
Abstract
Purpose
Anterior cruciate ligament (ACL) reconstruction using a bone–patellar tendon–bone (BTB) graft is known to provide secure fixation due to the direct bone-to-bone integration of the bone plug and bone tunnel. It is important to know the time required for bone integration when designing the postoperative rehabilitation protocol or deciding when the patient can return to competition-level activity, especially if the patient is an athlete. However, because reports are scarce, the period necessary for bone-to-bone integration after ACL reconstruction using a BTB graft remains unclear. The purpose of this study was to clarify this issue. It was hypothesised that ACL reconstruction using a BTB graft via an anatomical rectangular tunnel would help in the integration between bone plugs and bone tunnels on both the femoral and tibial sides after at least 6 months, at which point basic exercises similar to pre-injury sporting activity levels can be resumed.
Methods
This study included 40 knees treated with ACL reconstruction using a BTB graft via anatomical rectangular tunnel reconstruction between 2013 and 2014 in a single institute. The integration between bone plugs and bone tunnels was evaluated using multi-slice tomosynthesis, which is a technique for producing slice images using conventional radiographic systems, at 1, 3, and 5 months postoperatively. All procedures were performed by two experienced surgeons. Bone integration was evaluated by two orthopaedic doctors.
Results
The rates of integration of the bone plug and femoral bone tunnel on tomosynthesis at 1, 3, and 5 months postoperatively were 0, 55, and 100%, respectively. On the tibial side, the corresponding rates were 0, 75, and 100%, respectively. The rate of integration on the tibial side was significantly higher than that on the femoral side at 3 months postoperatively (p = 0.031).
Conclusions
Bone-to-bone integration on the femoral and tibial sides was complete within 5 months after surgery in all cases. Since the time required for bone integration is important in designing the postoperative rehabilitation approach, these results will serve as a useful guideline for planning rehabilitation protocols.
Level of evidence
IV.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Secure fixation between the tendon graft and bone tunnel is one of the principal determinants of successful anterior cruciate ligament (ACL) reconstruction [8, 10, 25, 36, 37]. Among the various tendon grafts considered suitable for this repair, hamstring and patellar tendons are the most popular [9, 14, 16, 26, 33, 34, 38]. The mechanism of healing between the tendon graft and the bone tunnel in bone-attached tendons is distinct from that in bone-free tendons. Bone-free tendons anchor to the bone wall via newly formed collagen fibres that resemble Sharpey’s fibres [18, 25, 39]. In contrast, ACL reconstruction with bone–patellar tendon–bone (BTB) grafts provides good fixation due to the direct bone-to-bone integration involved [4, 5, 17, 22]. However, because previous reports are scarce, the period necessary for bone-to-bone integration after BTB ACL reconstruction is unknown.
ACL reconstruction using a BTB graft via an anatomical rectangular tunnel (also known as anatomical rectangular tunnel BTB ACL reconstruction) is a novel surgical technique reported by Hayashi et al. [13], Mae et al. [20] and Shino et al. [27,28,29]. In this procedure, the BTB graft was positioned, such that it mimicked the natural fibre arrangement of a normal ACL according to the concepts of anatomic reconstruction. Suzuki et al. reported early integration of the bone plug in the femoral tunnel in anatomical rectangular tunnel BTB ACL reconstruction using an interference screw for graft fixation on the femoral side [30]. Suspensory fixation devices were used on the femoral side during anatomical rectangular tunnel BTB ACL reconstruction at the study centre. However, the exact period required for bone plug and tunnel integration in anatomical rectangular tunnel BTB ACL reconstruction when using a suspensory button for femoral side fixation is still unknown. Understanding the time required for integration between the tendon bone plug and bone tunnel is important in designing the postoperative rehabilitation protocol or timing the return to competition-level activity, especially in athletes.
With the above in mind, the aim of this study was to assess the time required for integration between bone plugs and bone tunnels following anatomical rectangular tunnel BTB ACL reconstruction with suspensory devices for fixation on the femoral side and a double spiked plate (DSP) system (MEIRA Corp., Nagoya, Japan) and screw for fixation on the tibial side. The DSP system is a modified pull-out suture technique that makes it possible to fix the graft under a predetermined amount of tension [29].
