
Abstract
Introduction and hypothesis
Urethral injection therapy (UIT) has been performed since the early 20th century and a variety of agents have been launched. In 2006, polyacrylamide hydrogel (PAGH) was introduced and is now widely used as an agent. The objective was to evaluate the efficacy of PAGH based on a national population over a 5-year period (2007–2011) and the influence of patient-related factors, surgeon experience, and department volume.
Methods
A retrospective cohort study was carried out based on data from the Danish Urogynaecological Database (DugaBase).
Results
A total of 731 women were registered in the DugaBase. Cure was achieved in 75 out of 252 women (29.8%) and no leakage at all in 23 out of 252 (9.1%) at the 3-month follow-up. The mean total International Consultation on Incontinence Questionnaire-Short Form (ICIQ-SF) score decreased from 16 (SD 3.8) to 10.6 (SD 6.2; p < 0.001). UIT was performed at 16 departments, of which four high-volume departments performed 547 out of 814 UITs (67.2%). Women with severe UI had a decreased chance of cure (all ICIQ-SF scores), as did women on antimuscarinic drugs (adjusted OR 0.14; 95%, CI 0.04–0.41 “frequency”) and (adjusted OR 0.33; 95%, CI 0.13–0.82, “amount”). Women treated by a high-volume surgeon had a higher chance of cure (OR 4.51; 95% CI, 1.21–16.82, “frequency”) and a lower risk of 30-day hospital contacts (OR 0.27; 95% CI 0.09–0.76).
Conclusion
The study represented a cure for UIT among women in an everyday life setting. A surgeon learning curve for UIT was indicated, as was assigning interventions to fewer hands to improve the surgical training value and consequently the cure rate for women with UIT.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Urethral injection therapy (UIT) has been performed since the early 20th century and a variety of agents have been launched, but many were subsequently withdrawn from the market owing to product-specific side effects [1]. Currently, UIT remains an attractive alternative to synthetic midurethral slings (MUS) for the treatment of female urinary incontinence (UI) because of its minimally invasive nature and its few and mild side effects [2].
Polyacrylamide hydrogel (PAGH), introduced in Europe as a bulking agent in 2006, is now widely used [3]. The current knowledge of the efficacy and safety of UIT using PAGH is based on 10 studies with a follow-up of 1–3 years [4–13], 4 of which are major studies [4, 8, 11, 12]. However, no national population-based PAGH studies have been conducted and there is a lack of studies generally, which reflects the daily clinical practice [14]. Furthermore, patient characteristics associated with a decreased chance of cure among women injected with PAGH are not well-understood [14].
A few studies have indicated that there is a learning curve for surgeons in mastering the technique [4, 15, 16]. Two studies have up to now shown that both surgeon and department volume have an influence on subjective outcomes in UIT [4, 15], but no major studies have assessed these aspects.
The Danish Urogynaecological Database (DugaBase) was established in 2006 to monitor the quality of urogynaecological surgery [17]. This national clinical database provides a unique opportunity to retrieve information on women with UIT, as a large population-based sample size representing several years can be obtained.
The main purpose of the present study was to evaluate the effect of UIT on patient-reported outcome measures (PROMs) and the rate of 30-day hospital contacts based on a national background population over a 5-year period (2007–2011). Furthermore, we examined the influence of patient-related factors, surgeon experience, and department volume.
Materials and methods
Data sources
Data were retrieved from three Danish registers: DugaBase, the Danish National Patient Registry, and the Register of Medicinal Product Statistics.
All Danish residents have a unique personal identification number that incorporates date of birth and gender and is used for registering each individual’s contact (for purposes of consultation or treatment) with the national healthcare system, thus enabling linkage among all registries.
The DugaBase was established as a clinical database in 2006 and serves both clinical and scientific purposes [17–19]. It comprises women residing in Denmark who at the age of 18 or over undergo surgical procedures for UI or pelvic organ prolapse (POP) according to the NOMESCO procedure codes [20].
