
Abstract
Introduction
Surgical options for uterovaginal prolapse can be categorized into uterus conservation—e.g., laparoscopic sacrohysteropexy (LSHP) or vaginal hysterectomy (VH). There is insufficient reliable information on long-term comparative outcomes of these procedures. The primary aim of this study was to compare subjective and objective outcomes of LSHP and VH. The secondary aim was to record adverse events, recurrent prolapse, and new-onset stress urinary incontinence (SUI) up to 2 years.
Methods
Women with symptomatic uterovaginal prolapse who opted for either LSHP or VH were included. Subjective outcomes were compared at 1 and 2 years from baseline using the validated questionnaires. Objective/anatomical outcomes using the Pelvic Organ Prolapse Quantification (POP-Q) system were assessed before and at 3 months after surgery. Adverse events, recurrent prolapse, and new-onset SUI was recorded up to 2 years.
Results
The study assessed 226 women with uterovaginal prolapse; 125 opted for surgery (44 LSHP, 81 VH). There was no statistically significant difference in symptom domains between groups at baseline and 1 and 2 years. At 3 months POP-Q, greater improvement was seen in points Ba and Ap in the LSHP group compared to VH group and smaller genital hiatus was seen in the VH group. Adverse events, recurrent prolapse, or new-onset SUI were not significantly different in the two groups.
Conclusions
Both LSHP and VH are effective surgical options for uterovaginal prolapse. At 2 years, both procedures had similar improvement in symptom domains, overall scores, adverse events, recurrent prolapse, and new-onset SUI. Long-term randomized studies are needed.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Pelvic organ prolapse (POP) is a common condition in parous women that can become particularly significant with advancing age [1]. As life expectancy increases, this condition is acquiring greater significance. POP adversely impacts on a woman’s quality of life (QOL) [2]. Women with symptomatic POP after undergoing pelvic floor muscle exercise training choose between surgery and a vaginal pessary [3]. Approximately one in ten women opt to have POP surgery in their lifetime [1]. The recurrence of POP symptoms is common following POP surgery [3]; 30% of women who chose surgical option for POP symptoms undergo another POP operation either of the same or a different compartment [1].
Surgical treatment options for uterovaginal prolapse include removal or conservation of the uterus. There are various surgical approaches to both options, including vaginal, laparoscopic, robotic laparoscopic, and open abdominal [4]. There is a dearth of reliable information on the comparative outcomes of various surgical treatments for the uterovaginal prolapse relating to bladder, bowel, sexual function, and impact on QOL, all of which often occur in association with POP. Variations in approaches and techniques used and reported outcome measures in some previous studies preclude drawing helpful conclusions.
This prospective observational study aimed to compare subjective outcomes in women undergoing laparoscopic sacrohysteropexy (LSHP) or vaginal hysterectomy (VH) for symptomatic uterovaginal prolapse at baseline and 1 and 2 years following surgery using the validated International Consultation on Incontinence Questionnaire—Vaginal Symptoms (ICIQ-VS) [5] and the International Consultation on Incontinence Questionnaire—Urinary incontinence (ICIQ-UI) Short Form (SF) [6]. We also aimed to compare objective/anatomical outcomes at baseline and 3 months using the Pelvic Organ Prolapse Quantification (POP-Q) system. We also aimed to record adverse events (AE) and the need for surgery for recurrent POP (same/different compartment) or for new-onset stress urinary incontinence (SUI) up to 2 years.
Materials and methods
Between October 2012 and October 2013, 226 women with symptomatic uterovaginal prolapse referred to a gynecology or subspecialist urogynecology clinic at Royal Cornwall Hospital (after having received pelvic floor physiotherapy) were assessed. A detailed urogynaecology history was taken by a registrar or consultant gynecologist/subspecialist urogynecologist regarding symptoms of POP, urinary, bowel, and sexual dysfunction. Demographic data collected were age, parity, and body mass index (BMI). Note was made of previous POP or urinary incontinence (UI) surgery, medical comorbidities, hormone replacement therapy, constipation, chronic cough, and smoking status. Patients underwent an examination for staging by a skilled gynecologist using the standardized and validated International Continence Society (ICS) POP-Q [7]. Since POP is a clinical diagnosis, paraclinical tools such as pelvic floor imaging or cytological examination were not performed..
