
Abstract
Purpose
To clarify the effect of longitudinal tears of the medial meniscus on the in situ meniscus force and the tibiofemoral relationship under axial load.
Methods
Twenty-one intact porcine knees were mounted on a 6-degrees of freedom robotic system, and the force and three-dimensional path of the knee joints were recorded during three cycles under a 250-N axial load at 30°, 60°, 90° and 120° of knee flexion. They were divided into three groups of seven knees with longitudinal tears in the middle to the posterior segment of the medial meniscus based on the tear site: rim, outer one-third and inner one-third of the meniscal body. After creating tears, the same tests were performed. Finally, all paths were reproduced after total medial meniscectomy, and the in situ force of the medial meniscus was calculated based on the principle of superposition.
Results
With a longitudinal tear, the in situ force of the medial meniscus was significantly decreased at 60°, 90° and 120° of knee flexion, regardless of the tear site. The decrement was greater with a tear in the meniscal body than a tear in the rim. A longitudinal tear in the meniscal body caused a significantly greater tibial varus rotation than a tear in the rim at all flexion angles.
Conclusion
Longitudinal tears significantly decreased the in situ force of the medial meniscus. Tears in the meniscal body caused a larger decrease of the in situ meniscus force and greater varus tibial rotation than tears in the rim.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The meniscus plays an important role in the knee joint such as load distribution and transmission, stabilisation, lubrication and shock absorption. Load distribution and transmission are important functions to protect the articular cartilage by increasing the contact area while decreasing contact pressure [1, 3, 18, 21]. Isolated meniscal tears are common among young athletes with high activity levels [26, 29]. Particularly, longitudinal tears (e.g., bucket-handle tears) of the medial meniscus have been frequently associated with articular cartilage lesions [19]. Biomechanical studies using human cadaveric knees have demonstrated that a longitudinal tear of the medial meniscus affects the strain and stress distribution on the circumferential fibres [15, 17], decreases the contact area and increases the pressure on the cartilage [21]. Measurement of the in situ force of the meniscus is clinically meaningful since the in situ force directly correlates with the meniscal function of load distribution and transmission under axial loads [25]. However, the effect of longitudinal tears on the in situ force of the medial meniscus is still unclear.
Stabilisation of the knee joint is another important meniscal function. Yoon et al. showed that varus malalignment in the lower extremity was aggravated after arthroscopic medial meniscectomy [30]. In a biomechanical study using human menisci, Allaire et al. described that a complete radial tear at the posterior root of the medial meniscus led to tibial external rotation and increased varus alignment under an axial load [1]. Accordingly, a loss of meniscal function may result in abnormal tibial rotation and stress concentration in a smaller contact area and, possibly, initiate the development of osteoarthritis [13, 28]. However, no studies have simultaneously investigated the effect of longitudinal tears in the medial meniscus on the tibiofemoral relationship as well as the in situ force of the meniscus under a compression load.
Most human cadaveric knees are obtained from elderly individuals frequently exhibiting degenerative changes in their menisci or cartilages. Porcine models are commonly used as alternative materials for human models because of anatomical similarity [14, 16], and using young porcine knees reduces the influence of these qualitative variations.
This experimental study using a porcine model aimed to clarify the effect of a longitudinal tear on the in situ force of the medial meniscus as well as the tibiofemoral relationship, depending on the tear site, using a porcine model. Our hypothesis was that the in situ force of the medial meniscus would be decreased and the varus rotation would be increased by the longitudinal tears in the medial meniscus, but the magnitude of these effects would be different, depending on the tear site. This is the first study to clarify the difference of the biomechanical effects due to the longitudinal tears depending on the tear sites, and the clinical relevance would be that when the longitudinal tears were repaired, postoperative rehabilitation programmes might be changed depending on the longitudinal tear sites.
Materials and methods
Twenty-one intact fresh frozen porcine knee joints were used in this study. The pigs were approximately 105 kg (range 100–105 kg) in weight with a mean age of 24 weeks (range 23–25 weeks). Specimens with any osteoarthritic changes or ligamentous injuries were excluded. The knees were frozen at − 30 °C and thawed at room temperature for 24 h before testing.
