
Abstract
Introduction and hypothesis
Sexual health is an important aspect of women’s health. Women with urinary incontinence (UI) and pelvic organ prolapse (POP) have more complaints about sexual dysfunctions than do women without. In Iran, there is no questionnaire to assess sexual function in women who with UI; thus, this study aimed to translate the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (PISQ-12) and provide evidence for psychometric properties.
Methods
This cross-sectional study was conducted from April 2012 to October 2012 in a sample of women who attended an urogynecology clinic. Participants were divided into two groups (incontinent with or without POP and normal). All types of UI were assessed. The PISQ-12 was translated into Iranian based on international standards, and its reliability was assessed using test/retest reliability and internal consistency. In addition, its validity was evaluated using face and content validity, comparison with known groups, and convergent validity. Both exploratory and confirmatory factor analyses were conducted.
Results
Mean participant age was 47.52 years. Cronbach’s alpha coefficient was 0.84 for PISQ-12 and 0.70–0.79 for all domains. Pearson’s correlation coefficient between PISQ-12 and the Female Sexual Function Index (FSFI) was 0.73. Exploratory factor analysis loaded three factors; confirmatory factor analysis confirmed factor structures.
Discussion
This study showed that the Iranian version of PISQ-12 was a short, useful, valid, reliable, and condition-specific instrument to assess sexual function in women with UI/POP.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Pelvic floor disorders such as urinary incontinence (UI) and pelvic organ prolapse (POP) may have several adverse effects on sexual function [1, 2]. Both UI and sexual dysfunction might cause negative impacts on health-related quality of life (HR-QoL) [3, 4]. UI is associated with low libido, vaginal dryness, and dyspareunia [5] and is independent of age, race, and educational level [1]. Many women may be avoiding sexual intercourse due to fear or shame of incontinence during intercourse [6, 7]. In most societies like Iran, UI is a taboo, and women do not like to speak of it and its consequences, even with medical personnel [8, 9]. There are many different reasons, including shame, embarrassment [10], and lack of information on available treatment options [8]. Similarly, women have difficulty speaking about sexual dysfunction. In this regard, evidence suggests that despite their high prevalence, these problems remain undetected in health care clinics [11–13]. Therefore, a woman with concomitant UI and sexual dysfunction may have significant difficulty talking about her problems [14], which implies the need for finding ways to make it easier for every woman to receive the best possible care.
According to an Iranian study, 35.8 % of women do not seek help for their sexual dysfunction, and this issue is neglected in clinical surveys [15]. Lack of time is reported by both patients and clinicians as being one of the most common causes of screening failure [15, 16]. In this regard, administration of short, specific questionnaires in gynecology clinics might help identify patients who experience or are at risk of sexual dysfunction [17]. We believe that a brief, effective, multidimensional, inexpensive measure easy to understand and complete may help clinicians and patients in this respect.
Several general questionnaires are designed to assess female sexual function. Although many of them are valid and reliable, general questionnaires may not be sensitive enough to detect significant changes in women with special conditions such as UI [18]. Currently, only the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (PISQ-12) is condition specific and designed to assess sexual function in women with UI/ POP [19].
Rogers et al. developed the first self-report condition-specific questionnaire, known as PISQ [19]. The psychometric properties of PISQ-12 by Rogers and coworkers are well documented in many languages [20–22]; however, it is not available in Iran, and since many women in Iran, as in all countries, experience UI [23], there is a significant special need for a validated and reliable questionnaire. In fact, without condition-specific questionnaires, this problem will remain undetected in the clinical setting. Thus, this study aimed to translate and provide evidence for the psychometric properties of the Iranian version of PISQ-12 in order to use it in clinical settings and perhaps for research purposes.
Methods
Questionnaire and scoring
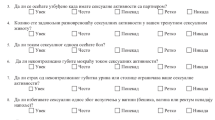
The PISQ-12 is the only validated, condition-specific, self administered questionnaire to assess sexual function in woman with UI and POP. It is composed of 12 items in three different domains: behavioral–emotive (4 items), physical (5 items), and partner related (3 items). The behavioral–emotive domain comprises questions about sexual desire, orgasm, excitement, and satisfaction. The physical domain assesses pain episodes during intercourse, incontinency of urine during intercourse, avoiding sexual function due to prolapse, and fear of urine or stool incontinence. The partner-related domain measures erection disorder, early ejaculation, and orgasm. Questions are rated on a five-point Likert scale ranging from 0 to 4, indicating a worse to better condition. Reverse scoring is used for questions 1– 4. The score of each domain is calculated by adding the score of each question [24]
Translation procedures
Psychometric properties of the Iranian version of PISQ-12 were done according to international standards mentioned below [25]. The flowchart of the study process is shown in Fig. 1.