All women with symptomatic uterovaginal prolapse stage ≥2 were offered a choice of pessary or surgery. Exclusion criteria were desire for future pregnancy, abnormal uterine bleeding, abnormal cervical smear test result, concomitant and bothersome SUI, and other medical problems contraindicating general anesthesia or surgery. Women who opted for surgery and were eligible for both surgical treatment options (LSHP or VH) were evaluated. Women were given information (verbal and written) about the procedures and their benefits and risks and consented for concomitant vaginal pelvic floor repair, if needed. This information is detailed in our local trust-approved patient information leaflet. These options were uterus removal group (vaginal hysterectomy with vault suspension technique using sutures) and uterus preservation [laparoscopic suspension (sacrohysteropexy) with mesh].
These surgical options are included in the British Society of Urogynaecology (BSUG) national registry.
Women who needed more time to decide were allowed to do so. All women signed a consent form for the procedure and completed the ICIQ-VS and ICIQ-UI (SF) prior to surgery. Vaginal estrogens were only prescribed if there was evidence of vaginal atrophy. All women gave written consent for data use. This observational study was reviewed by the local Research and Development Department at The Royal Cornwall Hospital, and ethical/institutional review board approval was deemed unnecessary.
Surgery was performed under general anesthesia. For LSHP, we used type 1 macroporous, monofilament, nonabsorbable polypropylene mesh (PROLENE, Ethicon). The mesh is shaped to create two arms and a tail. After creating a pneumoperitoneum, four laparoscopic ports were introduced, and the peritoneum was opened over the sacral promontory and right pelvic sidewall down to the uterosacrals. Windows were created in the broad ligament on both sides. The arms of the mesh were introduced through the broad ligament windows and sutured anterior to the cervix using Ethibond™ 2/0 (Ethicon). The tail of the mesh was attached to the sacral promontory using a Protack™ 5-mm helical fastener (Covidien™ USA). The mesh was completely covered with theperitoneum. This technique is described by the Oxford Group [8,9,10,11].
For VH, the vault support was performed by suturing the exteriorized uterosacral ligaments to the vaginal vault [12]. Additional vault support was performed using the McCall technique whereby plication of uterosacral ligaments in the midline is achieved by incorporating the cul-de-sac peritoneum and posterior vaginal cuff. This obliterates the peritoneum of the posterior cul-de-sac and elevates the vault toward the plicated uterosacral ligaments [13, 14]. Both vault suspension techniques were performed using Vicryl 1 reabsorbable sutures (Ethicon).
Subjective outcomes at 1 and 2 years were assessed using the ICIQ-VS and ICIQ-UI (SF) questionnaires. The urogynecology nurse specialist mailed questionnaires to participants at 1 and 2 years postoperatively with a stamped, self-addressed return envelope. Results were compared with pretreatment baseline questionnaires. A reminder ICIQ-VS and ICIQ-UI (SF) was sent 2–3 months later to those who failed to respond. A record of the procedure was kept on the BSUG national registry. It is routine practice in our unit to invite these women for 3-month outpatient follow-up where a POP-Q is performed for objective/anatomical outcomes. We recorded concomitant POP surgery of other compartments (anterior and/or posterior colporrhaphy and/or enterocele repair with or without use of vaginal mesh (we use only biological mesh for vaginal pelvic floor surgery). Intraoperative and up to 3 months postoperative AE are recorded on the BSUG, which is routine practice. Moreover, notes were reviewed at 2 years to record procedure-related AE, such as mesh complications. Other outcomes were repeat POP surgery and/or SUI requiring surgical intervention within the 2-year postoperative period.
Statistical analysis
Two-tailed Mann–Witney U test/Wilcoxon signed-rank test were used for unpaired/paired data comparisons, respectively. Mann–Whitney U test was used to compare the difference between LSHP and VH groups, and Wilcoxon signed-rank test compared the difference in the same group at 1 and 2 years from baseline. For binary outcomes, two-tailed sign test/Fisher exact test for paired/unpaired data, respectively were used. P value <0.05 was taken as statistically significant.