The tibia and femur were cut at a length of 150 mm from the joint line. The muscles, including the quadriceps muscle–patella–patellar tendon complex, were carefully removed from the joint, whereas the cruciate and collateral ligaments and capsule were left intact. The ends of the femur and tibia were potted in cylindrical moulds of acrylic resin (Ostron II; GC Corporation, Tokyo, Japan). The fibula was cut at a length of 50 mm from the proximal tibiofibular joint and fixed to the tibia to maintain its anatomical position using acrylic resin. To create longitudinal tears in the medial meniscus under a direct vision, a 40 × 40 × 5 mm osteotomy was performed at the femoral attachment area of the medial collateral ligament before testing, referring to the methodology in previous studies [3, 18] (Fig. 1). During the tests, the osteotomy site was rigidly bicortically fixed with two cancellous screws. A pilot study using four samples was conducted to evaluate the biomechanical effect of the osteotomy, and it was confirmed that the osteotomy did not result in a significant change in the in situ force of the medial meniscus or tibiofemoral relationship (Table 1). Thus, the knee after rigid screw fixation of the osteotomy site was regarded as the intact knee in this study.

Knee specimen. a A 40 mm × 40 mm × 5 mm osteotomy at the femoral insertion of medial collateral ligament was performed to create longitudinal tears in the medial meniscus under direct vision without compromising the medial collateral ligament complex. a′ Schema of a. b During the tests, the osteotomy site was rigidly bicortically fixed with two cancellous screws of 70 mm in length and 4 mm in diameter. To minimize the rotation and displacement of the osteotomy site in testing conditions, the edges of the osteotomy site and the original bone were carefully aligned during screw fixation. b′ Schema of b. MCL medial collateral ligament
Equipment
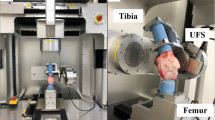
The femoral and tibial cylinders of the porcine knees were fixed to the clamps of the manipulator of a robotic simulator [5,6,7,8] (Fig. 2). The robotic simulator system consisted of a 6-degrees of freedom manipulator consisting of three translational/rotational actuators, servo-motor controllers, a 6-degrees of freedom universal force/moment sensor (UFS), and a control computer [5,6,7,8,9,10, 22, 23, 25]. The maximum clamp-to-clamp compliance with the knee extended was 321 N/mm in the medial–lateral direction, 424 N/mm in the anterior–posterior direction, and 814 N/mm in the proximal–distal direction [10]. The force sensor resolution was 0.01–0.02 N for forces and 0.001 N m for torques [10, 25]. The test–retest reliability of this robotic system was ± 0.006 mm in translation and ± 0.03° in rotation for reproducing the paths [10, 25]. Force control fluctuations were < 5 N in force and < 0.2 Nm in moment. According to previous studies [5,6,7,8,9,10, 22, 23, 25], the knee joint coordinate system was defined with respect to the non-orthogonal mechanism proposed by Grood and Suntay [11]. Data acquisition was performed at a rate of 17–20 Hz [9].