Study process
Permission was obtained from the PISQ author to translate and validate the questionnaire in Iran. Two independent professional translators fluent in English translated the questionnaire from English into Persian. After assessing the two translated versions, disagreement was resolved and one forward version of the questionnaire was provided. Then, two native-English-speaking translators fluent in Iranian (other than the first translators) translated the forward version back into English. These translations were then compared with the original questionnaire. Finally, a panel of experts comprising a gynecologist, a midwife, a psychologist, an expert in psychometrics, the research team, and the translators reviewed all processes and assessed the questionnaire for wording and grammar. After careful consideration, consensus was reached, and the penultimate version of the Iranian questionnaire was provided.
To evaluate quantitative content validity, two indexes were used: content validity ratio (CVR) and content validity index (CVI). To examine CVR, the questionnaire was given to ten experts who were asked to assess each item based on a three-point Likert scale (essential, useful but not essential, not necessary). Based on the Lawshe CVR, to determine the minimum CVR value, each item with CVR >0.62 was considered significant and was maintained [26]. Then, in order to evaluate CVI, the questionnaire was provided to ten experts who were asked to assess each item based on a four-point Likert scale for relevancy, clarity, and simplicity. The CVI was calculated for each item.
The face validity was tested on 20 incontinent women with or without POP. All patients had a thorough understanding of the Persian language. Average age, education, and UI duration in this sample were 38 years, secondary, and 6 years, respectively. In order to determine the face validity, the following procedure was used. First, a questionnaire was completed by each participant. Then, all participants were asked about the meaning of each question to make sure they understand the entire questionnaire. Their answers were collected and showed that all patients had full understanding of the Iranian version of the PISQ-12. Finally, some minor changes were applied, according to patient comments, to finalize the questionnaire.
Participants and data collection
This cross-sectional study was conducted from April to October 2012 in Imam Khomeini Hospital, a large teaching hospital affiliated with Tehran University of Medical Sciences. A consecutive sample of women attending the urogynecologic clinic of the hospital was recruited to participate. Participants were examined to determine whether they had UI (as confirmed by urodynamic studies), and any degree of POP confirmed by a clinician blinded to the research (UI/POP). For staging prolapse, the terminology of the International Urogynecological Association (IUGA)/International Continence Society (ICS) was used [27]. If participants had no complications (no UI or POP), they were also invited to take part in the study and complete the questionnaire. Only Iranian women at least 20 years old, married and sexually active, able to read and write, and not pregnant were included in the study. Women with reversible causes of UI, functional disability, mental disorder, or associated diseases were excluded.
Statistical analysis
Different statistical tests were used to assess the psychometric properties of the Iranian version of the PISQ-12. Data were examined for normality. Since data followed a normal distribution, parametric tests were used.
-
1.
Validity: Known group comparisons were performed in order to examine whether the questionnaire could differentiate between subgroups of women who differed in continence or POP. Independent t test was used for comparison. We hypothesized that the normal group would score better than those with UI/POP. In addition, convergent validity was performed between PISQ-12 and the Female Sexual Function Index (FSFI; Iranian version), the psychometric properties of which are documented [28]. Pearson’s correlation coefficient (r) between the two questionnaires was computed: r ≥ 0.70 strong correlation, r 0.45–0.70 showed a moderate correlation, and r ≤ 0.45 displayed a week correlation (divergent validity).
-
2.
Reliability: For test–retest reliability, 20 patients completed the questionnaire twice, at a 2-week interval, and intraclass correlation coefficient (ICC) was calculated. Internal consistency was assessed by Cronbach’s alpha coefficient. Values ≥0.70 were considered significant [29].
-
3.
Factor analysis: Both exploratory (EFA) and confirmatory (CFA) factor analyses were performed. EFA was conducted using SPSS version 16. In order to extract data, principal component analysis was used. Data reduction was performed with varimax using the Kaiser normalization method. Confirmatory factor analysis was performed using Lisrel.
-
4.
Factor model of the Iranian version of PISQ-12 was assessed. Various fit indexes including goodness-of-fit index (GFI), adjusted goodness-of-fit index (AGFI), the root mean square error of approximation (RMSEA), normal fit index (NFI), and comparative fit index (CFI) were used to achieve model fitness.
Ethics
The Ethics Committee of Tehran University of Medical Sciences approved the study, and all participants completed an informed consent form before entering the study. A private environment was provided for participants to complete the questionnaire, and all participant information was kept confidential.