Since its establishment, pre- and postoperative questionnaires have been collected systematically [17]. These include the International Consultation on Incontinence Questionnaire-Short Form (ICIQ-SF), which has been translated into Danish, but not validated, and the Patient’s Global Impression of Improvement (PGI-I score), which was added in 2013 [18].
The database completeness of the DugaBase has increased from 33% in 2007 to 91% in 2011 using the Danish National Patient Registry as reference, whereas the data completeness constantly during this period has been lower [19]. This is mainly because follow-up after a UI procedure is not standardized: some departments routinely follow up all patients, whereas others only follow up on patients with complications.
The validity of 11 main variables has been examined and we found 90–100% agreement when comparing information from the database with medical records [17]. The standard for surgical quality is set by the DugaBase steering committee [21].
The Danish National Patient Registry was established in 1977 and provides information on diagnoses, minor procedures, and surgery undergone by inpatients, outpatients and emergency room visits in Danish hospitals [22]. Studies of procedure codes registered in the Danish National Patient Registry have shown a high validity [23].
It is mandatory under Danish law for all Danish hospital departments and private hospitals to report data to the DugaBase and the Danish National Patient Registry [22]. Furthermore, the hospitals are only reimbursed if they report to the Danish National Patient Registry [22].
The Register of Medicinal Product Statistics was established in 1993, and retrieves information from Danish pharmacies on medicinal products [24].
Study population and settings
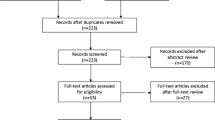
The Danish healthcare system is financed by taxes and provides care free of charge for all residents [22]. The study population included women aged 18 years or older residing in Denmark, who underwent first-time UIT using PAGH from 2007 through 2011, as registered in the DugaBase. To identify an instance of UIT in 2007 as being likely to be a woman’s first-time UIT, we included 2006 as a lag year. Only women who had completed the questionnaires pre- and postoperatively were included in the main analyses (Fig. 1). The guidelines for Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) were adhered to [25].

Description of the study cohort. The guidelines for Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) were applied
In 2003, PAGH (®Bulkamid) was introduced into Denmark, and by 2006, it had virtually replaced the previous PAGH agent (®Aquamid) [3]. In the present study, the agent predominantly used was PAGH (®Bulkamid), as less than 1.2% of cases (10 out of 814) involved other agents. In Denmark, UIT in women is performed transurethrally by a gynecologist using a urethroscope and normally three deposits are placed between the bladder neck and mid-urethra. The procedure is most often performed in an outpatient setting [4]. No formal training in UIT currently exists in Denmark. Routine, planned follow-up for the surgical treatment of UI is normally 3 months postoperatively.
Potential predictors
Potential variables associated with the outcome of UIT were patient-related factors, surgeon, and department volume.
Patient-related factors
Patient-related factors included a medical history, as registered in the DugaBase (age, body mass index [BMI], American Society of Anesthesiologists [ASA] classification, previous surgery (hysterectomy, UI surgery, POP), and severity of UI preoperatively according to the ICIQ-SF score.
Information on the preoperative use of medication related to UI was retrieved from The Register of Medicinal Product Statistics (diuretics [ATC C03], antimuscarinic drugs [ATC G04BD], estrogens [ATC G03C], and a group of less frequently used drugs [desmopressin ATC H01BA02, imipramine ATC N06AA02, and duloxetine ATC N06AX21]).
Surgeon volume
Surgeon volume, as registered in the DugaBase for each instance of UIT, was categorized into three groups of surgeon volume (number of UITs performed over their surgical career): low (≤25), medium (26–75), and high volume (>75).
Department volume
Department volume was defined as in a previous study, high (≥15 UITs per year) and low (<15 per year) [4]. The Danish National Patient Registry was used to verify that the classification of department volume was based on the actual annual number of UITs. A total of 814 out of 1,346 UITs were actually registered in the DugaBase. Sixteen of the 22 departments involved were registered in the DugaBase. The remaining 6 departments contributed 61 of the 1,346 UITs (4.5%). All 4 high-volume departments were registered both in the DugaBase and the Danish National Patient Registry.