Six-degrees of freedom robotic system. The femur was fixed to the lower mechanism, while the tibia was fixed to the upper mechanism via a universal force/moment sensor
Test protocols
For preconditioning, the specimens were initially subjected to three cycles of passive extension-flexion between 20° and 130° to exclude the influence of creep behaviour of the viscoelastic soft tissues. Then, the simulator applied an axial load from 0 to 250 N at a rate of 0.08 mm/s for three cycles at 30°, 60°, 90°, and 120° of knee flexion, simulating that a 100-kg pig stands on four legs. The three-dimensional (3-D) path of knee motion (P1) and the forces on the knee in the three directions (F1) during the three cycles of the axial loading tests were recorded via the UFS. After these initial tests, the fixation screws were removed and approximately 30-mm longitudinal tears were created from the middle to the posterior segment of the medial meniscus under a direct vision. In this procedure, they were divided into three groups depending on the tear sites: (1) the rim, (2) the outer one-third of the meniscal body, and (3) the inner one-third of the meniscal body (Fig. 3). The three groups consisted of seven knees respectively. Next, the osteotomy site was rigidly refixed with the screws and the same tests were performed. The 3-D path of the knee motion (P2) and the forces on the knee in the three directions (F2) were again recorded via the UFS. Then, the screws were removed again, the medial meniscus was totally removed, and the osteotomy site was rigidly refixed with the screws. The simulator reproduced all the identical paths previously obtained (P1 and P2) while the forces F1′ and F2′ were recorded. Based on the principle of superposition [6], the in situ force of the medial meniscus in the intact state (FMM intact) and that with the longitudinal tear (FMM tear) was calculated in all the three cycles of the axial load from 0 to 250 N (Fig. 4). Of all the obtained data, those under axial loads of 50, 150, and 250 N at the third cycle, respectively, were used for the analysis. Accordingly, the in situ force of the meniscus was defined as the resultant force that the meniscus carries in response to a load applied to the knee joint [2, 25]. Regarding the tibiofemoral relationship, the alternation of the tibial position and rotation as a result of the longitudinal meniscal tear was assessed by comparing the paths in the intact state (P1) with those in the injured state (P2). The paths were further compared between the three different meniscal tear sites during the third cycle under an axial load of 250 N. Before conducting the experiments, the study protocol was meticulously reviewed by the ethical committee of Osaka University and it was determined that this experimental study did not require the approval of the institutional review board, since all the knee specimens were obtained from edible pigs.

Schema of longitudinal tear sites in the middle to posterior segment of medial meniscus. (1) Rim, (2) outer third of meniscal body, (3) inner third of meniscal body. ACL anterior cruciate ligament, PCL posterior cruciate ligament, MM medial meniscus, LM lateral meniscus

Flowchart of testing protocol and acquired data. MM medial meniscus
Statistical analysis
All statistical tests were performed using JMP software version 13.0.0 (SAS Institute Inc., Cary, NC, USA). For a power analysis with a power of 0.8 and an α of 0.05, it was determined that six knee specimens were required for comparison of a 16% difference with an SD of ± 8% of the decrement of the in situ force of the medial meniscus. Thus, the sample size of seven knee specimens in each of the three meniscal tear groups in this study was acceptable. The paired t test was used to compare the in situ force of the medial meniscus between the intact state and the injured state with the longitudinal tear. In the comparison of the three meniscal tear sites, a two-factor repeated-measures analysis of variance was used for the factors of flexion angles and longitudinal tear sites (rim, outer third and inner third). A post hoc test for multiple comparisons was performed using the Tukey honestly significant difference test. P < 0.05 was considered statistically significant.
Results
In situ force of medial meniscus
With a longitudinal tear, the in situ force of the medial meniscus was significantly decreased in comparison to the force in its intact state at 60°, 90°, and 120° of knee flexion, regardless of the meniscal tear site (Table 2; Fig. 5). Regarding the effect of the tear site, the decrement of the in situ force of the medial meniscus was significantly greater in the group with a tear in the outer one-third of the meniscal body than that in the group with a tear in the rim under all testing conditions except for in 30° of knee flexion under an axial load of 50 N (Fig. 6).

In situ force of medial meniscus. a 30° of knee flexion, b 60° of knee flexion, c 90° of knee flexion, d 120° of knee flexion. *P < 0.05 (significant difference between the in situ force of the intact meniscus and that with a longitudinal tear)

Decrement of in situ force of medial meniscus due to longitudinal tear. a 50-N axial load, b 150-N axial load, c 250-N axial load. *P < 0.05
Tibiofemoral relationship
A longitudinal tear in the outer or inner third of the meniscal body caused a significantly greater tibial varus rotation than a tear in the rim at all flexion angles under a 250-N axial load (Table 3). The results were similar under 50 and 150-N axial loads as well.