It was hypothesised that anatomical rectangular tunnel BTB ACL reconstruction would help in the integration between bone plugs and bone tunnels on both the femoral and tibial sides after at least 6 months, at which point basic exercises similar to pre-injury sporting activity levels can be resumed. The method of postoperative rehabilitation after ACL reconstruction has not yet been established due to a lack of data [2, 35]. If it becomes clear that bone-to-bone integration is complete within 6 months after the procedure, this knowledge will serve as a basis for discussions on rehabilitation protocols after ACL reconstruction. As a result, this study confirmed that the use of the investigated rehabilitation protocols yielded reasonable times of return to basic exercises that were similar to pre-injury sporting activity levels.
Materials and methods
Patients with isolated ACL injuries and ACL injuries with concomitant meniscal tears were included in this study. Patients with multiple ligament injuries and those undergoing revision ACL were excluded. All reconstructions were performed by two experienced surgeons. Bone integration was assessed by two orthopaedic doctors using tomosynthesis. Tomosynthesis is a technique for producing slice images using conventional radiographic systems. It is a special type of imaging technology that fuses cone-beam computed tomography (CT) reconstruction with digital image processing to produce images of specified cross sections from a single tomography. Tomosynthesis has a shorter examination time, less metal equipment-related artefacts, and less radiation dose compared to CT.
Surgical technique
All patients underwent anatomical rectangular tunnel BTB ACL reconstruction with tourniquet control under general anaesthesia [27,28,29]. Arthroscopy was performed to identify meniscal tears; if a meniscal tear was present, a repair or meniscectomy was performed. For fixation, a 4 × 12-mm EndoButton (Smith & Nephew, Inc., Andover, MA, USA) was secured to the femoral bone plug using two #2 FiberWires (Arthrex, Inc., Naples, FL, USA) to enable placement of the distal end of the bone plug at the aperture of the femoral tunnel. Two leading sutures were used to pass the graft from the tibial tunnel to the femoral socket while maintaining the cancellous bone surface anteriorly. Femoral fixation was achieved with an EndoButton using the flip technique, and tibial fixation was performed using a DSP system with the pull-out suture technique [32] (Fig. 1).

Schema of anterior cruciate ligament reconstruction using a bone–patellar tendon–bone graft via an anatomical rectangular tunnel. Reconstruction was performed with an EndoButton for femoral fixation, while tibial fixation was achieved with a double spiked plate and screw
Radiographic analysis
All patients were evaluated via multi-slice tomosynthesis (SONIALVISION safire; Shimadzu, Co., Kyoto, Japan) at 1, 3, and 5 months postoperatively. Reconstructed imaging data provided cross-sectional coronal and sagittal images in 1-mm slices. Bone integration was evaluated from the femoral and tibial sides in the sagittal and coronal views, respectively. Bone integration was considered complete when trabecular continuity between the bone plug and the adjacent wall of the bone tunnel was observed in at least two consecutive slices (Fig. 2). The bone was considered as integrated only if the two orthopaedic doctors, who did not perform the procedures, agreed on the findings. The inter-observer reliability between the orthopaedic doctors who evaluated the tomosynthesis findings was κ = 0.82, while the intra-observer reliability was κ = 0.89.

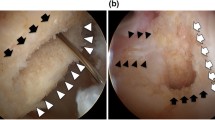
Tomosynthesis for the evaluation of bone integration. (a, b) Bone plug was separated from the bone socket, and was considered as not integrated. (c, d) Bone plug contacted the bone socket and continuity of the trabecular bone was observed; therefore, it was considered as integrated
The institutional review board of Teikyo University in Tokyo, Japan approved this study (ID17036). All patients were informed about the procedure and provided consent for participation in the study and for the publication of their data.
Statistical analyses
All statistical analyses were performed with SPSS version 21 (IBM, Co., Armonk, NY, USA). Fisher’s exact test was used to analyse the differences between bone integration at the femoral tunnel and the tibial tunnel. The κ statistic was used to analyse inter-observer and intra-observer reliability. Based on this protocol’s pilot study, it was assumed that the rate of integration at 3 months after the operation would be 80% on the tibial side and 50% on the femoral side. Thirty-seven patients were needed to establish a significant difference for integration on the tibial side and the femoral side with 80% power at a 2.5% one-sided significance level.
