
Abstract
Purpose
The aim of this study was to investigate gender-related differences in the sagittal curvature of the distal femoral condyle in the Korean osteoarthritic population
Methods
The sagittal curvatures of the distal femoral condyle of 1979 Korean patients (1680 female and 299 male) were evaluated using magnetic resonance imaging (MRI). MRI scans were obtained before total knee arthroplasty (TKA) in consecutive patients with end-stage osteoarthritis. The sagittal curvature of the distal medial and lateral femoral condyles was characterized with respect to the anterior, distal, and posterior circles. The diameter of each circle was measured. This study included 1873 varus and 106 valgus knees.
Results
The anterior, distal, and posterior diameters were significantly greater in the male patients than in the female patients (P < 0.05). In the male patients, the lateral diameter was significantly greater than the medial diameter in the anterior and posterior circles (P < 0.05). However, in the female patients, the lateral diameter was significantly greater only in the anterior circle. In both genders, the medial diameter was significantly greater than the lateral diameter of the distal circle (P < 0.05). For both the varus and valgus knees, the lateral diameter was greater than the medial diameter in the anterior circle.
Conclusions
It has been concluded that the sagittal curvature of the femoral condyles in females is significantly different to their male counterparts. This study provides a reliable evaluation of the sagittal curvature of the femoral condyle in the Korean population. These gender-related differences in the sagittal curvature of the femoral condyle may require further investigation to determine surgical implications such as in TKA, and the existence of gender-related dimorphism in specific knee injuries and pathologies, such as ligament injuries and tibiofemoral problems.
Level of evidence
III.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introductions
Accurate reproduction of the three-dimensional (3D) morphological relationships of knee joints aims to use the natural geometric and kinematic characteristics of the knee in the development of the total knee arthroplasty design [23]. The physiological requirements of the knee joints have significant variations between species, and kinematics are significantly influenced by the complex 3-D geometry of the distal femoral condyles [24].
Although 3-D models from individual subjects provide data for theoretical analysis, variations in individual anatomy have not been addressed [20]. Previous studies used a range of imaging modalities, including radiography and computed tomography, in which the hyaline cartilage was not shown, and measurements on cadavers, which may have undergone shrinkage and further destruction of each section of the bone specimen [10, 20]. Recently, considerable attention has been directed toward gender-related differences in TKA. New implant designs have been introduced to attribute for the anatomical differences between genders [4, 6, 18]. Geometric variations between Western male and female are well documented [14,15,16]. However, insufficient quantitative data have been reported on the geometric differences between the natural knees of male and female from the Asia–Pacific region. Yue et al. studied the geometry of the sagittal curvature of the distal femur in the Chinese population [28]. However, the limited cohort of sample was evaluated in their study without consideration of the cartilage due to the limitation of computed tomography (CT) [28]. In addition, knowing whether a difference exists between the diameter of the medial and lateral femoral condyles in both varus and valgus knees with osteoarthritis is important with regard to kinematics and the optimal 3-D alignment of the femoral component in TKA [3, 9]. If a clinically relevant asymmetry exists between the radii of the best-fit circles of the medial and lateral femoral condyles in varus and valgus osteoarthritic knees, accounting for this asymmetry may be necessary [21].
Therefore, the purpose of this study was to investigate a quantitative and unequivocal understanding of the distal femur morphology for clinical applications such as ligament reconstruction and TKA. It was hypothesized that gender-related differences exist in the sagittal curvature of the distal femoral condyle.
Materials and methods
In this study, the MRI scans of 2013 consecutive Korean patients who underwent TKA at our institution were retrospectively evaluated. The institutional review board (No.: 18-DR-02, Protocol No.: 3D-MRI according to sex_1.0) for this study approved the review of demographic data, radiographs, and MRI studies. Patients with poor function who showed a Kellgren–Lawrence grade 3 or 4 knee osteoarthritis who had undergone a primary TKA were included. Of the patients, 22 had a history of the previous surgery, 8 had a history of trauma, and 6 had a history of isolated patellofemoral arthritis of the knee joint and were excluded. 1979 patients, including 1680 female and 299 male patients, were included in the study. The varus–valgus angle was also measured between these axes, as shown in Fig. 1. The study consisted of 1873 varus and 106 valgus knees. The patient’s characteristics, such as age, gender, mechanical axis, and body mass index (BMI), are summarized in Table 1. The mean ages were 68.9 ± 6.6 and 69.2 ± 7.7, and years mean BMIs were 30.0 ± 3.1 and 29.6 ± 3.2 kg/m2 for the female and male patients, respectively (Table 1). No significant differences in patient demographics were found between the groups with respect to age and BMI.