Outcome measures
The primary outcomes were based on the ICIQ-SF completed at the 3-month follow-up after the primary UIT, and a secondary outcome was 30-day hospital contact.
The ICIQ-SF consists of three questions (frequency of UI, amount of leakage, and impact of UI on daily life) and results in a total score based on these questions (total ICIQ-SF).
Within each of the three questions, “cure” was based on a dichotomization as reported in accordance with globally accepted criteria reported previously (see Appendix, Fig. 3) [4–8, 12, 21]. The steering committee of the DugaBase has defined cure (a successful outcome) as leakage once a week or less, often or never, and we focused in particular on this outcome [21] and on “no leakage at all” on the frequency score, defined as answering “never” regarding leakage of urine [5]. “Change” was evaluated as the difference in the total ICIQ-SF score, pre- and postoperatively.
All relevant instances of contact with a Department of Obstetrics and Gynecology by women with a diagnosis classified according to the International Classification of Diseases, tenth edition (ICD 10) [26] within 30 days of initial UIT, were identified (referred to hereinafter as “30-day hospital contact”).
Statistical analysis
First-time UIT was the analytical unit. Descriptive statistics were used to evaluate baseline characteristics and outcomes. To evaluate baseline characteristics between patients treated by a low, medium or high surgeon volume, we used the Chi-squared test for trend (categorical variables) and one-way analysis of variance (ANOVA; continuous variables), and for department volume the Chi-squared test (categorical variables) and Student’s t test (continuous variables). Any change from baseline in the ICIQ-SF scores was analyzed using the Wilcoxon signed-rank test.
At logistic regression, the cure demonstrated in the ICIQ-SF score postoperatively was dichotomized for all three questionnaires and adjusted according to the preoperative ICIQ-SF score (“severity”). We analyzed the impact of patient-related factors believed to be clinically relevant and the influence of surgeon and department volume on cure by means of uni- and multivariate logistic regression. Hosmer–Lemeshow goodness-of-fit test was calculated to assess the fit of the models.
In the sensitivity analysis, we compared potential predictors before surgery between women who had filled in both questionnaires pre- and postoperatively on the one hand and women who had not completed the questionnaires (pre- and/or postoperatively) on the other. A p value < 0.05 was considered statistically significant. Data analysis was performed using STATA version 14.0 (StataCorp, College Station, TX, USA).
Results
Baseline characteristics
Between 1 January 2007 and 31 December 2011, a total of 731 women who underwent UIT for the first time were registered in the DugaBase. The mean age was 64, the mean BMI 26.7, and 56.5% had mixed UI (MUI) and 31% had pure stress UI (Table 1). Patient characteristics related to surgeon and department volume are reported separately (see Appendix, Table 4).
Among the 252 women who had pre- and postoperatively answered both questionnaires, 75 (29.8%) were cured and 23 (9.1%) had achieved no leakage at all by the 3-month follow-up (Fig. 2).

Frequency, before and after treatment—based on women who had completed questionnaires both pre- and postoperatively
For women with pure SUI, 40 out of 80 (50%) were cured, for MUI 60 out of 141 (43%), and for UUI, 4 out of 19 (21%; p < 0.07). There was a statistically significant improvement for all three ICIQ-SF scores (Table 2). The mean total ICIQ-SF score was 16.0 (SD 3.8) and after injection 10.6 (SD 6.2; p < 0.001).
Urethral injection therapy was performed in 16 departments, of which 4 high volume departments performed 547 out of 814 UITs (67.2%). More UITs were performed by high-volume surgeons in high-volume departments (368 out of 472 [75.9%]) compared with low-volume departments (117 out of 282 [24.1%] p < 0.001).