Discussion
The principal findings of this study using a porcine model were that (1) a longitudinal tear decreased the in situ force of the medial meniscus and (2) a longitudinal tear in the meniscal body had a greater effect on the in situ force and tibial rotation than a tear in the rim.
The meniscus has important roles in the knee joint, such as lubrication, stabilisation and load distribution and transmission. When the meniscus is injured, other knee structures including the articular cartilage can be consecutively affected. There were some studies investigating the biomechanical effect of a longitudinal tear of the medial meniscus in a human model [15, 17, 20, 21]. Muriuki et al. clarified the effect of a longitudinal tear of the medial meniscus on the articular cartilage using pressure film sensors, and demonstrated that a 15–20-mm longitudinal tear in the outer third of the posterior segment of the meniscus caused an increase of contact pressure and a decrease of the contact area under an axial load of 1000 N [21]. Kedgley et al. assessed the stress distribution along the inner and outer surfaces of longitudinal tears using finite-element models and reported that the edge was pulled apart under a 1000-N axial load when a 14-mm unstable longitudinal tear was created in the red–white zone [17]. However, no studies have directly assessed the effect of a longitudinal tear on meniscal function of load distribution and transmission. Using a porcine model, this study first showed that approximately 30-mm longitudinal tears significantly decrease the in situ force of the medial meniscus in 60°, 90°, and 120° of knee flexion under compressive loads, regardless of the tear sites. Therefore, a longitudinal tear in the middle to the posterior segment of the meniscus significantly affects the meniscal function of load distribution and transmission.
According to previous studies using a human model, compressive loads create a gap on the meniscus with a longitudinal tear in the meniscal body [4, 17, 20]. McCullough et al. measured the gap at the site of a longitudinal tear in the red–white zone of the middle to the posterior segment of the medial meniscus under simulated gait conditions and demonstrated that the tear edges were moving independently in the vertical direction and were likely unstable during the toe-off phase [20]. In our study, the biomechanical effects of the different sites of the longitudinal tears were initially compared using a porcine model, and it was demonstrated that tears in the meniscal body cause a greater decrease of the in situ force as well as greater tibial varus rotation than tears in the rim. Thus, the tear site might open under a compressive axial load and consequently cause a greater decrease of the meniscal function in the meniscal body compared with a tear in the rim. In contrast, the effects will be smaller in the case of a tear in the rim because the circumferential fibres in the meniscal body are not impaired. In summary, the clinical relevance of this study using a porcine model is that the meniscal function of load distribution and transmission is decreased with a longitudinal tear in the middle to posterior segment, especially when the tear involves the meniscal body. According to the present results, postoperative rehabilitation programmes after meniscal repair might be changed depending on the longitudinal tear sites. For the tear in the rim, weight-bearing exercise could be started earlier because the tear had a smaller effect on the in situ force. On the contrary, for the tear in the meniscal body, more protective rehabilitation programmes might be recommended since it would be expected that the load on the sutures is higher under axial loads.
There are some limitations in this study. First, it was difficult to simply transfer the conclusions to human knees, since the difference in meniscal stiffness might influence the in situ force of the meniscus in the intact state as well as in the injured states [24]. However, most of the human cadaveric knees are obtained from elderly individuals and frequently exhibit degenerative changes in their menisci or cartilages. Therefore, to reduce the influence of these qualitative variations, young porcine knees with anatomical similarity to human knees [14, 16] were used in this experimental study. Second, the magnitude of the axial load applied in this study might have been comparably small. An axial load of 250 N is equivalent to the load on the knee joint when standing on four legs. The biomechanical effect of a meniscal tear with higher axial loads simulating daily activities, such as squatting or running, will be further investigated in future studies. Third, the biomechanical effect of a longitudinal tear of 30 mm in length from the middle to the posterior segment of the medial meniscus was evaluated. This tear length was expected to be adequate to yield clinically significant findings in this experimental study, as some clinical studies showed that the healing rate after meniscal repair was significantly lower for longitudinal tears with a length of more than 20–25 mm [12, 27]. However, it would be interesting to identify the threshold of tear length that significantly affects the meniscal load distribution and transmission.