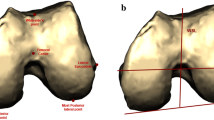
Schematic representation of a femur mechanical axis, transepicondylar axis, (b) sagittal diameter of the medial condyle (c), and sagittal diameter of the lateral condyle
The MRI scanning protocol was same as that used in a previous study [11, 12]. The MRI method used in the patient-specific instruments made it possible to develop 3-D reconstructed models effectively [21]. MRI scans were imported into the modeling software (Mimics version 17.0; Materialise, Leuven, Belgium) and segmented to develop 3-D femoral bony and cartilage models. The mechanical axis of the femur was first obtained by connecting the centers of the femoral head and intercondylar notch (Fig. 1a). The plane perpendicular to the mechanical axis was the transverse plane. The surgical transepicondylar axis was defined as the line between the lateral and medial epicondyles (Fig. 1a). The surgical transepicondylar axis was projected on the transverse plane, and the projected line was used as the x-axis. The coronal plane was defined using the mechanical axis and x-axis. The sagittal plane was defined as the plane perpendicular to the transverse and coronal planes. In the sagittal plane, the outer contours of the medial and lateral condyles were defined as three circles (Fig. 1b). Red, green, and blue circles denoted the anterior, posterior, and distal circles, respectively. The diameter of each circle was measured by a well-trained observer. To evaluate intraobserver and interobserver variabilities, 200 3-D MRI scans, 100 for the female patients and 100 for the male patients, were remeasured > 1 week after the initial measurements by the first and second observers. The intraobserver and interobserver errors were 0.87 and 0.92, respectively, as calculated using the intraclass correlation method.
Statistical analysis
The arithmetic means, standard deviations, and 95% confidence intervals were evaluated to describe the radii and demographic data. Statistical data were analyzed using SPSS (version 18.0, IBM, Chicago, IL, USA), and the Student’s t test was used to examine the significance of the differences between the genders. Paired t tests were used to examine the differences between the medial and lateral sides in the same gender. In addition, a paired Student’s t test was used to determine whether the radii of the medial and lateral femoral condyles differed between the varus and valgus knees. The differences were regarded as significant when the P value was < 0.05. A post hoc power analysis was performed in the anterior medial diameter between the two groups using G power 3.1. The alpha value was 0.05, and a statistical power was 100%. In the previous studies, the alpha value was 0.05 and the target power was 80% [7, 13]. In post hoc power test, the power was 0.98 with an alpha of 0.05 [19]. There is 100% power value which means that the sample size of this study was sufficient.
Results
The measured values related to the morphological parameters of the distal femoral condyle are summarized in Tables 2, 3, and 4. The anterior, distal, and posterior circles exhibited a normal distribution on the medial and lateral sides. The diameters of the anterior, distal, and posterior circles were significantly greater in the male patients than in the female patients (P < 0.05). The diameter of the anterior circle on the lateral side was significantly greater than that on the medial side (Table 2). However, the diameter of the distal circles was significantly greater on the medial side than on the lateral side.
The sagittal curvature of the femoral condyles was evaluated with respect to the femoral anteroposterior difference (Table 3). As the femoral anteroposterior size increased, the diameter of the sagittal curvature of the femoral condyles also increased.
In the 1873 varus knees, the mean diameter of the lateral posterior circle was 0.1 mm larger than that of the medial posterior circle (Table 4). In the group of 106 valgus knees, the mean diameter of the lateral posterior circle was 0.6 mm larger than that of the medial posterior circle (Table 5).
Discussion
The most important finding of this study was that a gender-related difference was found in the sagittal curvature of the distal femoral condyle. This study found that the sagittal curvature diameter of the distal femoral condyle was significantly smaller in the Korean female patients than in the male patients. The diameters of the anterior and posterior circle were significantly greater on the lateral side than on the medial side for male patients. However, the diameter of the distal circle on the lateral side was significantly smaller than that on the medial side in both genders. The diameter of the anterior circle was significantly greater on the lateral side than on the medial side in the female patients, but no significant difference was found in the posterior circle. In addition, the difference was not statistically significant in both the varus and valgus knees.