Results
Demographic characteristics of the study sample
In all, 200 women participated in this study: 100 in the normal group and 100 in the UI/POP group. No participant was excluded, and there were no missing items (0 %). Mean participant age was 47.52 [standard deviation (SD) 9.84; range 29–78] years. Most participants were housewives (79 %), and educational level of the majority was secondary school (57.5 %). There was no difference in age, educational level, menopausal status, and mode of infant delivery between groups (P > 0.05). According to the international classification of adult body mass index (BMI), most participants were overweight. Demographic characteristics of the study samples are shown in Table 1.
Content validity
Results of quantitative CVR was 0.80 and CVI 0.70, indicating that all items were suitable.
Known group comparisons
Table 2 presents the comparison of sexual function between normal and UI/POP groups. There was a statistically significant difference in PISQ-12 between groups and behavioral–emotive and physical domains (P < 0.001). Differences in the partner-related domain were not significant between groups (P = 0.09).
Convergent validity
Convergent validity of the PISQ-12 is shown in Table 3. Pearson’s correlation coefficient showed that correlation between the physical domain and the excitement and pain domain was strong (r ≥ 0.70). For the FSFI, apart from the pain domain, the correlation between the behavioral–emotive domain and all domains was strong (r ≥ 0.70). In the partner-related domain, the correlation with desire and satisfaction was week (r ≤ 0.45), indicating divergent validity.
Reliability
Cronbach’s alpha coefficient of the questionnaire was 0.84, and alpha for the entire subscale ranged from 0.70 to 0.79. In addition, ICC was 0.95 and ranged from 0.93 to 0.96 for all subscales. Results are shown in Table 4.
Factor analysis
Results of exploratory factor analysis are shown in Table 5. The calculated Kaiser–Meyer–Olkin (KMO) was 0.80, and Bartlett’s test of sphericity was significant (P < 0.001). Results of confirmatory factor analysis showed that the patterns of the three domains had good fit indexes (GFI = 0.88, RMSEA = 0.10, AGFI = 0.82, NFI = 0.90, CFI = 0.93).
Discussion
The aim of this study was to validate the Iranian version of the PISQ-12. The results indicated it is a valid and reliable measure to assess sexual function in women with UI and POP and has appropriate psychometric properties.
Results showed the satisfactory reproducibility of the Iranian version of the PISQ-12: Cronbach’s alpha coefficient for all domains was perfect, indicating excellent reproducibility. CVI and CVR showed high content validity. A strong correlation was observed with FSFI. Known group comparison analysis showed it can discriminate between clinically different patients, i.e., continent and incontinent women. There was a three-factor solution for this questionnaire that was similar to its original language. Exploratory factor analysis indicated that items 1, 2, 3, 4, and 12 loaded in the behavioral–emotive domain; items 5, 6, 7, 8, and 9 loaded in the physical domain; and items 10 and 11 loaded in the partner-related domain. Several factors, such as cultural differences, can cause this difference. These findings can be explained by the fact participants in the study experienced orgasmic intensity as a behavioral–emotive component. Therefore, item no 12 was located in a different domain.
Our study had some limitations that need to be addressed. Although it was conducted in a tertiary referral center, patients with UI who attend the urogynecology clinic may differ from the entire UI population, so findings may not be generalizable. In addition, patients attending other centers may differ in terms of sociocultural conditions, so studies in different centers with larger samples are needed.
Conclusion
Psychometric assessment of the Iranian version of the PISQ-12 suggests it is a short, useful, valid, reliable, condition-specific instrument to assess sexual function in women with UI/POP.
References
Handa VL, Harvey L, Cundiff GW, Siddique SA, Kjerulff KH (2004) Sexual function among women with urinary incontinence and pelvic organ prolapse. Am J Obstet Gynecol 191(3):751–756
Novi JM, Jeronis S, Morgan MA, Arya LA (2005) Sexual function in woman with pelvic organ prolapse compared to woman without pelvic organ prolapse. J Urol 173:1669–1672
Kwon BE, Kim GY, Son YJ, Roh YS, You M (2010) Quality of life of women with urinary incontinence: a systematic literature review. Int Neurourol J 14(3):133–138
Asoglu MR, Selcuk S, Cam C, Cogendez E, Karateke A (2014) Effects of urinary incontinence subtypes on women’s quality of life (including sexual life) and psychosocial state. Eur J Obstet Gynecoland Reprod Biol 176:187–190
