
Abstract
Purpose
To compare patient characteristics including patient sex, age, body mass index (BMI), activities at the time of injury and injury profiles in patients with anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) injuries.
Methods
Data were obtained from the Swedish National Knee Ligament Registry. Two study groups were created: (1) index ACL reconstruction (ACL group) and (2) index PCL reconstruction (PCL group). Between-group differences were investigated using Fisher’s exact test and Fisher’s non-parametric permutation test for dichotomous variables and continuous variables, respectively.
Results
Of 39,010 patients, 38,904 were ACL injuries. A larger proportion of patients with combined injuries to the PCL, meniscus and cartilage were female, aged > 25 years and with a BMI of > 35 kg/m2 compared with patients with combined injuries to the ACL, meniscus and cartilage. An isolated ACL injury was more commonly found in males, while all other injury profiles of ACL, including combined injuries with meniscus, cartilage and collateral ligament injuries, were more frequently observed in females. The PCL injuries were sustained either during pivoting sports, non-pivoting sports or were traffic-related.
Conclusion
Different patient characteristics (BMI, age and sex), and activities at the time of injury (sport- versus traffic-related activities), resulted in distinct injury profiles for the ACL and PCL groups. These findings provide valuable information of the way specific injury patterns of cruciate ligament injuries occur, and subsequently may help clinicians with the diagnostic process of ACL and PCL injuries.
Level of evidence
III.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Injuries to the cruciate ligaments, including anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) tears, are severe injuries affecting athletes in their ability to return to sport [23, 25, 26]. Previous studies have demonstrated a higher incidence of PCL injuries in men [14, 17], while female athletes appear to run a greater risk of sustaining an ACL injury [4, 11]. Furthermore, ACL injuries are reported to occur more commonly in young high-level female athletes, while males affected by an ACL injury are reported to be somewhat older [24]. A higher body mass index (BMI) has also been related to an increased risk of sustaining cruciate ligament injuries[29] and has been reported to be an important contributory factor in combined knee ligament injuries [28]. Additionally, different injury profiles of knee ligament injuries have been linked to different types of injury mechanism, where ACL injuries have usually been associated with non-contact sports and PCL injuries with high-energy trauma [6, 14, 20, 33]. Consequently, PCL injuries more frequently coincide with additional knee ligament tears, while ACL injuries more often occur with concurrent meniscal lesions [20, 30].
Despite the rising incidence of cruciate ligament injuries and their negative impact on both sports participation and general knee function, the specific injury profiles for ACL and PCL injuries are yet to be described. Thus, the purpose of this study was to explore and compare patient characteristics including patient sex, age, BMI and activity at the time of injury, as well as injury profiles in patients undergoing either ACL or PCL reconstruction. It was hypothesised that ACL and PCL injuries would have distinct injury profiles, where ACL injuries would be more common in younger patients with a lower BMI, while patients with PCL injuries would be older and have a higher BMI. A deeper understanding of the profiles of these severe knee injuries could lead to improved treatment planning and, subsequently, improved treatment-related outcomes. Additionally, an increased knowledge of injury profiles for cruciate ligament injuries could provide essential information relating to possible factors associated with specific forms of ACL and PCL injury in order to formulate secondary prevention strategies based on patients’ individual characteristics and activities.
Materials and methods
This retrospective cohort study was approved by the Swedish Ethical Review Authority (registration number: 2020-03559 and 2021-01002) and was performed in accordance with the Declaration of Helsinki.
Data were obtained from the Swedish National Knee Ligament Register (SNKLR), which mainly collects data on surgically treated ACL and PCL injuries. The registry includes both surgeon- and patient-reported information, including demographical characteristics, injury- and surgery-related factors and patient-reported outcome measurements (PROMs) [2]. Participation in the SNKLR is optional and exclusion can be requested if research participation is not desired by the patient. The registry has previously been described in more detail [12].