Patient-related factors
Among patient characteristics, the preoperative severity of UI significantly decreased the likelihood of cure in all ICIQ-SF scores (data not shown). Similarly, women on antimuscarinic drugs preoperatively had a significantly lower chance of cure according to the frequency score (adjusted OR 0.14; 95%, CI 0.04–0.41) and the amount score (adjusted OR 0.33; 95%, CI 0.13–0.82; Table 3). There was no influence of SUI, UUI or MUI on cure.
Surgeon volume
Women treated by a high-volume surgeon had an increased chance of cure according to the frequency score compared with women treated by a low-volume surgeon (adjusted OR 4.51; 95% CI, 1.21–16.82) and a lower risk of hospital contacts (adjusted OR 0.35; 95% CI, 0.16–0.79).
Department volume
The risk of 30-day hospital contact was lower for women treated in a high-volume department (adjusted OR 0.27; 95% CI 0.09–0.76).
Sensitivity analyses
At baseline, only a few differences in potential predictors between women who answered both total ICIQ-SF pre- and postoperatively and women who did not: BMI (26.4 vs 28.1, p = 0.02), ASA 1–2 (86.9% vs 74.5%, p = 0.03), previous UI surgery (16.5% vs 32.2%, p = 0.03), previous POP surgery (15.6 vs 32.3%, p = 0.02), department volume (low 34.5% vs 46.1; high 65.5% vs 53.9%, p = 0.02) and surgeon volume (low 18.2% vs 12.4%, medium 23.8% vs 15.7%; high 58.6% vs 71.9%, p = 0.03).
There were no differences in potential predictors between women who had completed both questionnaires and women who had only completed the questionnaire, either pre- or postoperatively (data not shown). There were no differences in severity of UI pre- or postoperatively, with regard to completion of all questionnaires (data not shown).
Discussion
This national population-based cohort study on transurethral PAGH injection among 731 women, from 2007 through 2011, demonstrated that 29% of the women were cured and 9% had no leakage at all at the 3-month follow-up. The mean total ICIQ-SF score improved statistically significantly from 16 to 10.6.
Comparison with other studies of PAGH is hampered by the usage of different PROMs, definitions of cure, sample sizes, and follow-up periods [10, 18, 27]. The short follow-up period of the present study differed from the ten PAGH studies that had follow-up periods of from 1 to 3 years [4–8, 12, 13]. Moreover, the majority of the studies reported results representing both one or more UITs [14], as opposed to our results, which exclusively represented women with first-time UIT [8].
The efficacy of PAGH in the present study may appear to be at the lower end of the spectrum compared with the literature [4, 6–13]. However, our results represented women who underwent UIT in an everyday life setting and surgeons with differing experience, as opposed to prospective studies financed by industry in which patients were “selected” [4, 7, 8, 11] and in which surgeons who conducted the studies were more likely experienced surgeons from high-volume departments [4, 8].
Nevertheless, studies based exclusively on women with severe UI or previous surgical treatment for UI reported equivalent [5] or better results compared with ours [6, 12, 13]. The women in these studies may have benefitted from more repeat UITs. However, only one study reported cure after the second UIT and the chance of cure was lower than after the first UIT [8].
Finally, definitions of both cure and no leakage at all are fairly strict outcome measures. Synthetic MUS and colposuspension, which are documented to be more effective [28], only demonstrate no leakage at all achieved in 40% and 30% of the patients at the long-term follow-up [29].
Even though the UIT cure rate may seem low, it still remains a viable option as it is less invasive and has fewer and milder side effects compared with synthetic MUS [14].
Similarly, the present study identified only a few patient characteristics that were predictors of a lower chance of cure. The severity of UI preoperatively was consistently and independently associated with lower chance of cure in all ICIQ-SF scores. There was no obvious influence of MUI and UUI on cure, although the absolute likelihood of cure for women with UUI was somewhat lower. Previous studies found a borderline poorer outcome for women with MUI injected with PAGH [4, 8, 10]. Women who used an antimuscarinic drug preoperatively had a decreased likelihood of cure and this may indicate that women with the most severe forms of MUI and UUI may have a decreased chance of cure. It seems paradoxical that the predictors for a lower chance of cure were found among women who most often have UIT, i.e., women with severe UI or severe MUI/UUI who are not candidates for synthetic MUS. This emphasizes the need for proper patient counselling to provide women with realistic expectations regarding outcome.