Conclusion
In a porcine model, longitudinal tears significantly decrease the in situ force of the medial meniscus. Tears in the meniscal body cause a larger decrease of the in situ force and greater varus rotation than tears in the rim.
Abbreviations
- 3-D:
-
Three-dimensional
- UFS:
-
Universal force/moment sensor
References
Allaire R, Muriuki M, Gilbertson L, Harner CD (2008) Biomechanical consequences of a tear of the posterior root of the medial meniscus: similar to total meniscectomy. J Bone Joint Surg Am 90(9):1922–1931
Allen CR, Wong EK, Livesay GA, Sakane M, Fu FH, Woo SL (2000) Importance of the medial meniscus in the anterior cruciate ligament-deficient knee. J Orthop Res 18(1):109–115
Bedi A, Kelly NH, Baad M, Fox AJ, Brophy RH, Warren RF, Maher SA (2010) Dynamic contact mechanics of the medial meniscus as a function of radial tear, repair, and partial meniscectomy. J Bone Joint Surg Am 92(6):1398–1408
Dürselen L, Hebisch A, Claes LE, Bauer G (2003) Gapping phenomenon of longitudinal meniscal tears. Clin Biomech (Bristol, Avon) 18(6):505–510
Fujie H, Mabuchi K, Woo SL-Y, Livesay GA, Arai S, Tsukamoto Y (1993) The use of robotics technology to study human joint kinematics: a new methodology. J Biomech Eng 115(3):211–217
Fujie H, Livesay GA, Woo SLY, Kashiwaguchi S, Blomstrom G (1995) The use of a universal force-moment sensor to determine in situ forces in ligaments: a new methodology. J Biomech Eng 117(1):1–7
Fujie H, Livesay GA, Fujita M, Woo SLY (1996) Forces and moments in 6-DOF at the human joint: mathematical description for control. J Biomech 29(12):1577–1585
Fujie H, Sekito T, Orita A (2004) A novel robotic system for joint biomechanical tests: application to the human knee joint. J Biomech Eng 126(1):54–61
Fujie H, Otsubo H, Fukano S, Suzuki T, Suzuki D, Mae T, Shino K (2011) Mechanical functions of the three bundles consisting of the human anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc 19(Suppl 1):S47–S53
Fujie H, Kimura K, Yamakawa S (2013) Static and dynamic properties of a 6-DOF robotic system for knee joint biomechanics study. ASME Summer Bioeng Conf. https://doi.org/10.1115/SBC2013-14849
Grood ES, Suntay WJ (1983) A joint coordinate system for the clinical description of three-dimensional motions: application to the knee. J Biomech Eng 105(2):136–144
Haklar U, Donmez F, Basaran SH, Canbora MK (2013) Results of arthroscopic repair of partial- or full-thickness longitudinal medial meniscal tears by single or double vertical sutures using the inside-out technique. Am J Sports Med 41(3):596–602
Hosseini A, Van de Velde SK, Gill TJ, Li G (2012) Tibiofemoral cartilage contact biomechanics in patients after reconstruction of a ruptured anterior cruciate ligament. J Orthop Res 30(11):1781–1788
Jaspers P, Lange A, Huiskes R, van Rens T (1980) The mechanical function of the meniscus experiments on cadaveric pig knee-joints. Acta Orthop Belg 46(6):663–668
Jones RS, Keene GC, Learmonth DJ, Bickerstaff D, Nawana NS, Costi JJ, Pearcy MJ (1996) Direct measurement of hoop strain in the intact and torn human medial meniscus. Clin Biomech 11(5):295–300
Joshi MD, Suh JK, Marui T, Woo SL (1995) Interspecies variation of compressive biomechanical properties of the meniscus. J Biomed Mater Res 29(7):823–828
Kedgley AE, Saw TH, Segal NA, Hansen UN, Bull AMJ, Masouros SD (2019) Predicting meniscal tear stability across knee-joint flexion using finite-element analysis. Knee Surg Sports Traumatol Arthrosc 27(1):206–214