Data collection and study sample
The data obtained from the SNKLR were collected between 1 January 2005 and 31 December 2019. Only data on patients undergoing either ACL reconstruction (ACL-R) or PCL reconstruction (PCL-R) were obtained from the register. Two main study groups were created, including patients who had undergone an index ACL reconstruction (ACL group) and an index PCL reconstruction (PCL group). Additionally, the following groups were created for subgroup analysis: isolated ACL injury, ACL injury + meniscal injury + cartilage injury, ACL injury + collateral ligament injury, isolated PCL injury, PCL injury + meniscal injury + cartilage injury and PCL injury + collateral ligament injury. Patients with any concomitant fracture, as well as combined ACL and PCL injuries, were excluded. In addition, patients with revision ACL or PCL, or previous knee surgeries were excluded from further assessment. Patient characteristics including age, patient sex, BMI, smoking status, activity at the time of injury and the type of injury (ACL versus PCL injuries) were extracted from the SNKLR. Surgical data on concomitant injuries, including information on neurovascular injuries, injuries to the posterior lateral corner (PLC) and cartilage lesions, as well as meniscal and collateral ligament injuries, were extracted for further analyses. Activities at the time of injury were divided into the following categories: sports-related injuries, including alpine/skiing, pivoting sport, non-pivoting sport and other physical activity (other recreational sport, exercise and trampoline), as well as traffic-related injuries and other activities at the time of injury (other, outdoor and work activity). Moreover, sports including American football/rugby, basketball, dancing, floorball, gymnastics, handball, ice hockey, bandy, martial arts, racket sports, football, volleyball and wrestling were categorised as pivoting sports, while cross-country skiing, cycling, horseback riding, motocross/enduro, skateboarding, snowboarding and surfing/wakeboarding were categorised as non-pivoting sports.
Statistical analyses
The statistical analyses were performed using the SAS System for Windows (version 9, SAS Institute, North Carolina, USA). Continuous and ordinal data are presented as the mean and standard deviation (SD), as well as the median with minimum and maximum, while count (n) and proportion (%) are used for dichotomous variables. Between-group differences were investigated using Fisher’s exact test for dichotomous variables. Fisher’s non-parametric permutation test was used to compare differences in continuous variables between the study groups. All the tests were two-tailed at a 5% significance level.
Results
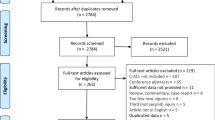
Baseline data were available for 39,010 patients (Fig. 1), of which 38,904 patients had undergone an ACL reconstruction. The ACL group was significantly younger compared with the PCL group (mean 27 ± 10 and 31 ± 13 years), p < 0.01). Male sex was reported for 57% of patients with ACL-R and 62% of patients with PCL-R (p = 0.32). There was no significant difference between groups with regard to BMI (p = 0.15). Table 1 presents a detailed description of patient characteristics.

Flow chart of patient enrolment. Values are given as the count (n). ACL anterior cruciate ligament, PCL posterior cruciate ligament
Concomitant injuries
The presence of concomitant injuries compared between the ACL group and PCL group did not reach statistical significance (p = 0.05; Table 2). However, more cartilage injuries were seen in the PCL group (38%) compared with the ACL group (26%) (p = 0.01) and ACL injuries more frequently occurred in conjunction with meniscal injuries (44%) compared with PCL injuries (23%) (p < 0.001). Furthermore, concomitant collateral ligament injuries were more frequently present in the PCL group (47%) compared with the ACL group (5.0%) (p < 0.001; Table 2).
Activity at time of injury
The most frequently reported activity at the time of injury for both the ACL and PCL groups was sports. However, a larger proportion of ACL injuries were sustained during sports than for PCL injuries (p < 0.001). Among sports-related ACL injuries, 65% and 16% were associated with pivoting sports and alpine/skiing respectively, while sports-related PCL injuries were most frequently caused by pivoting (32%) and non-pivoting sports (13%). Moreover, a larger proportion of traffic-related injuries was reported among patients with PCL tears (24%) compared with the ACL group (2.0%, p < 0.001; Table 1).