Women treated by a high -volume surgeon (>75 UITs) had significantly better outcomes on the frequency score and a significantly lower risk of 30-day hospital contact. Only two studies to date have pointed to a learning curve for UIT [4, 15] and the present study likewise only indicated this. Women treated at high-volume departments had a significantly lower risk of 30-day hospital contact, which corresponds to a previous multicenter study, which showed better results for departments that injected >15 UITs per year [4]. The influence of department volume in the present study probably reflects that significantly more surgeries were performed by high-volume surgeons in high-volume departments compared with low-volume departments. The majority of departments (12 out of 16) rarely performed UIT. As the annual number of UITs has decreased to 200 UITs during recent years in Denmark [30], a surgeon volume of >75 UITs will be difficult to achieve in the future.
The study has several strengths. We reported outcomes based on a national population of women consecutively registered in the DugaBase. This represented everyday life, unlike previous studies, which were either financed by industry with several exclusion criteria [5, 6, 9, 10] or involved women with severe UI [6] and previous surgical treatment [4, 7, 8, 11]. To the best of our knowledge, this is the largest study of UIT mainly using PAGH. We reported on issues not addressed previously including several clinical confounders. As outcome data were collected independently of the surgeon, the risk of investigator bias was minimized.
There were also limitations to the study, as we were only able to examine PROMs at short-term follow-up. Furthermore, our study indicated a learning curve for UIT. Future studies including more PROMs (e.g., the PGI-I score) will perhaps support evidence for a learning curve within UIT. Studies that explore aspects of this field are also needed, e.g., the threshold for acquiring the skill and which areas should be practiced.
Furthermore, we had no information on objective outcome measures and no reliable registration of surgical complications. There is at present focus on improving the database completeness for objective outcome measures, which will make future studies within this field possible.
Because of the low database completeness of the DugaBase at the beginning of our study period [21], we cannot exclude some selection bias, as not all low-volume departments were included in the study. However, as all four high-volume departments were registered in the DugaBase and performed the majority of the UITs, the lack of a few low-volume departments seems to be of minor importance, as their UIT contribution was small. Last but not least, there was a possible selection bias related to the patient characteristics, as women who had fulfilled both questionnaires were healthier (lower BMI, lower ASA score, and with less POP/UI surgery behind them) and more often from high-volume departments, compared with women who had not completed the questionnaires.
Conclusion
This national population-based cohort study represented women with a first-time injection at the 3-month follow-up in an everyday life setting. The results may seem to be at the lower end of the spectrum in comparison to the literature. However, UIT cure should be considered in the light of the fact that it is often performed in women who are not clinically suitable candidates for having or being willing to have a synthetic MUS. The severity of UI preoperatively was a strong predictor of a lower chance of cure and, similarly, the use of antimuscarinic drugs preoperatively indicated a poorer outcome for women with severe MUI and UUI. A learning curve for UIT was indicated, as was the recommendation that the treatment should be restricted to fewer hands to improve surgeon training and consequently the cure rate for women with UIT.
References
Meyer L. 2 tilfælde af incontinentia urinae helbredte ved parafininjektioner. Ugeskr Laeger. 1904;104:5.
Kotb AF, Campeau L, Corcos J. Urethral bulking agents: techniques and outcomes. Curr Urol Rep. 2009;10(5):396–400.
Lose G, Mouritsen L, Nielsen JB. A new bulking agent (polyacrylamide hydrogel) for treating stress urinary incontinence in women. BJU Int. 2006;98(1):100–4. doi:10.1111/j.1464-410X.2006.06205.x.
