynecol J. 2010;21(2):193–202. https://doi.org/10.1007/s00192-009-1011-x.
Daly D, Clarke M, Begley C. Urinary incontinence in nulliparous women before and during pregnancy: prevalence, incidence, type, and risk factors. Int Urogynecol J. 2018;29(3):353–62. https://doi.org/10.1007/s00192-018-3554-1.
Wesnes SL, Rørtveit G, Bø K, Hunskaar S. Urinary incontinence during pregnancy. Obstet Gynecol. 2007;109(922):8.
Sangsawang B. Risk factors for the development of stress urinary incontinence during pregnancy in primigravidae: a review of the literature. Eur J Obstet Gynecol Reprod Biol. 2014;178:27–34. https://doi.org/10.1016/j.ejogrb.2014.04.010.
Mørkved S, Salvesen KA, Bø K, Eik-Nes S. Pelvic floor muscle strength and thickness in continent and incontinent nulliparous pregnant women. Int Urogynecol J Pelvic Floor Dysfunct. 2004;15(06):384–9, discussion 390. https://doi.org/10.1007/s00192-004-1194-0.
Tähtinen RM, Cartwright R, Tsui JF, Aaltonen RL, Aoki Y, Cárdenas JL, et al. Long-term impact of mode of delivery on stress urinary incontinence and urgency urinary incontinence: a systematic review and meta-analysis. Eur Urol. 2016;70(01):148–58. https://doi.org/10.1016/j.eururo.2016.01.037.
Bouillon R, Marcocci C, Carmeliet G, Bikle D, White JH, Dawson-Hughes B, et al. Skeletal and extraskeletal actions of vitamin D: current evidence and outstanding questions. Endocr Rev. 2019;40:1109–51.
Gunton JE, Girgis CM. Vitamin D and muscle. Bone Rep. 2018;8:163–7.
Ceglia L, Harris SS. Vitamin D and its role in skeletal muscle. Calcif Tissue Int. 2013;92:151–62.
Girgis CM, Mokbel N, Cha KM, Houweling PJ, Abboud M, Fraser DR, Mason RS, Clifton-Bligh RJ, Gunton JE. The vitamin D receptor (VDR) is expressed in skeletal muscle of male mice and modulates 25-hydroxyvitamin D (25OHD) uptake in myofibers. Endocrinology. 2014;155(9):3227–37. https://doi.org/10.1210/en.2014-1016.
Badalian SS, Rosenbaum PF. Vitamin D and pelvic floor disorders in women: results from the National Health and Nutrition Examination Survey. Obstet Gynecol. 2010;115(4):795–803. https://doi.org/10.1097/AOG.0b013e3181d34806.
Navaneethan PR, Kekre A, Jacob KS, Varghese L. Vitamin D deficiency in postmenopausal women with pelvic floor disorders. J Midlife Health. 2015;6:66–9.
Parker-Autry CY, Markland AD, Ballard AC, Downs-Gunn D, Richter HE. Vitamin D status in women with pelvic floor disorder symptoms. Int Urogynecol J. 2012;23:1699–705.
Aydogmus H, Demirdal US. Vitamin D deficiency and lower urinary tract symptoms in women. Eur J Obstet Gynecol Reprod Biol. 2018;228:48–52. https://doi.org/10.1016/j.ejogrb.2018.06.009.
Lee HS, Lee JH. Vitamin D and urinary incontinence among Korean women: a propensity score-matched analysis from the 2008–2009 Korean National health and nutrition examination survey. J Korean Med Sci. 2017;32:661–5.
Stafne SN, Mørkved S, Gustafsson MK, Syversen U, Stunes AK, Salvesen KA, et al. Vitamin D and stress urinary incontinence in pregnancy: a cross-sectional study. BJOG. 2020;127:1704–11.
Aydogmus S, Kelekci S, Aydogmus H, Demir M, Yilmaz B, Sutcu R. Association of antepartum vitamin D levels with postpartum pelvic floor muscle strength and symptoms. Int Urogynecol J. 2015;26:1179–84.
Rocha J, Brandão P, Melo A, Torres S, Mota L, Costa F. Avaliação da Incontinência Urinária na Gravidez e no Pós-Parto: Estudo Observacional [Assessment of urinary incontinence in pregnancy and postpartum: observational study]. Acta Med Port. 2017;30(7–8):568–72. Portuguese. https://doi.org/10.20344/amp.7371.