Injury profile
Different patient characteristics resulted in distinct injury profiles for ACL and PCL injuries (Fig. 2.). Patients with combined injuries to the PCL, meniscus and cartilage were more often female, aged > 25 years and with a BMI of > 35 kg/m2 compared with patients with combined injuries to the ACL, meniscus and cartilage. Moreover, patients with combined injuries to the PCL and collateral ligament had a higher BMI (BMI > 35 kg/m2) and they were slightly younger and more frequently male compared with patients with combined injuries to the PCL, meniscus and cartilage. Patients with ACL injuries generally had a lower BMI (BMI < 35 kg/m2) compared with patients with PCL injuries. An isolated ACL injury was more commonly found in males, while all other injury profiles of ACL, including combined injuries with meniscus, cartilage and collateral ligament injuries, were more frequently observed in females. Additionally, a larger proportion of PCL injuries was found in females compared with males.

Spider chart of different injury profiles, by demographical dimension. Different patient characteristics are found in different injury patterns for ACL and PCL injuries. ACL anterior cruciate ligament, BMI body mass index, PCL posterior cruciate ligament
Differences in activities at the time of injury were identified among the specific injury profiles of ACL and PCL injury groups (Fig. 3). Pivoting sport was the most prevalent activity at the time of injury in patients with an isolated ACL injury, while an isolated PCL injury was the result of either pivoting sports, non-pivoting or traffic-related activity. Moreover, combined injuries to the ACL, meniscus and cartilage were most frequently the result of a pivoting sport, while both alpine/skiing and pivoting sport were the most common activities at the time of injury for a combined injury to the ACL and collateral ligaments. Both an isolated PCL injury and a combined injury to the PCL and collateral ligaments were usually either traffic related or occurred during pivoting sport. However, a PCL injury combined with meniscal and cartilage lesions was most frequently sustained in a traffic-related activity at the time of injury or other physical activities.

Spider chart of different injury profiles, by the type of activity at the time of injury. Differences in activity at the time of injury are found among the specific injury profiles of ACL- and PCL-injured knees. Pivoting sport: American football/rugby, basketball, dancing, floorball, gymnastics, handball, ice hockey/bandy, martial arts, racket sports, football, volleyball, wrestling. Non-pivoting sport: cross-country skiing, cycling, horseback riding, motocross/enduro, skateboarding, snowboarding and surfing/wakeboarding. Other physical activity: other recreational sport, exercise, trampoline. Other: other, outdoor activity and work. ACL anterior cruciate ligament, PCL posterior cruciate ligament
Discussion
The most important findings in this study were the differences in injury profiles for patients with ACL and PCL injuries. An isolated ACL injury was more commonly found in males, while all other injury profiles of ACL, including combined injuries with meniscus, cartilage and collateral ligament injuries, were more frequently observed in females compared with males. Moreover, a larger proportion of PCL injuries was found in females compared with males.
Concomitant injuries to the collateral ligaments and the articular cartilage were more prevalent in the PCL group compared with the ACL group. In contrast, ACL injuries more frequently occurred either in isolation or in combination with meniscal injuries. These findings are in agreement with previous studies reporting a higher incidence of various concomitant injuries in a population with PCL injuries, whereas ACL injuries tend to occur either in isolation or in conjunction with meniscal lesions [8, 24]. Furthermore, the higher occurrence of concomitant injuries in PCL-injured populations has previously been attributed to high-energy injury mechanisms, leading to more complex patterns of knee ligament injuries [7, 8, 35]. In line with previous research, [3, 8, 9, 27], a high rate of traffic- and sports-related injury mechanisms has been reported in the population with a PCL injury, while ACL injuries most commonly occurred due to sports-related activities, especially pivoting sports.