Lose G, Sorensen HC, Axelsen SM, Falconer C, Lobodasch K, Safwat T. An open multicenter study of polyacrylamide hydrogel (Bulkamid®) for female stress and mixed urinary incontinence. Int Urogynecol J. 2010;21(12):1471–7. doi:10.1007/s00192-010-1214-1.
Martan A, Masata J, Svabik K, El-Haddad R, Hubka P. Transurethral injection of polyacrylamide hydrogel (Bulkamid®) for the treatment of female stress urinary incontinence and changes in the cure rate over time. Ceska Gynekol. 2013;78(6):554–9.
Beraru A, Droupy S, Wagner L, Soustelle L, Muyschondt C, Ben Naoum K, et al. Efficacy of periurethral injections of polyacrylamide hydrogel (Bulkamid(®)) and quality of life of patients with urinary incontinence due to sphincter deficiency (IUE-IS). Prog Urol. 2014;24(8):501–10. doi:10.1016/j.purol.2014.02.003.
Leone Roberti Maggiore U, Alessandri F, Medica M, Gabelli M, Venturini PL, Ferrero S. Outpatient periurethral injections of polyacrylamide hydrogel for the treatment of female stress urinary incontinence: effectiveness and safety. Arch Gynecol Obstet. 2013;288(1):131–7. doi:10.1007/s00404-013-2718-y.
Toozs-Hobson P, Al-Singary W, Fynes M, Tegerstedt G, Lose G. Two-year follow-up of an open-label multicenter study of polyacrylamide hydrogel (Bulkamid®) for female stress and stress-predominant mixed incontinence. Int Urogynecol J. 2012;23(10):1373–8. doi:10.1007/s00192-012-1761-8.
Trutnovsky G, Tamussino K, Greimel E, Bjelic-Radisic V. Quality of life after periurethral injection with polyacrylamide hydrogel for stress urinary incontinence. Int Urogynecol J. 2011;22(3):353–6. doi:10.1007/s00192-010-1296-9.
Vecchioli-Scaldazza CV, Smaali C, Morosetti C, Azizi B, Giannubilo W, Ferrara V. Polyacrylamide hydrogel (bulkamid®) in female patients of 80 or more years with urinary incontinence. Int Braz J Urol. 2014;40(1):37–43. doi:10.1590/s1677-5538.ibju.2014.01.06.
Sokol ER, Karram MM, Dmochowski R. Efficacy and safety of polyacrylamide hydrogel for the treatment of female stress incontinence: a randomized, prospective, multicenter North American study. J Urol. 2014;192(3):843–9. doi:10.1016/j.juro.2014.03.109.
Pai A, Al-Singary W. Durability, safety and efficacy of polyacrylamide hydrogel (Bulkamid(®)) in the management of stress and mixed urinary incontinence: three year follow up outcomes. Cent European J Urol. 2015;68(4):428–33. doi:10.5173/ceju.2015.647.
Zivanovic I, Rautenberg O, Lobodasch K, von Bunau G, Walser C, Viereck V. Urethral bulking for recurrent stress urinary incontinence after midurethral sling failure. Neurourol Urodyn. 2016. doi:10.1002/nau.23007.
Kasi AD, Pergialiotis V, Perrea DN, Khunda A, Doumouchtsis SK. Polyacrylamide hydrogel (Bulkamid®) for stress urinary incontinence in women: a systematic review of the literature. Int Urogynecol J. 2016;27(3):367–75. doi:10.1007/s00192-015-2781-y.
Monga AK, Robinson D, Stanton SL. Periurethral collagen injections for genuine stress incontinence: a 2-year follow-up. Br J Urol. 1995;76(2):156–60.
Shah PJR. Injectables and GSI. Urol News. 1997;2:7–11.
Guldberg R, Brostrom S, Hansen JK, Kaerlev L, Gradel KO, Norgard BM, et al. The Danish Urogynaecological Database: establishment, completeness and validity. Int Urogynecol J. 2012;6(24):983–90. doi:10.1007/s00192-012-1968-8.