Results
Forty-nine knees were treated using anatomical rectangular tunnel BTB ACL reconstruction between 2013 and 2014 at Teikyo University Hospital. Two knees were excluded, because revision ACL was performed and five knees were excluded, because the patients were unable to undergo three tomosynthesis assessments at the appropriate time points. Finally, 40 knees (14 women and 26 men) were eligible for analysis. The median patient age at the time of surgery was 20.5 years (range 16–49 years). Other preoperative patient characteristics are shown in Table 1.
The rates of integration of the bone plug with the femoral bone tunnel on tomosynthesis at 1, 3, and 5 months postoperatively were 0, 55, and 100%, respectively (Fig. 3). On the tibial side, the corresponding rates were 0, 75, and 100%, respectively (Fig. 4). The bone plugs were integrated with the bone tunnels on the femoral and tibial sides by postoperative month 5 in all patients. The rate of integration was higher on the tibial side than on the femoral side at 3 months postoperatively (p = 0.031; Fig. 5), suggesting that bone integration on the tibial side occurred earlier.

Bone integration on the femoral side. a Bone integration rates on the femoral side at 1, 3, and 5 months after surgery. b Sagittal-plane tomosynthesis on the femoral side. Bone integration was negative at 1 month after surgery. c Bone plug was integrated at 5 months after surgery

Bone integration on the tibial side. a Bone integration rates on the tibial side at 1, 3, and 5 months after surgery. b Coronal-view tomosynthesis on the tibial side. Bone integration was negative at 1 month after surgery. c Bone plug was integrated at 5 months after surgery

Bone integration rates on the femoral and tibial sides at 3 months after surgery. The bone integration rate was significantly higher on the tibial side than on the femoral side
Discussion
The principal finding of this study was that the integration of the bone plugs of the tendon graft with the femoral bone tunnel and the tibial bone tunnel occurred within 5 months in all patients following anatomical rectangular tunnel BTB ACL reconstruction with suspensory fixation. Bone integration on the femoral side was slower than previously reported, wherein bone plug-femoral tunnel integration occurred within 8 weeks of the anatomical rectangular tunnel BTB ACL reconstruction procedure [30]. In the previous study, interference screws were used for femoral side fixation, and bone integration was evaluated using CT. Additionally, the researchers suggested that earlier bone integration may be attributed to the type of fixation used. However, Lomasney et al. performed conventional round tunnel allograft BTB ACL reconstruction with bioabsorbable interference screws for fixation and reported bone plug-tibial bone tunnel integration in only 34.5% of cases at 5 months postoperatively [17]. The shape of the bone tunnels and the sensitivity of the imaging method used for the assessment of integration may explain the difference in bone healing time between these studies and the current study.
Kawakami et al. studied the integration of tendons into bone tunnels by comparing bone-attached tendon grafts with interference screw fixation and bone-free tendon grafts with extra-articular suture fixation [15]. In this previous study involving anterior half replacement of the medial collateral ligament in Japanese white rabbits, the two interventional groups were found to be comparable in terms of biomechanical characteristics in the early postoperative period. This result confirmed that EndoButtons were not inferior to interference screws for femoral fixation in experimental animal models. However, the efficacy of suspensory buttons for femoral fixation in anatomical rectangular tunnel BTB ACL reconstruction has not been confirmed in clinical settings [3, 24]. Recently, Taketomi et al. reported bone plug integration with a femoral socket within 1 year of anatomical rectangular tunnel BTB ACL reconstruction with EndoButtons for femoral side fixation in all cases [31]. The authors also reported that EndoButton use was associated with a low incidence of bone plug migration, short mean distance of bone plug migration, satisfactory short-term clinical outcomes, and low complication rates. These previous conclusions were consistent with the results of this study.
The use of tomosynthesis instead of CT or magnetic resonance imaging to evaluate the integration of bone plugs with bone tunnels is unique to the present study. The advantages of using tomosynthesis are as follows: (1) tomosynthesis has a shorter examination time, thus improving patient comfort; (2) the influence of metal equipment-related artefacts is lessened with tomosynthesis, enabling reliable evaluation of bone integration [6, 7, 19]; and (3) tomosynthesis has been associated with lower radiation doses than CT [1, 21, 23], making it safer for frequent or repeated imaging. Ha et al. reported that tomosynthesis provided superior diagnostic information compared with other imaging methods in the postoperative evaluation of wrist fractures, and was associated with lower costs and radiation exposure than CT [12]. The authors of this previous study recommended that tomosynthesis should be considered for the follow-up imaging of fractures.