Further differences in patient characteristics were noted between injury profiles of ACL and PCL injuries. A larger proportion of patients with combined injuries to the PCL, meniscus and cartilage was more frequently female, slightly older (> 25 years) and had a higher BMI (> 35 kg/m2) compared with the patients with combined injuries to the ACL, meniscus and cartilage. However, the high rate of PCL injuries combined with meniscus and cartilage lesions in female patients with a higher BMI may be explained by the knowledge that females more commonly sustain knee ligament injuries due to lower-energy mechanisms compared with males who are more frequently subject to high-energy injuries [33]. As a result, this information regarding female sex, a higher BMI and the relationship of these characteristics with complex PCL injuries may be helpful during the diagnostic process in order to arrive at a correct diagnosis, as well as being able to provide accurate treatment. Additionally, an increased BMI (≥ 30 kg/m2) has previously been associated with an increased risk of serious knee ligament injuries following low-energy trauma [22].
Isolated ACL injuries were more prevalent in males, while all other injury profiles of ACL and PCL injuries were more frequently seen in females. It has previously been established that female athletes run a higher risk of sustaining an ACL injury compared with males [4, 21, 34], resulting in a greater possibility of different injury profiles and concomitant injuries. Moreover, female athletes have been reported to have a higher BMI compared with males, causing higher ground reaction forces[31] and subsequently increasing the risk of more complex knee injuries. This finding may be of prognostic value following injury, since isolated ACL reconstruction can lead to superior outcomes and a lower rate of long-term osteoarthritis compared with ACL reconstruction with concomitant injuries [10].
Differences with regard to activity at the time of injury were identified among the specific injury profiles for ACL and PCL injuries and are in partial agreement with previous studies [14, 32, 35]. While pivoting sport was the most prevalent activity at the time of injury in patients with isolated ACL injuries, an isolated PCL injury was the result of either pivoting sports, non-pivoting or traffic-related activity. Although the high rate of ACL injuries due to pivoting sports is well established [9, 15], the relationship between PCL injuries and non-pivoting sports is less well known. However, the higher prevalence of PCL injuries compared with ACL injuries in non-pivoting athletes could be explained by the relatively greater popularity of cross-country skiing and snowboarding in Sweden compared with other countries, where pivoting sports including football and basketball are more popular Furthermore, ACL injuries accompanied by meniscus and cartilage injuries were most frequently observed in conjunction with pivoting sports activity at the time of injury, while alpine/skiing and pivoting sport were the most prevalent mechanisms of injury for ACL injuries with collateral ligament injuries. Additionally, the high incidence of combined ACL/MCL injuries in the alpine/skiing population has previously been reported[18, 19] and may be attributed to the high-energy impact and forces usually seen in skiing injury situations. Furthermore, pivoting sport activities have previously been associated with combined injuries to the ACL and meniscus [3, 5], supporting the importance of the meniscus as a secondary stabiliser during pivoting activities [13, 16]. Interestingly, isolated PCL and combined PCL and collateral ligament injuries were caused by similar activities and, as a result, no large differences in activities at the time of injury were observed. Since the activity at the time of injury is similar in these groups, patient characteristics, such as a higher BMI, may possibly be an explanation of the observed difference in injury profiles. Conversely, PCL injuries combined with meniscal and cartilage lesions were most commonly the result of traffic-related injury mechanisms or other physical activities, demonstrating an association between high-energy trauma and more complex knee ligament injuries.