Results
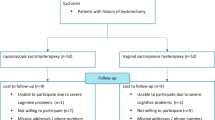
A total of 226 women were seen with symptomatic stage ≥2 uterovaginal prolapse during the study period. One hundred and thirty-one women opted for surgery for uterovaginal prolapse. We excluded six women from VH group (two deceased after 1-year follow-up; four needed concomitant SUI surgery). Therefore, 125 women were included for analysis (44 LSHP; 81 VH). All women completed a preoperative and 1-year ICIQ-VS and ICIQ-UI (SF) for surgical patients; 63/125 women (50%) completed the 2-year ICIQ-VS and ICIQ-UI (SF), 16 LSHP and 47 VH. Details of participants and questionnaire return are given in Fig. 1. Mean time interval for questionnaire response between baseline and the 1- and 2-year responses were 13 [standard deviation (SD) 3.2] and 25 (SD 5.9) months, respectively.

Study design
Women undergoing VH were older than those having a LSHP (p = 0.01). There was no statistically significant difference between groups with regard to BMI, previous urogynecology procedures, or parity (Table 1). Further details of baseline characteristics and previous urogynecological surgery are given in Table 1. There was no statistically significant difference in stage of anterior and middle compartment prolapse between groups; however, significantly more women in the VH group had posterior compartment prolapse (p = 0.00) preoperatively. Compared with the LSHP group, more women in the VH group underwent concomitant anterior and posterior repair (85% and 31%, respectively, in the VH group vs 0% and 9% in the LSHP group; p = 0.00).
Subjective outcomes of vaginal, urinary, fecal, sexual, and QOL symptoms
There were more sexually active women in the LSHP group: 21/44 (48%), 20/44 (45%), and 6/16 (38%) at baseline and 1 and 2 years, respectively, compared with 32/81 (40%), 27/81 (33%), and 16/49 (33%), respectively, in the VH group (Table 2).
At baseline, there was no difference between groups in vaginal, sexual, bowel, and urinary domains and overall sores in both groups (Tables 2 and 3). The symptom of tight vagina was reported as more bothersome in the VH group.
At 1 year compared with baseline, there was a statistically significant improvement in all vaginal domains in both groups. The exception was the lack of change in tight vagina symptom in the LSHP group. We found that the improvement noted in bowel symptoms at 1 year in both groups was sustained in the VH group at 2 years, but this was not so in the LSHP group. However, this difference between groups was not statistically significant (Table 2). All urinary domains showed a statistically significant improvement in the VH group. Overall, vaginal, QOL, and urinary scores improved in both groups. Sexual symptoms and their bothersomeness showed a statistically significant improvement in the LSHP group. There was no statistically significant difference in any of the sexual symptoms in the VH group at 1 year compared with baseline. The overall sexual score did not show statistically significant difference in either group.
At 2 years compared with baseline, in the VH group, symptoms of reduced sensation, tight vagina, amount of urine leak, and sexual domains did not demonstrate a statistically significant change, which was not significantly bothersome for those women. The other vaginal, urinary, and bowel symptoms improved, and overall vaginal and urinary symptom scores improved at 2 years compared with the baseline. In LSHP group, symptom of vaginal soreness, reduced sensation, loose vagina, tight vagina, bowel, urinary, and sexual domains showed no statistically significant change compared with baseline. However, it is interesting to note that this lack of symptom improvement was not bothersome. Overall vaginal scores also continued to demonstrate improvement in the LSHP group at 2 years compared with baseline. There was no difference between groups at 2 years compared with baseline in all symptom domains and overall scores.
Objective/anatomical outcomes using the POP-Q
Table 4 demonstrates greater improvement in points Ba and Ap in the LSHP group at 3 months compared with the VH group; it also shows the smaller genital hiatus in the VH group at 3 months compared with the LSHP group. There was no statistically significant difference in point C between groups (P = 0.06).
Adverse events in the two groups within 2 years from surgery
The LSHP group had two readmissions, one at day 5 with port-site hematoma and the other with urinary tract infection (UTI), and two bowel serosal injuries identified and sutured intraoperatively. There were no mesh--related AE during the study period. In the VH group, there were two bladder injuries repaired intraoperatively and one readmission with UTI at 2 weeks postoperatively. The difference in AE between groups was not statistically significant.