Previous studies showed that the surface of the distal femoral condyle is composed of two circular arcs: the distal circle in the extension facet and the posterior circle in the flexion facet [5, 16]. The knee kinematics from 20° ± 10° to full extension mainly occur at the distal circle, and flexion motion beyond 20° ± 10° occurs in the posterior circle. The results of most studies on the posterior circle were rather consistent [22, 26]; however, the measurements of the extension facets were variable. Some studies have reported that the radius of the lateral extension facet was larger than that of the medial facet [22], whereas others have proven otherwise [2, 16]. Asseln et al. showed that the lateral diameter was greater than the medial diameter in the posterior circle [1]. They showed that for the posterior circles, the lateral and medial diameters were 38.3 ± 5.1 and 34.6 ± 3.6 mm, respectively, in female patients and 42.6 ± 6.4 and 37.8 ± 4.3 mm, respectively, in male patients. Similar to their results, the results of the present study also showed that the diameter of the posterior circle in the male patients was greater than that in the female patients. However, the medial diameter was greater than the lateral diameter in the female patients in this study. These findings could be explained by the different cohorts and structural changes demonstrate in the femoral distal profile due to osteoarthritis. Siebold et al. reported that the medial and lateral diameters of the posterior circle were 43.2 ± 3.4 and 42.6 ± 3.6 mm, respectively, with no significant difference [24]. There was also no significant difference found in the posterior circle.
Yue et al. reported that the medial and lateral diameters of the posterior circle in male patients were 37.0 ± 2.8 and 39.4 ± 3.0 mm, respectively [28]. The lateral diameter was significantly greater than the medial diameter in the male patients [28]. In addition, the medial and lateral diameters of the posterior circle in female patients were 32.2 ± 1.2 and 33.0 ± 2.2 mm, respectively. They found no significant difference in the diameter of the posterior circle in the female patients, which showed good agreement with the results of this study [28]. The comparison of the diameter of the distal circle showed high deviations. In this study, the medial and lateral diameters of the distal circle were 73.3 ± 35.1 and 62.1 ± 14 mm, respectively, in the female patients and 79.8 ± 17.4 and 67.0 ± 14.6 mm, respectively, in the male patients. It was shown that the diameter of the lateral distal circle was significantly smaller than that of the medial side in both genders, showing good agreement with the previous studies [2, 16, 24, 28]. In addition, it was found that, for the anterior circle, the lateral diameter was greater than the medial diameter. Wang et al. reported that the lateral and medial diameters of the anterior circle were 51.0 ± 5.6 and 37 ± 6.5 mm, respectively, in male patients, and 53.2 ± 5.4 and 40.4 ± 6.0 mm, respectively, in female patients [27]. Similar to the findings of this study, their data showed that the lateral diameter was greater than the medial diameter, showing a gender-related difference. However, in their study, the diameter was greater in the female patients than in the male patients, which is contrary to our result. In general, many anatomical studies have shown that the diameter in female patients is smaller than that in male patients [28].
The relationship between the diameters of the medial and lateral femoral condyles in varus and valgus knees is important for femoral alignment and restoring kinematics in TKA. The two principal findings in this study were that the asymmetry between the diameters of the medial and lateral femoral posterior circles was small (0 < 2 mm) and that the association between these diameters was strong in both the varus and valgus knees. Accurate femoral positioning is challenging for even the most experienced arthroplasty surgeon, because arthritis distorts the knee surface, soft tissues conceal the articular surfaces, and conventional and navigational instruments lack precision [25]. The asymmetry between the diameters of the lateral and medial femoral condyles can be considered clinically unimportant in TKA, because it is relatively small compared with the cumulative error of positioning the femoral component in 6 degrees of freedom [8]. The small asymmetry between the diameters of the medial and lateral femoral condyles raises the question regarding the appropriate method for setting the rotation of the femoral component in valgus knees. External rotation of the femoral component has been recommended for valgus knees to compensate for the “hypoplasia” of the lateral femoral condyle. It can avoid internal rotation and reduce the risk of patellofemoral complications [17]. A previous study showed that the lateral femoral condyle is not hypoplastic with respect to the medial femoral condyle in a valgus knee [8]. Varus or valgus wear is unlikely caused by a difference in the diameter of the femoral posterior circle [8].