The evaluation of bone integration performed on the femoral side, as well as on the tibial side, was another strength of the current study, which was in contrast to most other studies that only evaluated the femoral side [30, 31]. This enabled this investigation to identify a significant difference in the rate of bone integration between the femoral and tibial sides. There are several possible reasons for this difference. First, healing may be faster on the tibial side due to differences in the residual cancellous bone on the bone plugs. Most of the cancellous bone on the femoral bone plug was shaved off to achieve a rectangular shape, in contrast to the bone plug on the tibial side. Second, the method of fixation was different between the two sites. EndoButtons were used as suspensory devices on the femoral side, while a DSP and screws were used on the tibial side. Third, the femoral tunnel may be subjected to greater mechanical stress due to longitudinal motion of the graft (bungee effect) [11], which may prolong bone integration time on the femoral side.
Follow-up assessment revealed that bone integration at either end of the tendon graft was complete within 5 months after surgery. These results indicate the need to reconsider the protocol for rehabilitation following anatomical rectangular tunnel BTB ACL reconstruction. This accelerated rehabilitation protocol was not associated with delayed bone integration. While returning to sporting activities may be possible within 5 months after the procedure, other factors, such as muscle strength, ligamentization, and the risk of re-injury, should be taken into consideration when determining the appropriate time to return to competitive-level activity, especially in athletes.
This study had limitations. First, a patient comparison group treated using an interference screw was not included in this study. Second, only a small number of patients were included in this study. Third, the use of digital tomosynthesis to evaluate bone integration is relatively poorly reported and no definite criteria have been established. Finally, this study did not analyse the clinical outcomes associated with the procedure.
Conclusions
Bone-to-bone integration on the femoral and tibial sides was complete within 5 months after anatomical rectangular tunnel BTB ACL reconstruction.
Abbreviations
- ACL:
-
Anterior cruciate ligament
- BTB:
-
Bone–patellar tendon–bone graft
- DSP:
-
Double spiked plate
- CT:
-
Computed tomography
References
Becker AS, Martini K, Higashigaito K, Guggenberger R, Andreisek G, Frauenfelder T (2017) Dose reduction in tomosynthesis of the wrist. AJR Am J Roentgenol 208:159–164
Cavanaugh JT, Powers M (2017) ACL rehabilitation progression: where are we now? Curr Rev Musculoskelet Med 10:289–296
Colombet P, Bouguennec N (2017) Suspensory fixation device for use with bone–patellar tendon–bone grafts. Arthrosc Tech 6:e833–e838
Drogset JO, Grøntvedt T, Myhr G (2006) Magnetic resonance imaging analysis of bioabsorbable interference screws used for fixation of bone–patellar tendon–bone autografts in endoscopic reconstruction of the anterior cruciate ligament. Am J Sports Med 34:1164–1169
Fink C, Benedetto KP, Hackl W, Hoser C, Freund MC, Rieger M (2000) Bioabsorbable polyglyconate interference screw fixation in anterior cruciate ligament reconstruction: a prospective computed tomography-controlled study. Arthroscopy 16:491–498
Gazaille RE, Flynn MJ, Page W, Finley S, van Holsbeeck M (2011) Technical innovation: digital tomosynthesis of the hip following intra-articular administration of contrast. Skelet Radiol 40:1467–1471
Gomi T, Hirano H (2008) Clinical potential of digital linear tomosynthesis imaging of total joint arthroplasty. J Digit Imaging 21:312–322
Goradia VK, Rochat MC, Grana WA, Rohrer MD, Prasad HS (2000) Tendon-to-bone healing of a semitendinosus tendon autograft used for ACL reconstruction in a sheep model. Am J Knee Surg 13:143–151
Grassi A, Nitri M, Moulton SG, Marcheggiani Muccioli GM, Bondi A, Romagnoli M et al (2017) Does the type of graft affect the outcome of revision anterior cruciate ligament reconstruction? A meta-analysis of 32 studies. Bone Jt J 99-B:714–723