New-onset SUI and recurrent prolapse within 2 years from surgery
Three of 44 (7%) women in the LSHP group had new-onset bothersome SUI within 3 months and required a midurethral tape (tension-free vaginal tape) procedure, compared with none of the 81 women (0%) in the VH group. Within 2 years of surgery, two women in VH group (2.4%) underwent posterior repair, and one woman (1.2%) had a sacrocolpopexy. In the LSHP group, two women had symptomatic prolapse (4.5%): one a stage 2 rectocele and another a stage 2 cystocele and stage 2 rectocele. However, both women opted for vaginal support pessary management. The difference in new-onset prolapse (p = 0.84) and UI (P = 0.08) between groups within 2 years from surgery was not statistically significant.
Discussion
In this prospective study, we found no difference between LSHP and VH groups at 2 years compared with baseline in all symptom domains and their overall scores. All women presenting with symptomatic POP were offered treatment with a vaginal pessary or surgery, in line with the current evidence and recommendations based on expert opinion [15,16,17,18,19,20]. Selection bias was reduced by offering all women the same information on available surgical options. We routinely provide women an information leaflet that details all surgical treatment options for POP as well as separate specific information leaflets (LSHP and VH). We had no difficulty recruiting the VH. This is contrary to the experience reported in a randomized study by Rahmanou et al. [8] that struggled to recruit for a VH group. Compared with our results, more women in their study underwent concomitant vaginal pelvic floor repair in both the VH (98%) and LSHP (82%) group [8].
We found that neither surgical group needed significant numbers of subsequent pelvic floor surgery within the 2-year follow-up period. In other studies, more apical surgery was required in the VH group compared with the uterine suspension group (14% vs 6%), and more repeat vaginal repairs were required following hysteropexy (10–17%) [8, 10, 21]. This was seen favorably in our study, where only one of 81 (1.23%) women who underwent VH needed repeat apical surgery (sacrocolpopexy) within the 2-year follow-up time period. In our study all VH were performed by one surgeon and all LSHP by the other, both of whom are expert in their technique. This helped reduce the bias of operator performance. Similar results showing a low reoperation rate were shown in a retrospective study of reconstructive vaginal surgery for advanced POP at 86 months comparing hysterectomy versus sacrospinous hysteropexy [22].
We used two questionnaires—the ICIQ-VS [5] and the ICIQ-UI (SF) [7]—to assess all pelvic floor dysfunction symptoms (vaginal, bowel, sexual, urinary, and QOL). The ICIQ-VS is a simple, robust, fully validated tool that allows the assessment of vaginal, bowel, and sexual symptoms and their impact on QOL [5]. The ICIQ-VS assesses vaginal symptoms (awareness of dragging pain, vaginal soreness, reduced vaginal sensation, vaginal laxity, lump/bulge coming down the vagina, vaginal lump felt or seen, vaginal dryness, vaginal digitation to evacuate bowels, tight vagina, interference of vaginal symptoms with sexual life, and relationship with partner) and the bother of each of these symptoms and interference with everyday life. We also included the final shortened version of the ICIQ-UI (SF), which has high levels of validity, sensitivity, and reliability and provides a simple and robust measure to evaluate urinary symptoms and their impact on QOL [6].
We found a significant improvement in all vaginal symptoms at 1 and 2 years in both the LSHP and VH groups, except for tight vagina and the bothersomeness of loose vagina symptoms in the LSHP group. This might be explained by expectations from the procedure in younger age LSHP women. Moreover, LSHP would not lead to vaginal epithelial scar tissue, which can create an effect of tight vagina in the VH group. However, there was not a statistically significant difference between groups. Our findings of improvement in both groups are in agreement with other studies assessing surgical treatment of female POP [19, 22, 23]. However, these studies compared surgical to nonsurgical treatment options of any compartment prolapse and had a shorter follow-up than our study. Abdool et al. [19] reported statistically significant improvement at 1 year in prolapse, urinary, bowel, and sexual function in pessary users (n = 359) and those who chose surgery (n = 195) using the validated Sheffield POP questionnaire. Lo et al. [22] demonstrated that in 146 women (120 in the hysterectomy group and 26 in the hysteropexy group), no difference was seen in the adjusted objective and subjective success rates and sexual function between sacrospinous hysteropexy and hysterectomy. However, the hysterectomy group had fewer bothersome symptoms of prolapse. Two hundred and eighty-seven women with symptomatic POP were recruited for treatment with either pessary use or surgery. Improvement in vaginal, bowel, urinary, and QOL scores was reported using the same validated questionnaires we used in our study at 1 year after treatment. No statistically significant difference was noted between groups [23]. In a recent Cochrane review on surgery for apical prolapse [24], six studies (n = 667) were included to review vaginal hysterectomy versus alternatives for uterine prolapse. Though one randomized controlled trial found that awareness of POP was less likely after hysterectomy than after abdominal sacrohysteropexy [relative risk (RR) 0.38, 95% confidene interval (CI) 0.15–0.98, n = 84, moderate-quality evidence) [24]. However, no clear conclusions could be reached from the available evidence.