In terms of clinical relevance, the lateral femoral condyle is often assumed to have a “larger” diameter than the medial condyle, which is related to internal tibial rotation in flexion and the associated greater rollback of the lateral condyle than that of the medial condyle [28]. This impression can be attributed to the fact that the lateral condyle is longer than the medial condyle in the anteroposterior direction. However, the real functional area of the femoral condyle in terms of articulation with the tibia consists of the distal and posterior circles. The study showed that the diameter of the flexion facet was similar in both lateral and medial condyles, and the diameter of lateral extension facet was significantly smaller compared to the medial extension facet case [28]. Therefore, the condylar geometric shape may not be sufficient to evaluate the knee joint kinematics [28].
These results can be useful for the design and fabrication of more patient- or gender-specific TKA implants. Awareness of the gender-related differences in femoral morphology may help improve the implant designs for TKA. However, further evaluation is required to determine whether these design changes would improve clinical outcomes.
This study has some limitations. First, only Korean patients were examined. Future investigations should include other Asia–Pacific populations to establish a general data base for the population in this region. Second, MRI was used to develop the 3-D distal femur in this study, which may have led to errors in the computational model. Nevertheless, MRI allowed us to reconstruct soft tissues such as the articular cartilage, and the inaccuracy of the 3-D reconstruction could be reduced using a protocol described in our previous study [12]. Third, MRI was reassessed without a time interval to avoid the memory effect. Fourth, in the varus–valgus classification, no neutral coronal alignment group was contained. In this study, differences among the anterior, posterior, and distal sagittal diameters were focused between males and females. Thus, analysis on the relationship between sagittal diameter and alignment will be intended more intensively in further studies. Fifth, the influences of the femur and tibia on varus–valgus alignment were not compared. Using the joint-line convergence angle, the influences of the femur and tibia on varus–valgus alignment can be measured. However, the alignment is not the focus of this study, we will analyze it in further study.
Finally, although statistically significant differences were found in the morphology of the distal femur between the genders, further investigations are required to determine if each of these differences has any clinical impact. Anatomical, not functional, differences were investigated in the current present study.
Conclusions
This study found that the medial and lateral sagittal curvatures of the distal femoral condyle were asymmetrical, with gender-related differences in the Korean population. This study provides a reliable evaluation of the sagittal curvature of the femoral condyle in the Korean population. The results of the study are helpful to improve the understanding of knee joint kinematics and developing physiological knee prostheses. These gender-related differences in the sagittal curvature of the femoral condyle may require further investigation to determine surgical implications in, for example, TKA, and the gender-related dimorphism in specific knee injuries and pathologies, including ligament injuries and tibiofemoral problems.
References
Asseln M, Hanisch C, Schick F, Radermacher K (2018) Gender differences in knee morphology and the prospects for implant design in total knee replacement. Knee 25:545–558
Biščević M, Hebibović M, Smrke D (2005) Variations of femoral condyle shape. Coll Antropol 29:409–414
Blaha JD, Mancinelli CA, Simons WH (2002) Using the transepicondylar axis to define the sagittal morphology of the distal part of the femur. J Bone Joint Surg Am 84-A Suppl 2:48–55.