This study has several strengths and limitations. The strengths in the current study include the overall large sample size, including detailed information on a total of 39,010 patients. Additionally, the SNKLR has been estimated to cover approximately 90% of all ACL reconstructions in Sweden [1, 2] and the study sample is therefore representative of the Swedish ACL-reconstructed population. One limitation of this study was the relatively small sample size of included PCL injuries. The primary focus of the SNKLR is the collection of data with regard to surgically treated ACL injuries, which can, in turn, explain the small sample size of patients with PCL injuries. In addition, the annual incidence of PCL injuries is considerably lower compared with the annual incidence of ACL injuries [24, 25], which can partly explain the small sample size of included PCL injuries. Finally, this study was retrospective in nature, which can only indicate relationships between patient characteristics and ACL or PCL injury profiles rather than causal relationships. However, the results of this study, demonstrating distinct injury profiles for ACL and PCL injuries, can be considered as clinically important and subsequently, may help clinicians with the diagnostic process of ACL and PCL injuries.
Conclusion
This study from the SNKLR shows that patient characteristics and activities at the time of injury resulted in specific injury profiles for ACL and PCL, as follows. (1) Females, older patients and patients with a higher BMI were more susceptible to more complex injuries, such as combined PCL injuries; (2) a larger proportion of combined ACL, meniscus and cartilage injuries was found in females; (3) isolated ACL injuries were most frequently found in males; (4) ACL injuries were sustained during pivoting sports or alpine skiing; (5) PCL injuries were sustained either during pivoting sports, non-pivoting sports or were traffic related. These data provide valuable information to increase our understanding of how specific injury forms of cruciate ligament injury (ACL and PCL) occur and can help clinicians with the diagnostic process of ACL and PCL injuries.
References
XBase The Swedish knee ligament registry. Annual Report 2020.
Ahldén M, Samuelsson K, Sernert N, Forssblad M, Karlsson J, Kartus J (2012) The Swedish National Anterior Cruciate Ligament Register: a report on baseline variables and outcomes of surgery for almost 18,000 patients. Am J Sports Med 40:2230–2235
Alentorn-Geli E, Myer GD, Silvers HJ, Samitier G, Romero D, Lázaro-Haro C et al (2009) Prevention of non-contact anterior cruciate ligament injuries in soccer players. Part 1: mechanisms of injury and underlying risk factors. Knee Surg Sports Traumatol Arthrosc 17:705–729
Arendt EA, Agel J, Dick R (1999) Anterior cruciate ligament injury patterns among collegiate men and women. J Athl Train 34:86–92
Astur DC, Xerez M, Rozas J, Debieux PV, Franciozi CE, Cohen M (2016) Anterior cruciate ligament and meniscal injuries in sports: incidence, time of practice until injury, and limitations caused after trauma. Rev Bras Ortop 51:652–656
Boden BP, Dean GS, Feagin JA Jr, Garrett WE Jr (2000) Mechanisms of anterior cruciate ligament injury. Orthopedics 23:573–578
Caldas MTL, Braga GF, Mendes SL, da Silveira JM, Kopke RM (2013) Posterior cruciate ligament injury: characteristics and associations of most frequent injuries. Rev Bras Ortop (English Edition) 48:427–431
Fanelli GC, Edson CJ (1995) Posterior cruciate ligament injuries in trauma patients: part II. Arthroscopy 11:526–529
Granan LP, Inacio MC, Maletis GB, Funahashi TT, Engebretsen L (2013) Sport-specific injury pattern recorded during anterior cruciate ligament reconstruction. Am J Sports Med 41:2814–2818
Grassi A, Pizza N, Al-Zu’bi BBH, Fabbro GD, Lucidi GA, Zaffagnini S (2022) Clinical outcomes and osteoarthritis at very long-term follow-up after ACL reconstruction: a systematic review and meta-analysis. Orthop J Sports Med 10:23259671211062240