In accordance with our study, other studies have reported improvement in bowel-emptying symptoms with surgical correction of POP [19, 22, 23]. These studies had maximum follow-up of 1 year compared with our study of 2 years. Dietz et al. demonstrated no differences in functional outcomes or QOL at 12 months follow-up in women who underwent sacrospinous hysteropexy or VH for uterovaginal prolapse [21].
The belief that sexual function may be negatively affected after hysterectomy has not been supported in the literature to date. Weber et al. reported high degrees of satisfaction and no consistent changes in urinary, lower gastrointestinal, or sexual function after abdominal hysterectomy for benign gynecologic conditions in 43 women [25]. We found a significant improvement in the bothersomeness of interference with sex life and relationship with the partner due to vaginal symptoms in the LSHP group at 1 year; however, there was no statistically significant difference between groups. There was no further improvement noted at 2 years. This may be explained by expectations of ongoing improvement in sexual function in women opting for surgical treatment of POP. Since ours is the only study evaluating symptoms at 2 years using validated questionnaires, it would be of interest to assess longer-term change in pelvic floor symptoms in randomized studies.
Improvement in urinary domains in the VH group can be explained by more concomitant anterior compartment repairs in the VH group (Table 1), which may have contributed to improvement in urinary symptoms in the VH group. Other studies have reported improvement in urinary symptoms [19, 22, 23], which is in agreement with our results. Improved urinary symptoms in the postoperative period are also reported in a randomized prospective study of sacrospinous hysteropexy and vaginal hysterectomy [21].
There was no statistically significant difference between groups in terms of intraoperative AE and AE up to 2 years. Similar results are reported by Rahmanou et al. at 1-year follow-up for both groups [8].
In our study, three women in the LSHP group underwent midurethral surgery for SUI versus none in the VH group. This may be explained by the exclusion of women in the VH group who underwent concomitant SUI surgery. Moreover, more women in the VH underwent concomitant anterior repair, which may also have contributed to these results. Some studies also demonstrated that SUI (6–12%) after vaginal POP repair is likely to be secondary to the straightening/correction or overcorrection of the vesicourethral angle [26,27,28,29,30], which may explain the post-LSHP SUI findings. Our study did not demonstrate a difference in number of vaginal repairs for recurrent POP in either group; Rahmanou et al. [8], however, demonstrated more subsequent vaginal repairs following LSHP. This may again be explained by more concomitant anterior and posterior repairs in the VH group in our study, thereby requiring fewer pelvic floor repairs postoperatively.
On POP-Q assessment at 3 months’ follow-up, we found no statistically significant difference between groups in terms of improvement in point C, contrary to other studies [8, 10]. The likely explanation for is the lack of bias associated with variable surgical techniques, as one surgeon performed all VH and the other all LSHP. The finding of statistically significant improvement in points Ba and Ap in the LSHP group can be explained by elevation of these POP-Q points during the LSHP procedure. A smaller genital hiatus in the VH group can be explained by reduced distension effect after VH, as these women also had multicompartment prolapse adding to the distension and therefore increased preoperative genital hiatus, which reduced after VH.
Strengths
External validity of this study was enhanced by the use of fully validated assessment tools, attempts to reduce selection bias, and eliminating performance bias by one surgeon performing all VH and the other performing all LSHP. We are not aware of another prospective study that has evaluated the comparative subjective outcomes of LSHP and VH using the validated ICIQ-VS and ICIQ-UI (SF) questionnaires at 2 years. We used the two questionnaires to assess all pelvic floor dysfunction symptoms, which add to the strength of our study. We offered women information on all surgical options available, and the women chose the surgical option (LSHP vs VH), thereby reducing selection bias.