Yuan P, Wang T, Li H, Lan R, Li M, Liu J. Systematic review and meta-analysis of the association between vitamin D status and lower urinary tract symptoms. J Urol. 2021;205:1584–94.
Gul, S. To investigate the relationship between vitamin D deficiency and urinary incontinence in third trimester pregnant women. CoHe/Thesis Center Home. Thesis number: 2022-712896 via. https://tez.yok.gov.tr
Gungor Uğurlucan F, Yasa C, Yuksel Ozgor B, Ayvacikli G, Gunaydin C, Balci BK, Yalcin O. Validation of the Turkish version of the ICIQ-FLUTS, ICIQ-FLUTS long-form, ICIQ-LUTS quality-of-life, and ICIQ-FLUTS sexual functions. Neurourol Urodyn. 2020;39(3):962–968. https://doi.org/10.1002/nau.24302
Tanawattanacharoen S, Thongtawee S. Prevalence of urinary incontinence during the late third trimester and three months postpartum period in King Chulalongkorn Memorial Hospital. J Med Assoc Thai. 2013;96:144–9.
Zhu L, Li L, Lang JH, Xu T. Prevalence and risk factors for peri- and postpartum urinary incontinence in primiparous women in China: a prospective longitudinal study. Int Urogynecol J. 2012;23:563–72.
Mushtaq S, Ahmed A. Effectiveness of pelvic floor muscle training versus Pfilates exercise program to treat stress urinary incontinence in females: a randomized control trial. Isra Med J. 2019;11((4)-Part B):281–5.
Dumoulin C, Hay SJ, Habeé-Seguin GM, Mercier J. Pelvic floor muscle training versus no treatment, or in active control treatments, for urinary incontinence in women. Cochrane Database Syst Rev. 2014;1:CD005654.
NICE. Antenatal care for uncomplicated pregnancies. Clinical guideline [CG 62] London, UK; 2017. Available at: https://www.nice.org.uk/guidance/cg62.
Fritel X, Fauconnier A, Bader G, Cosson M, Debodinance P, Deffieux X, et al. Diagnosis and management of adult female stress urinary incontinence: guidelines for clinical practice from the French College of Gynaecologists and Obstetricians. Eur J Obstet Gynecol Biol Reprod. 2010;151:14–9.
Woodley SJ, Lawrenson P, Boyle R, Cody JD, Mørkved S, Kernohan A, et al. Pelvic floor muscle training for preventing and treating urinary and faecal incontinence in antenatal and postnatal women. Cochrane Database Syst Rev 2020;(5): CD007471. https://doi.org/10.1002/14651858.CD007471.pub4.
Fritel X, de Tayrac R, Bader G, Savary D, Gueye A, Deffieux X, et al. Preventing urinary incontinence with supervised prenatal pelvic floor exercises. Obstet Gynecol. 2015;126(2):370–7. https://doi.org/10.1097/AOG.0000000000000972.
Markland AD, Vaughan C, Huang A, et al. Effect of vitamin D supplementation on urinary incontinence in older women: ancillary findings from a randomized trial. Am J Obstet Gynecol. 2022;226(535):e1–12.
Vaughan CP, Markland AD, Huang AJ, Tangpricha V, Grodstein F. Vitamin D intake and progression of urinary incontinence in women. Urology. 2021;150:213–8. https://doi.org/10.1016/j.urology.2020.04.090.
Kilic MK, Kizilarslanoglu MC, Kara O, Arik G, Varan HD, Kuyumcu ME, et al. Hypovitaminosis D is an independent associated factor of overactive bladder in older adults. Arch Gerontol Geriatr. 2016;65:128–32. https://doi.org/10.1016/j.archger.2016.03.019.
Funding
This study was funded by the Board of Izmir Katip Celebi University Scientific Research Projects (2020-TDU-TIPF-0020).
Author information
Authors and Affiliations
Contributions
S Aydogmus: Project development, Critical revisions to the paper,
S Gul, Gizen Naz Kahraman: Data collection
H Aydogmus,: Manuscript writing
A. Yilmaz: Manuscript writing
Corresponding author
Ethics declarations
Conflicts of interest
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Aydogmus, S., Aydogmus, H., Gul, S. et al. Is vitamin D replacement effective in the treatment of postpartum urinary incontinence?. Int Urogynecol J 34, 1103–1108 (2023). https://doi.org/10.1007/s00192-022-05446-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-022-05446-5