Gwinn DE, Wilckens JH, McDevitt ER, Ross G, Kao TC (2000) The relative incidence of anterior cruciate ligament injury in men and women at the United States Naval Academy. Am J Sports Med 28:98–102
Hamrin Senorski E, Svantesson E, Engebretsen L, Lind M, Forssblad M, Karlsson J et al (2019) 15 years of the Scandinavian knee ligament registries: lessons, limitations and likely prospects. Br J Sports Med 53:1259–1260
Katakura M, Horie M, Watanabe T, Katagiri H, Otabe K, Ohara T et al (2019) Effect of meniscus repair on pivot-shift during anterior cruciate ligament reconstruction: objective evaluation using triaxial accelerometer. Knee 26:124–131
Lind M, Nielsen TG, Behrndtz K (2018) Both isolated and multi-ligament posterior cruciate ligament reconstruction results in improved subjective outcome: results from the Danish Knee Ligament Reconstruction Registry. Knee Surg Sports Traumatol Arthrosc 26:1190–1196
Lindanger L, Strand T, Mølster AO, Solheim E, Inderhaug E (2019) Return to play and long-term participation in pivoting sports after anterior cruciate ligament reconstruction. Am J Sports Med 47:3339–3346
Musahl V, Citak M, O’Loughlin PF, Choi D, Bedi A, Pearle AD (2010) The effect of medial versus lateral meniscectomy on the stability of the anterior cruciate ligament-deficient knee. Am J Sports Med 38:1591–1597
Owesen C, Sandven-Thrane S, Lind M, Forssblad M, Granan LP, Årøen A (2017) Epidemiology of surgically treated posterior cruciate ligament injuries in Scandinavia. Knee Surg Sports Traumatol Arthrosc 25:2384–2391
Posch M, Schranz A, Lener M, Tecklenburg K, Burtscher M, Ruedl G (2021) In recreational alpine skiing, the ACL is predominantly injured in all knee injuries needing hospitalisation. Knee Surg, Sports Traumatol, Arthrosc 29:1790–1796
Posch M, Schranz A, Lener M, Tecklenburg K, Burtscher M, Ruedl G (2021) In recreational alpine skiing, the ACL is predominantly injured in all knee injuries needing hospitalisation. Knee Surg Sports Traumatol Arthrosc 29:1790–1796
Prentice HA, Lind M, Mouton C, Persson A, Magnusson H, Gabr A et al (2018) Patient demographic and surgical characteristics in anterior cruciate ligament reconstruction: a description of registries from six countries. Br J Sports Med 52:716–722
Renstrom P, Ljungqvist A, Arendt E, Beynnon B, Fukubayashi T, Garrett W et al (2008) Non-contact ACL injuries in female athletes: an International Olympic Committee current concepts statement. Br J Sports Med 42:394
Ridley TJ, Cook S, Bollier M, McCarthy M, Gao Y, Wolf B et al (2014) Effect of body mass index on patients with multiligamentous knee injuries. Arthroscopy 30:1447–1452
Ross BJ, Savage-Elliott I, Brown SM, Mulcahey MK (2020) Return to play and performance after primary ACL reconstruction in American football players: a systematic review. Orthop J Sports Med 8:2325967120959654
Sanders TL, Maradit Kremers H, Bryan AJ, Larson DR, Dahm DL, Levy BA et al (2016) Incidence of anterior cruciate ligament tears and reconstruction: a 21-year population-based study. Am J Sports Med 44:1502–1507
Sanders TL, Pareek A, Barrett IJ, Kremers HM, Bryan AJ, Stuart MJ et al (2017) Incidence and long-term follow-up of isolated posterior cruciate ligament tears. Knee Surg Sports Traumatol Arthrosc 25:3017–3023
Sandon A, Söderström T, Stenling A, Forssblad M (2021) Can talented youth soccer players who have undergone anterior cruciate ligament reconstruction reach the elite level? Am J Sports Med 49:384–390
Schulz MS, Russe K, Weiler A, Eichhorn HJ, Strobel MJ (2003) Epidemiology of posterior cruciate ligament injuries. Arch Orthop Trauma Surg 123:186–191
Shimozaki K, Nakase J, Takata Y, Shima Y, Kitaoka K, Tsuchiya H (2018) Greater body mass index and hip abduction muscle strength predict noncontact anterior cruciate ligament injury in female Japanese high school basketball players. Knee Surg Sports Traumatol Arthrosc 26:3004–3011