Limitations
Ours is not a randomized controlled trial. We did not exclude women with concomitant-compartment POP; therefore, women in the VH group underwent more concomitant anterior and posterior compartment prolapse. We acknowledge limitations in the generalizability of these results, as it is a single-center study, with one surgeon performing one type of operation and a second surgeon the other type. Bias of surgeon in prefering a particular technique could not be excluded. However, both surgeons are experts in their particular field and were consistently employing fully validated surgical techniques. Women in our study did not undergo a POP-Q at 1 and 2 years after prolapse operation, as it is not routine practice in the National Health Service to invite patients for clinical examination and long-term follow-up due to financial constraints. A multicenter, randomized, controlled study with long-term follow-up, yearly POP-Q evaluation, and subjective questionnaire assessments may be topics for future evaluation.
Conclusions
This study highlights that both LSHP and VH are effective surgical treatment options for managing uterovaginal prolapse. At 2 years, there was no significant difference between the two procedures in terms of symptom domains, overall scores, AE, recurrent prolapse, or new-onset SUI. Long=term data from randomized controlled studies is needed.
Abbreviations
- BSUG:
-
British Society of Urogynaecology
- ICIQ-UI (SF):
-
International Consultation on Incontinence Questionnaire—Urinary Incontinence Short Form
- ICIQ-VS:
-
International Consultation on Incontinence Questionnaire—Vaginal Symptoms
- LSHP:
-
Laparoscopic sacrohysteropexy
- POP:
-
Pelvic organ prolapse
- POP-Q:
-
Pelvic Organ Prolapse Quantification
- QOL:
-
Quality of life
- SUI:
-
Stress urinary incontinence
- VH:
-
Vaginal hysterectomy
References
Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol. 1997;89:501–6.
Digesu GA, Chaliha C, Salvatore S, Hutchings A, Khullar V. The relationship of vaginal prolapse severity to symptoms and quality of life. BJOG. 2005;112:971–6.
Dallenbach P, Kaelin-Gambirasio I, Jacob S, Dubuisson JB, Boulvain M. Incidence rate and risk factors for vaginal vault prolapse repair after hysterectomy. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19(12):1623–9.
Zucchi A, Lazzeri M, Porena M, Mearini L, Costantini E. Uterus preservation in pelvic organ prolapse surgery. Nat Rev Urol. 2010;7(11):626–33.
Price N, Jackson SR, Avery K, Brookes ST, Abrams P. Development and psychometric evaluation of the ICIQ vaginal symptoms questionnaire: the ICIQ-VS. BJOG. 2006;113(6):700–12.
Avery K, Donovan J, Peters T, Shaw C, Gotoh M, Abrams P. ICIQ: a brief and robust measure for evaluating the symptoms and impact of urinary incontinence. Neurourol Urodyn. 2004;23(4):322–30.
Bump RC, Mattiasson A, Bo K, Brubaker LP, DeLancey JO, Klarskov P, et al. The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. Am J Obstet Gynecol. 1996;175(1):10–7.
Rahmanou P, Price N, Jackson SR. Laparoscopic hysteropexy versus vaginal hysterectomy for the treatment of uterovaginal prolapse: aprospective randomized pilot study. Int Urogynecol J. 2015;26:1687–94.
Rahmanou P, Price N, Jackson SR. Laparoscopic hysteropexy: a novel technique for uterine preservation surgery. Int Urogynecol J. 2014;25(1):139–40.
Rahmanou P, White B, Price N, Jackson SR. Laparoscopic hysteropexy: 1- to 4-year follow-up of women postoperatively. Int Urogynecol J. 2014;25(1):131–8.
Price N, Slack A, Jackson SR. Laparoscopic hysteropexy: the initial results of a uterine suspension procedure for uterovaginal prolapse. BJOG Int J Obstet Gynaecol. 2010;117(1):62–6813.
Jha S, Moran P. The UK national prolapse survey: 5 years on. Int Urogynecol J. 2011;22(5):517–28.
McCall ML. Posterior culdeplasty; surgical correction of enterocele during 395 vaginal hysterectomies; a preliminary report. Obstet Gynecol. 1957;10:595–602.
RCOG. Green-top guideline no. 46: the management of posthysterectomy vaginal vault prolapse. 2007. http://www.rcog.org.uk/en/guidelines-research-services/guidelines/gtg46
Adams EJ, Thomson AJM, Maher C, Hagen S. Mechanical devices for pelvic organ prolapse in women. Cochrane Database Syst Rev. 2004;(2):CD004010. doi:10.1002/14651858.CD004010.pub2.