Conley S, Rosenberg A, Crowninshield R (2007) The female knee: anatomic variations. JAAOS 15:S31–S36
Freeman MA, Pinskerova V (2005) The movement of the normal tibio-femoral joint. J Biomech 38:197–208
Greene KA (2007) Gender-specific design in total knee arthroplasty. J Arthroplasty 22:27–31
Hoshino Y, Kuroda R, Nishizawa Y, Nakano N, Nagai K, Araki D et al (2018) Stress distribution is deviated around the aperture of the femoral tunnel in the anatomic anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 26:1145–1151
Howell SM, Howell SJ, Hull ML (2010) Assessment of the radii of the medial and lateral femoral condyles in varus and valgus knees with osteoarthritis. J Bone Joint Surg Am 92:98–104
Kessler O, Durselen L, Banks S, Mannel H, Marin F (2007) Sagittal curvature of total knee replacements predicts in vivo kinematics. Clin Biomech (Bristol, Avon) 22:52–58
Kettelkamp DB, Jacobs AW (1972) Tibiofemoral contact area–determination and implications. J Bone Joint Surg Am 54:349–356
Koh YG, Nam JH, Chung HS, Kim HJ, Chun HJ, Kang KT (2018) Gender differences in morphology exist in posterior condylar offsets of the knee in Korean population. Knee Surg Sports Traumatol Arthrosc 27:1628–1634
Koh YG, Nam JH, Chung HS, Lee HY, Kim HJ, Kim HJ et al (2019) Gender-related morphological differences in sulcus angle and condylar height for the femoral trochlea using magnetic resonance imaging. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-019-05423-4
Krych AJ, Johnson NR, Mohan R, Dahm DL, Levy BA, Stuart MJ (2018) Partial meniscectomy provides no benefit for symptomatic degenerative medial meniscus posterior root tears. Knee Surg Sports Traumatol Arthrosc 26:1117–1122
Lonner JH, Jasko JG, Thomas BS (2008) Anthropomorphic differences between the distal femora of men and women. Clin Orthop Relat Res 466:2724–2729
Mahfouz MR, Merkl BC, Fatah EE, Booth R Jr, Argenson JN (2007) Automatic methods for characterization of sexual dimorphism of adult femora: distal femur. Comput Methods Biomech Biomed Engin 10:447–456
Malek IA, Moorehead JD, Abiddin Z, Montgomery SC (2009) The correlation between femoral condyle radii and subject height. Clin Anat 22:517–522
Matsuda S, Miura H, Nagamine R, Mawatari T, Tokunaga M, Nabeyama R et al (2004) Anatomical analysis of the femoral condyle in normal and osteoarthritic knees. J Orthop Res 22:104–109
Merchant AC, Arendt EA, Dye SF, Fredericson M, Grelsamer RP, Leadbetter WB et al (2008) The female knee: anatomic variations and the female-specific total knee design. Clin Orthop Relat Res 466:3059–3065
Minami T, Muneta T, Sekiya I, Watanabe T, Mochizuki T, Horie M et al (2018) Lateral meniscus posterior root tear contributes to anterolateral rotational instability and meniscus extrusion in anterior cruciate ligament-injured patients. Knee Surg Sports Traumatol Arthrosc 26:1174–1181
Monk AP, Choji K, O'Connor JJ, Goodfellow JW, Murray DW (2014) The shape of the distal femur: a geometrical study using MRI. Bone Joint J 96-b:1623–1630
Nunley RM, Ellison BS, Zhu J, Ruh EL, Howell SM, Barrack RL (2012) Do patient-specific guides improve coronal alignment in total knee arthroplasty? Clin Orthop Relat Res 470:895–902
Nuño N, Ahmed A (2003) Three-dimensional morphometry of the femoral condyles. Clin Biomech 18:924–932
Rostlund T, Carlsson L, Albrektsson B, Albrektsson T (1989) Morphometrical studies of human femoral condyles. J Biomed Eng 11:442–448
Siebold R, Axe J, Irrgang JJ, Li K, Tashman S, Fu FH (2010) A computerized analysis of femoral condyle radii in ACL intact and contralateral ACL reconstructed knees using 3D CT. Knee Surg Sports Traumatol Arthrosc 18:26–31
Siston RA, Patel JJ, Goodman SB, Delp SL, Giori NJ (2005) The variability of femoral rotational alignment in total knee arthroplasty. J Bone Joint Surg Am 87:2276–2280
Siu D, Rudan J, Wevers HW, Griffiths P (1996) Femoral articular shape and geometry. A three-dimensional computerized analysis of the knee. J Arthroplasty 11:166–173
Wang J, Yue B, Wang Y, Yan M, Zeng Y (2012) The 3D analysis of the sagittal curvature of the femoral trochlea in the Chinese population. Knee Surg Sports Traumatol Arthrosc 20:957–963
Yue B, Varadarajan KM, Ai S, Tang T, Rubash HE, Li G (2011) Gender differences in the knees of Chinese population. Knee Surg Sports Traumatol Arthrosc 19:80–88
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Funding
No funding has been received for this study.
Ethical approval
Ethical approval was obtained by the institutional review board at the Yonsei Sarang Hostpital.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Koh, YG., Nam, JH., Chung, HS. et al. Gender difference exists in sagittal curvature of the distal femoral condyle morphology for osteoarthritic population. Knee Surg Sports Traumatol Arthrosc 28, 3740–3746 (2020). https://doi.org/10.1007/s00167-019-05769-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-019-05769-9