Snaebjörnsson T, Svantesson E, Sundemo D, Westin O, Sansone M, Engebretsen L et al (2019) Young age and high BMI are predictors of early revision surgery after primary anterior cruciate ligament reconstruction: a cohort study from the Swedish and Norwegian knee ligament registries based on 30,747 patients. Knee Surg Sports Traumatol Arthrosc 27:3583–3591
Svantesson E, Hamrin Senorski E, Kristiansson F, Alentorn-Geli E, Westin O, Samuelsson K (2020) Comparison of concomitant injuries and patient-reported outcome in patients that have undergone both primary and revision ACL reconstruction-a national registry study. J Orthop Surg Res 15:9
Uhorchak JM, Scoville CR, Williams GN, Arciero RA, Pierre PS, Taylor DC (2003) Risk factors associated with noncontact injury of the anterior cruciate ligament. Am J Sports Med 31:831–842
Winkler PW, Zsidai B, Narup E, Kaarre J, Horvath A, Sansone M et al (2022) Sports activity and quality of life improve after isolated ACL, isolated PCL, and combined ACL/PCL reconstruction. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-022-07060-w
Winkler PW, Zsidai B, Wagala NN, Hughes JD, Horvath A, Senorski EH et al (2021) Evolving evidence in the treatment of primary and recurrent posterior cruciate ligament injuries, part 1: anatomy, biomechanics and diagnostics. Knee Surg Sports Traumatol Arthrosc 29:672–681
Yang J, Tibbetts AS, Covassin T, Cheng G, Nayar S, Heiden E (2012) Epidemiology of overuse and acute injuries among competitive collegiate athletes. J Athl Train 47:198–204
Zsidai B, Horvath A, Winkler PW, Narup E, Kaarre J, Svantesson E et al (2022) Different injury patterns exist among patients undergoing operative treatment of isolated PCL, combined PCL/ACL, and isolated ACL injuries: a study from the Swedish National Knee Ligament Registry. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-022-06948-x
Acknowledgements
The authors would like to thank statistician Bengt Bengtsson from the Statistiska Konsultgruppen for help with performing the statistical analyses and giving advice regarding interpretation of data.
Funding
Open access funding provided by University of Gothenburg.
Author information
Authors and Affiliations
Contributions
All listed authors have contributed substantially to this work: literature review, and primary manuscript preparation were performed by JK, BZ, PWW, EN, and AH. KS, EHS, ES and VM assisted with interpretation of the results, initial drafting of the manuscript, as well as editing and final manuscript preparation. All authors read and approved the final manuscript to be published.
Corresponding author
Ethics declarations
Conflict of interest
Volker Musahl reports educational grants, consulting fees, and speaking fees from Smith & Nephew plc, educational grants from Arthrex and DePuy/Synthes, is a board member of the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS), and deputy editor-in-chief of Knee Surgery, Sports Traumatology, Arthroscopy (KSSTA). Kristian Samuelsson is a member of the Board of Directors in Getinge AB.
Ethical approval
This study was approved by the Swedish Ethical Review Authority (registration number: 2020-03559 and 2021-01002) and performed in accordance with the Declaration of Helsinki.
Informed consent
Participation in the Swedish National Knee Ligament Registry is voluntary for patients and surgeons and the registry complies with the Swedish legislation relating to data security. Therefore, no written consent is necessary for national databases in Sweden. Investigators had access only to unidentifiable patient data.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This study was performed at the Department of Orthopaedics, Institute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kaarre, J., Zsidai, B., Winkler, P.W. et al. Different patient and activity-related characteristics result in different injury profiles for patients with anterior cruciate ligament and posterior cruciate ligament injuries. Knee Surg Sports Traumatol Arthrosc 31, 308–315 (2023). https://doi.org/10.1007/s00167-022-07131-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-022-07131-y