Maher C, Baessler K, Glazener CMA, Adams EJ, Hagen S. Surgical management of pelvic organ prolapse in women. Cochrane Database Syst Rev. 2007 (3):CD004014. doi:10.1002/14651858
Thakar R, Stanton S. Management of genital prolapse. BMJ. 2002;324(7348):1258–62.
Kapoor DS, Thakar R, Sultan AH, Oliver R. Conservative versus surgical management of prolapse: what dictates patient choice? Int Urogynecol J Pelvic Floor Dycfunct. 2009;20(10):1157–61.
Abdool Z, Thakar R, Sultan AH, Oliver R. Prospective evaluation of outcome of vaginal pessaries versus surgery in women with symptomatic pelvic organ prolapse. Int Urogynecol J. 2011;22:273–8.
Lone FW, Thakar R, Sultan AH, Karamalis G. A 5-year prospective study of vaginal pessary use for pelvic organ prolapse. Int J Gynecol Obstet. 2011;114:56–9.
Dietz V, Van der Vaart CH, Van der Graaf Y, Heintz P, Schraffordt Koops SE. One-year follow-up after sacrospinous hysteropexy and vaginal hysterectomy for uterine descent: a randomized study. Int Urogynecol J. 2010;21(2):209–16.
Lo TS, Pue LB, Hung TH, Wu PY, Tan YL. Long-term outcome of native tissue reconstructive vaginal surgery for advanced pelvic organ prolapse at 86 months: hysterectomy versus hysteropexy. J Obstet Gynaecol Res. 2015;41(7):1099–107.
Lone FW, Thakar R, Sultan AH. One-year prospective comparison of vaginal pessaries and surgery for pelvic organ prolapse using the validated ICIQ-VS and ICIQ-UI (SF) questionnaires. Int Urogynecol J. 2015;26(9):1305–12.
Maher C, Feiner B, Baessler K, Christmann-Schmid C, Haya N, Brown J (2016) Surgery for women with apical vaginal prolapse. Cochrane Database Syst Rev. 2016;(10): CD012376. doi:10.1002/14651858.CD012376.
Weber AM, Walters MD, Schover LR, Church JM, Piedmonte MR. Functional outcomes and satisfaction after abdominal hysterectomy. Obstet Gynecol. 1999;181(3):530–5.
Benson JT, Lucente V, McClellan E. Vaginal versus abdominal reconstructive surgery for the treatment of pelvic support defects: a prospective randomized study with long-term outcome evaluation. Obstet Gynecol. 1996;175(6):1418–22.
Maher CF, Qatawneh AM, Dwyer PL, Carey MP, Cornish A, Schluter PJ. Abdominal sacral colpopexy or vaginal sacrospinous colpopexy for vaginal vault prolapse: a prospective randomized study. Obstet Gynecol. 2004;190(1):20–6.
Segal S, Arya LA, Smith AL. Functional outcomes for incontinence and prolapse surgery. Curr Bladder Dysfunct Rep. 2012;7(3):179–86.
Roovers JP, Oelke M. Clinical relevance of urodynamic investigation tests prior to surgical correction of genital prolapse: a literature review. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(4):455–60.
Altman D, Vayrynen T, Engh ME, Axelsen S, Falconer C, Nordic. Transvaginal mesh group Anterior colporrhaphy versus transvaginal mesh for pelvic-organ prolapse. N Engl J Med. 2011;364(19):1826–36.
Acknowledgements
Our sincere thanks to the women who participated in the study. We also acknowledge the contribution of Mr. Rob Holmes, consultant gynecologist, who performed LSHP and entered the intraoperative and postoperative data of these women on BSUG.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Funding
None of the authors have any financial disclosure/conflict of interest.
Rights and permissions
About this article

Cite this article
Lone, F., Curnow, T. & Thomas, S.A. Laparoscopic sacrohysteropexy versus vaginal hysterectomy for uterovaginal prolapse using validated questionnaires: 2-year prospective study. Int Urogynecol J 29, 71–79 (2018). https://doi.org/10.1007/s00192-017-3405-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-017-3405-5