Grassman SR, McDonald DB, Thornton GM, Shrive NG, Frank CB (2002) Early healing processes of free tendon grafts within bone tunnels is bone-specific: a morphological study in a rabbit model. Knee 9:21–26
Höher J, Möller HD, Fu FH (1998) Bone tunnel enlargement after anterior cruciate ligament reconstruction: fact or fiction? Knee Surg Sports Traumatol Arthrosc 6:231–240
Ha AS, Lee AY, Hippe DS, Chou SH, Chew FS (2015) Digital tomosynthesis to evaluate fracture healing: prospective comparison with radiography and CT. AJR Am J Roentgenol 205:136–141
Hayashi H, Kurosaka D, Saito M, Ikeda R, Kijima E, Yamashita Y et al (2017) Anterior cruciate ligament reconstruction with bone–patellar tendon–bone graft through a rectangular bone tunnel made with a rectangular retro-dilator: an operative technique. Arthrosc Tech 6:e1057–e1062
Jones KG (1963) Reconstruction of the anterior cruciate ligament. A technique using the central one-third of the patellar ligament. J Bone Jt Surg Am 45:925–932
Kawakami H, Shino K, Hamada M, Nakata K, Nakagawa S, Nakamura N et al (2004) Graft healing in a bone tunnel: bone-attached graft with screw fixation versus bone-free graft with extra-articular suture fixation. Knee Surg Sports Traumatol Arthrosc 12:384–390
Lipscomb AB, Johnston RK, Snyder RB, Warburton MJ, Gilbert PP (1982) Evaluation of hamstring strength following use of semitendinosus and gracilis tendons to reconstruct the anterior cruciate ligament. Am J Sports Med 10:340–342
Lomasney LM, Tonino PM, Coan MR (2007) Evaluation of bone incorporation of patellar tendon autografts and allografts for ACL reconstruction using CT. Orthopedics 30:152–157
Lui P, Zhang P, Chan K, Qin L (2010) Biology and augmentation of tendon–bone insertion repair. J Orthop Surg Res 5:59
Machida H, Yuhara T, Sabol JM, Tamura M, Shimada Y, Ueno E (2011) Postoperative follow-up of olecranon fracture by digital tomosynthesis radiography. Jpn J Radiol 29:583–586
Mae T, Shino K, Iuchi R, Kinugasa K, Uchida R, Nakagawa S et al (2017) Biomechanical characteristics of the anatomic rectangular tunnel anterior cruciate ligament reconstruction with a bone–patellar tendon–bone graft. J Orthop Sci 22:886–891
Martini K, Becker AS, Guggenberger R, Andreisek G, Frauenfelder T (2016) Value of tomosynthesis for lesion evaluation of small joints in osteoarthritic hands using the OARSI score. Osteoarthr Cartil 24:1167–1171
Mascarenhas R, Tranovich MJ, Kropf EJ, Fu FH, Harner CD (2012) Bone–patellar tendon–bone autograft versus hamstring autograft anterior cruciate ligament reconstruction in the young athlete: a retrospective matched analysis with 2–10 year follow-up. Knee Surg Sports Traumatol Arthrosc 20:1520–1527
Noël A, Ottenin MA, Germain C, Soler M, Villani N, Vilani N et al (2011) Comparison of irradiation for tomosynthesis and CT of the wrist. J Radiol 92:32–39
Nye DD, Mitchell WR, Liu W, Ostrander RV (2017) Biomechanical comparison of fixed-loop and adjustable-loop cortical suspensory devices for metaphyseal femoral-sided soft tissue graft fixation in anatomic anterior cruciate Ligament reconstruction using a porcine model. Arthroscopy 33:1225–1232 (e1221)
Rodeo SA, Arnoczky SP, Torzilli PA, Hidaka C, Warren RF (1993) Tendon-healing in a bone tunnel. A biomechanical and histological study in the dog. J Bone Jt Surg Am 75:1795–1803
Samuelsen BT, Webster KE, Johnson NR, Hewett TE, Krych AJ (2017) Hamstring autograft versus patellar tendon autograft for ACL reconstruction: is there a difference in graft failure rate? A meta-analysis of 47,613 patients. Clin Orthop Relat Res 475:2459–2468
Shino K, Mae T, Tachibana Y (2015) Anatomic ACL reconstruction: rectangular tunnel/bone–patellar tendon–bone or triple-bundle/semitendinosus tendon grafting. J Orthop Sci 20:457–468
Shino K, Nakata K, Nakamura N, Toritsuka Y, Horibe S, Nakagawa S et al (2008) Rectangular tunnel double-bundle anterior cruciate ligament reconstruction with bone–patellar tendon–bone graft to mimic natural fiber arrangement. Arthroscopy 24:1178–1183