Handa VL, Cundiff G, Chang HH, Helzlsouer KJ (2008) Female sexual function and pelvic floor disorders. Obstet Gynecol 111(5):1045
Tok EC, Yasa O, Ertunc D, Savas A, Durukan H, Kanik A (2010) The effect of pelvic organ prolapse on sexual function in a general cohort of women. J Sex Med 7(12):3957–3962
Rogers GR, Villarreal A, Kammerer-Doak D, Qualls C (2001) Sexual function in women with and without urinary incontinence and/or pelvic organ prolapse. Int Urogynecol J 12(6):361–365
Lose G (2005) The burden of stress urinary incontinence. Eur Urol Suppl 4(1):5–10
Rezai-Pour A, Mir-Mowlai T, Mahmoudi M, Jabbari K, Beh Bin Z (2002) Study in quality of life of women suffering from urinary incontinence. Hayat 8(3):13–21
Margalith I, Gillon G, Gordon D (2004) Urinary incontinence in women under 65: quality of life, stress related to incontinence and patterns of seeking health care. Qual Life Res 13(8):1381–1390
Moreira ED, Brock G, Glasser DB, Nicolosi A, Laumann EO, Paik A, Gingell C (2005) Help‐seeking behaviour for sexual problems: the Global Study of Sexual Attitudes and Behaviors. Int J Clin Pract 59(1):6–16
Moreira ED, Glasser DB, Nicolosi A, Duarte FG, Gingell C (2008) Sexual problems and help‐seeking behaviour in adults in the United Kingdom and continental Europe. BJU Int 101(8):1005–1011
Nicolosi A, Buvat J, Glasser DB, Hartmann U, Laumann EO, Gingell C (2006) Sexual behaviour, sexual dysfunctions and related help seeking patterns in middle-aged and elderly Europeans: the global study of sexual attitudes and behaviors. World J Urol 24(4):423–428
Harris SS, Link CL, Tennstedt SL, Kusek JW, McKinlay JB (2007) Care seeking and treatment for urinary incontinence in a diverse population. J Urol 177(2):680–684
Vahdaninia M, Montazeri A, Goshtasebi A (2009) Help-seeking behaviors for female sexual dysfunction: a cross sectional study from Iran. BMC Womens Health 9(1):3
Roos AM, Thakar R, Sultan AH, Scheer I (2009) Female sexual dysfunction: are urogynecologists ready for it? Int Urogynecol J Pelvic Floor Dysfunct 20(1):89–101
Kingsberg S, Althof SE (2009) Evaluation and treatment of female sexual disorders. Int Urogynecol J 20(1):33–43
Omotosho TB, Rogers RG (2009) Shortcomings/strengths of specific sexual function questionnaires currently used in urogynecology: a literature review. Int Urogynecol J 20(1):51–56
Rogers RG, Kammerer-Doak D, Villarreal A, Coates K, Qualls C (2001) A new instrument to measure sexual function in women with urinary incontinence or pelvic organ prolapse. Am J Obstet Gynecol 184(4):552–558
Romero AA, Hardart A, Kobak W, Qualls C, Rogers R (2003) Validation of a Spanish version of the pelvic organ prolapse incontinence sexual questionnaire. Obstet Gynecol 102(5, Part 1):1000–1005
Fatton B, Letouzey V, Lagrange E, Mares P, Jacquetin B, De Tayrac R (2009) Validation of a French version of the short form of the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (PISQ-12). J Gynecol Obstet Biol Reprod 38(8):662–667
Cam C, Sancak P, Karahan N, Sancak A, Celik C, Karateke A (2009) Validation of the short form of the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (PISQ-12) in a Turkish population. Eur J Obstet Gynecol Reprod Biol 146(1):104–107
Nojomi M, Bibi Amin E, Bashiri Rad R (2008) Urinary incontinence: hospital-based prevalence and risk factors. J Res Med Sci 13(1):22–28
Rogers RG, Coates KW, Kammerer-Doak D, Khalsa S, Qualls C (2003) A short form of the pelvic organ prolapse/urinary incontinence sexual questionnaire (PISQ-12). Int Urogynecol J 14(3):164–168
Beaton DE, Bombardier C, Guillemin F, Ferraz MB (2000) Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 25(24):3186–3191
Lawshe CH (1975) A qualitative approach to content validity. Pers Psychol 28(4):563–575
Haylen BT, De Ridder D, Freeman RM, Swift SE, Berghmans B, Lee J, Schaer GN (2010) An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int Urogynecol J 21(1):5–26
Mohammadi KH, Heydari M (2008) The female sexual function index (FSFI): validation of the Iranian version. Payesh 7(3):269–278
Cronbach LJ (1951) Coefficient alpha and the internal structure of tests. Psychometrika 16(3):297–334
Acknowledgments
This study was part of master’s degree thesis supported by Tehran University of Medical Sciences. We are grateful to Rebecca Rogers for granting us the permission to translate and validate the PISQ-12. We also wish to thank the Research Deputy of Tehran University, the staff of Imam Khomeini Hospital, and specially Mrs. Jabari, for their support and assistance.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Zohre, M., Minoo, P. & Ali, M. Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (PISQ-12): psychometric validation of the Iranian version. Int Urogynecol J 26, 433–439 (2015). https://doi.org/10.1007/s00192-014-2520-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-014-2520-9