Lee SJ, Aadalen KJ, Malaviya P, Lorenz EP, Hayden JK, Farr J, Kang RW, Cole BJ (2006) Tibiofemoral contact mechanics after serial medial meniscectomies in the human cadaveric knee. Am J Sports Med 34:1334–1344
Lewandrowski KU, Müller J, Schollmeier G (1997) Concomitant meniscal and articular cartilage lesions in the femorotibial joint. Am J Sports Med 25(4):486–494
McCulloch PC, Jones HL, Hamilton K, Hogen MG, Gold JE, Noble PC (2016) Does simulated walking cause gapping of meniscal repairs? J Exp Orthop 3(1):11
Muriuki MG, Tuason DA, Tucker BG, Harner CD (2011) Changes in tibiofemoral contact mechanics following radial split and vertical tears of the medial meniscus an in vitro investigation of the efficacy of arthroscopic repair. J Bone Joint Surg Am 93(12):1089–1095
Ohori T, Mae T, Shino K, Tachibana Y, Fujie H, Yoshikawa H, Nakata K (2017) Varus-valgus instability in the anterior cruciate ligament-deficient knee: effect of posterior tibial load. J Exp Orthop 4(1):24
Ohori T, Mae T, Shino K, Tachibana Y, Fujie H, Yoshikawa H, Nakata K (2019) Complementary function of the meniscofemoral ligament and lateral meniscus posterior root to stabilize the lateral meniscus posterior horn: a biomechanical study in a porcine knee model. Orthop J Sports Med 7(1):2325967118821605
Stärke C, Lohmann CH, Kopf S (2018) Stiffness of meniscus tissue depends on tibio-femoral load and structural integrity of the meniscus root. Proc Inst Mech Eng H 232(4):418–422
Tachibana Y, Mae T, Fujie H, Shino K, Ohori T, Yoshikawa H, Nakata K (2017) Effect of radial meniscal tear on in situ forces of meniscus and tibiofemoral relationship. Knee Surg Sports Traumatol Arthrosc 25(2):355–361
Terzidis IP, Christodoulou A, Ploumis A, Givissis P, Natsis K, Koimtzis M (2006) Meniscal tear characteristics in young athletes with a stable knee: arthroscopic evaluation. Am J Sports Med 34(7):1170–1175
Uchio Y, Ochi M, Adachi N, Kawasaki K, Iwasa J (2003) Results of rasping of meniscal tears with and without anterior cruciate ligament injury as evaluated by second-look arthroscopy. Arthroscopy 19(5):463–469
Van de Velde SK, Bingham JT, Hosseini A, Kozanek M, DeFrate LE, Gill TJ, Li G (2009) Increased tibiofemoral cartilage contact deformation in patients with anterior cruciate ligament deficiency. Arthritis Rheumatol 60(12):3693–3702
Yeh PC, Starkey C, Lombardo S, Vitti G, Kharrazi FD (2012) Epidemiology of isolated meniscal injury and its effect on performance in athletes from the National Basketball Association. Am J Sports Med 40(3):589–594
Yoon KH, Lee SH, Bae DK, Park SY, Oh H (2013) Does varus alignment increase after medial meniscectomy? Knee Surg Sports Traumatol Arthrosc 21(9):2131–2136
Acknowledgements
The authors thank Mr Yukiya Shibata for technical support with the use of the 6-degrees of freedom robotic system. This work is supported by a grant from Japan Society for the Promotion of Science, JSPS KAKENHI Grant Number JP26462293.
Funding
This work was founded by a grant from Japan Society for the Promotion of Science, JSPS 199 KAKENHI Grant Number JP26462293.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with animals performed by any of the authors because all the knee specimens were obtained from edible pigs from the local butcher.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Tachibana, Y., Mae, T., Shino, K. et al. A longitudinal tear in the medial meniscal body decreased the in situ meniscus force under an axial load. Knee Surg Sports Traumatol Arthrosc 28, 3457–3465 (2020). https://doi.org/10.1007/s00167-019-05735-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-019-05735-5