Shino K, Nakata K, Nakamura N, Toritsuka Y, Nakagawa S, Horibe S (2005) Anatomically oriented anterior cruciate ligament reconstruction with a bone–patellar tendon–bone graft via rectangular socket and tunnel: a snug-fit and impingement-free grafting technique. Arthroscopy 21:1402
Suzuki T, Shino K, Nakagawa S, Nakata K, Iwahashi T, Kinugasa K et al (2011) Early integration of a bone plug in the femoral tunnel in rectangular tunnel ACL reconstruction with a bone–patellar tendon–bone graft: a prospective computed tomography analysis. Knee Surg Sports Traumatol Arthrosc 19(Suppl 1):S29–S35
Taketomi S, Inui H, Nakamura K, Yamagami R, Tahara K, Sanada T et al (2015) Secure fixation of femoral bone plug with a suspensory button in anatomical anterior cruciate ligament reconstruction with bone–patellar tendon–bone graft. Joints 3:102–108
Taketomi S, Inui H, Tahara K, Shirakawa N, Tanaka S, Nakagawa T (2017) Effects of initial graft tension on femoral tunnel widening after anatomic anterior cruciate ligament reconstruction using a bone–patellar tendon–bone graft. Arch Orthop Trauma Surg 137:1285–1291
Taketomi S, Inui H, Yamagami R, Shirakawa N, Kawaguchi K, Nakagawa T et al. (2017) Bone–patellar tendon–bone autograft versus hamstring tendon autograft for anatomical anterior cruciate ligament reconstruction with three-dimensional validation of femoral and tibial tunnel positions. J Knee Surg. https://doi.org/10.1055/s-0037-1615813
Thompson SM, Salmon LJ, Waller A, Linklater J, Roe JP, Pinczewski LA (2016) Twenty-year outcome of a longitudinal prospective evaluation of isolated endoscopic anterior cruciate ligament reconstruction with patellar tendon or hamstring autograft. Am J Sports Med 44:3083–3094
Thrush C, Porter TJ, Devitt BM (2018) No evidence for the most appropriate postoperative rehabilitation protocol following anterior cruciate ligament reconstruction with concomitant articular cartilage lesions: a systematic review. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-018-4882-x
Weiler A, Hoffmann RF, Bail HJ, Rehm O, Südkamp NP (2002) Tendon healing in a bone tunnel. Part II: histologic analysis after biodegradable interference fit fixation in a model of anterior cruciate ligament reconstruction in sheep. Arthroscopy 18:124–135
Weiler A, Peine R, Pashmineh-Azar A, Abel C, Südkamp NP, Hoffmann RF (2002) Tendon healing in a bone tunnel. Part I: biomechanical results after biodegradable interference fit fixation in a model of anterior cruciate ligament reconstruction in sheep. Arthroscopy 18:113–123
Xie X, Liu X, Chen Z, Yu Y, Peng S, Li Q (2015) A meta-analysis of bone–patellar tendon–bone autograft versus four-strand hamstring tendon autograft for anterior cruciate ligament reconstruction. Knee 22:100–110
Yoshiya S, Nagano M, Kurosaka M, Muratsu H, Mizuno K (2000) Graft healing in the bone tunnel in anterior cruciate ligament reconstruction. Clin Orthop Relat Res 376:278–286
Funding
No funding was provided to the article.
Author information
Authors and Affiliations
Contributions
HM and TN made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data, and drafting the manuscript or revising it critically for important intellectual content. ST, HI, NS, NN, and ST agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. HK gave final approval of the version to be published. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Ethical approval
The institutional review board of Teikyo University in Tokyo, Japan approved this study (ID17036).
Informed consent
All patients were informed about the procedure and provided consent for participation in the study and for the publication of their data.
Rights and permissions
About this article

Cite this article
Masuda, H., Taketomi, S., Inui, H. et al. Bone-to-bone integrations were complete within 5 months after anatomical rectangular tunnel anterior cruciate ligament reconstruction using a bone–patellar tendon–bone graft. Knee Surg Sports Traumatol Arthrosc 26, 3660–3666 (2018). https://doi.org/10.1007/s00167-018-4938-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-018-4938-y