Larsen MD, Lose G, Guldberg R, Gradel KO. Discrepancies between patient-reported outcome measures when assessing urinary incontinence or pelvic- prolapse surgery. Int Urogynecol J. 2015;4(27):537–43. doi:10.1007/s00192-015-2840-4.
Guldberg R, Kesmodel US, Hansen JK, Gradel KO, Brostrom S, Kaerlev L, et al. Patient reported outcome measures in women undergoing surgery for urinary incontinence and pelvic organ prolapse in Denmark, 2006–2011. Int Urogynecol J. 2013;24(7):1127–34. doi:10.1007/s00192-012-1979-5.
Schiøler G, Larsen OB (2005) Klassifikation af operationer. 2 edn. Copenhagen: Munksgaard
Danish Urogynaecological Database, annual report 2007. Accessed 12 August 2016
Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sorensen HT. The Danish national patient registry: a review of content, data quality, and research potential. J Clin Epidemiol. 2015;7:449–90. doi:10.2147/clep.s91125.
Kjaergaard J, Clemmensen IH, Thomsen BL, Storm HH. Validity of diagnoses of and operations for nonmalignant gynecological conditions in the Danish national hospital registry. J Clin Epidemiol. 2002;55(2):137–42.
Kildemoes HW, Sorensen HT, Hallas J. The Danish national prescription registry. Scand J Public Health. 2011;39(7 Suppl):38–41. doi:10.1177/1403494810394717.
STROBE (2016) Strengthening the Reporting of Observational Studies in Epidemiology (STROBE). http://www.strobe-statement.org/index.php?id=available-checklists. Accessed 21 June 2016
International Classification of Diseases (ICD10). http://www.who.int/classifications/icd/ICD-10_2nd_ed_volume2.pdf. Accessed 31 August 2016
Castillo PA, Espaillat-Rijo LM, Davila GW. Outcome measures and definition of cure in female stress urinary incontinence surgery: a survey of recent publications. Int Urogynecol J. 2010;21(3):343–8. doi:10.1007/s00192-009-1032-5.
Kirchin V, Page T, Keegan PE, Atiemo K, Cody JD, McClinton S (2012) Urethral injection therapy for urinary incontinence in women. Cochrane Database Syst Rev 2:CD003881. doi:10.1002/14651858.CD003881.pub3
Freeman RM (2007) What’s a ‘cure’? Patient-centred outcomes of treatments for stress urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct 18(1):13–18 10.1007/s00192-006-0110-1
Statens Serum Institut. http://www.ssi.dk/Sundhedsdataogit/Sundhedsvaesenet%20i%20tal/Sundhedsveasenet%20generelt/Operationer/Operationer%20Regionsfordelt.aspx. Accessed 31 August 2016
Acknowledgements
Funding was provided by Aase og Ejnar Danielsens Fond and Edgar Schnohr og Hustru Gilberte Schnohr’s Fond. The Centre for Quality, Region of Southern Denmark, Middelfart, and the University of Southern Denmark financed the study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
The study was approved by the Danish Data Protection Agency (J.nr. 2012-41-0414). As the study did not include patient contact, it was not necessary to obtain approval from the Health Research Ethics Committee.
Conflicts of interest
Margrethe Foss Hansen incurred conference and travel expenses for attendance at the EUGA Leading Lights in Urogynaecology Congress, Warsaw, 2015, paid for by Astella. The other authors have no conflicts of interest to declare.
Appendix
Appendix

The International Consultation on Incontinence Questionnaire Short Form (ICIQ-SF)
Rights and permissions
About this article

Cite this article
Hansen, M.F., Lose, G., Kesmodel, U.S. et al. A national population-based cohort study of urethral injection therapy for female stress and mixed urinary incontinence: the Danish Urogynaecological Database, 2007–2011. Int Urogynecol J 28, 1309–1317 (2017). https://doi.org/10.1007/s00192-017-3265-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-017-3265-z