
Abstract
Purpose
To perform a systematic review aimed to determine (1) if the postural stability deficit represents a risk factor for ankle sprains; (2) the most effective postural stability evaluation to predict ankle sprains and (3) eventual confounding factors that could influence postural stability and ankle sprain risk.
Methods
A systematic electronic search was performed in MEDLINE, EMBASE and CINAHL using the search terms (balance) OR (postural stability) matched with (lower limb) OR (ankle) OR (foot) and (sprain) OR (injury) on October 2 2017. All prospective studies that evaluated postural stability as risk factor for ankle sprains were included. The PRISMA Checklist guided the reporting and data abstraction. Methodological quality of all included papers was carefully assessed.
Results
Fifteen studies were included, evaluating 2860 individuals. Various assessment tools or instruments were used to assess postural stability. The injury incidence ranged from 10 to 34%. Postural stability deficit was recognized as risk factor for ankle sprain (OR = 1.22–10.2) in 9 cases [3 out of 3 with Star Excursion Balance Test (SEBT)]. Among the six studies that measured the center-of-gravity sway, five were able to detect worse postural stability in athletes that sustained an ankle sprain. In nine cases, the measurement of postural stability did not show any statistical relationship with ankle sprains (four out of five with examiner evaluation). In the studies that excluded patients with history of ankle sprain, postural stability was reported to be a significant risk factor in five out of six studies.
Conclusions
The ultimate role of postural stability as risk factor for ankle sprains was not defined, due to the high heterogeneity of results, patient’s populations, sports and methods of postural stability evaluation. Regarding assessment instruments, measurement of center-of-gravity sway could detect athletes at risk, however, standardized tools and protocols are needed to confirm this finding. The SEBT could be considered a promising tool that needs further investigation in wider samples. History of ankle sprains is an important confounding factor, since it was itself a source of postural stability impairment and a risk factor for ankle sprains. These information could guide clinicians in developing screening programs and design further prospective cohort studies comparing different evaluation tools.
Level of evidence
I (systematic review of prospective prognostic studies).
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Sport activity and physical exercise are considered to have long-term benefits for global heath. However, a certain risk of injury for ankle injury is present especially in young athletes performing high-impact, contact and pivoting activities but also in leisure-time activities performed by non-professional athletes. It has been estimated that almost 60% of sports injuries are sprains, luxation, and ligament tears [29], and involve extensively lower limbs, especially the ankle joint [2, 13, 21]. To try to reduce the incidence of ankle sprains, preventive programs have been introduced [6, 20, 30, 32]. However, the development of effective prevention programs is strongly related to the capacity of identifying those with a higher risk of sustaining an ankle sprain. Therefore, adequate screening tools may be a crucial component in preventing these injuries and could be used preseason to identify athletes that are at high risk of developing an ankle sprain, with the aim to adjust training programs to the individual athlete.
Systematic reviews suggested several risk factors for ankle sprains, such as generalized hyperlaxity, joints range of motion (ROM), muscle strength and balance or postural stability deficit [7, 14]. If the first could be easily quantifiable, the latter aspect represents instead a matter of debate and controversies, as no gold standard measurements are available in the literature for postural stability evaluation.
The postural stability, which has been defined as the ability to maintain and control one’s center of gravity over a base of support, is a complex mechanism derived from the coordination and synergy between vestibular, visual and somatosensory systems [26, 36]. It could be quantified by means of direct evaluation by an examiner [9, 12, 18, 31, 36] or by force plates during static tasks such as single or double stance, or with dedicate tools that tries to capture and quantify difference during the executions of a broad spectrum of dynamic tasks such as jumps, regaining balance after perturbation, or complex movement with lower limbs during single leg stance [8, 15, 34, 35].
The broad spectrum of tools, tasks and measurement methods, coupled with the heterogeneity in patients populations regarding sex, sports, and previous injuries could be responsible of the lack of general agreement in considering alterations of postural stability as a risk factor for lower limb injuries [9, 37].
The aim of the present systematic review was, therefore, to determine (1) if postural stability deficit represents a risk factor for ankle sprains; (2) the most effective postural stability evaluation to predict ankle sprains and (3) eventual confounding factors that could influence postural stability and ankle injury sprains. The answer to these questions will guide clinicians in developing screening programs for ankle sprain, identify which athletes are at risk of sprain due to postural stability deficit and recommending which tools are more useful in this task.
Materials and methods
Study design
A systematic review was performed in accordance with the preferred reporting items for systematic reviews and meta-analysis guidelines [24].
Search strategy
A systematic electronic search, assisted by a librarian, was performed in MEDLINE, EMBASE and CINAHL databases on 2 October 2017. The search terms were mapped to Medical Subject Headings (MeSH) terms where possible. Search terms were entered under three concepts: concept 1—(balance) OR (postural stability); concept 2—(lower limb) OR (ankle) OR (foot); concept 3—(sprain) OR (injury). Each concept was then combined with the ‘AND’ operator to produce the search strategy and final yield. E-pub and ahead of print papers were included as well (Supplementary Appendix 1).
Selection criteria
The following inclusion criteria, modified from Onate et al. [25] were applied to the final yield:
-
1.
Studies investigating ankle sprain prediction or risk factors;
-
2.
Study population consists primarily of physically active individuals (athletes or military) of any level of experience (eg, recreational, college, professional, etc.);
-
3.
Either populations with or without history of previous ankle injuries;
-
4.
At least one of the sprain risk factor being studied is balance or postural stability measured with tools or examiner evaluation;
-
5.
Study is peer-reviewed;
-
6.
Prospective studies;
-
7.
Study is reported in English.
Also the following exclusion criteria were applied:
-
1.
Studies not reporting original research including review articles, expert opinion, or current concepts articles;
-
2.
Posters or abstracts at annual meetings or masters theses without subsequent peer-reviewed publication of a article;
-
3.
Studies investigating risk factors other than balance and postural stability;
-
4.
Animal studies;
-
5.
Studies drawing conclusions regarding risk of ankle sprain or injury prediction based on historical data.
Article selection
To select the articles to be included in the systematic review, two non-blinded authors reviewed the title and abstract of each article identified in the literature search. When eligibility was unclear from the title and abstract, the full text of the article was obtained and evaluated for eligibility. In the case of disputes, eligibility was obtained after consulting the senior author.
Data extraction
Regarding the population studied, the following information were obtained: number of patients enrolled, number of patients evaluated, inclusion\exclusion criteria, patient sex, mean age, sports practiced and the follow-up. Regarding the balance evaluation, the following information was extracted: details of the tool or devices used, test performed and parameter measured. Also, the information of additional measurements such as joint ROM, laxity, strength or injury history was noted. Regarding ankle sprains, the following information was extracted: definition of injury, total number of sprains and incidence. Finally, the statistical relationship between balance and ankle sprains was summarized. Other possible relations with the additional parameters evaluated were extracted as well.
Quality assessment
The methodological quality was evaluated according to a modified version of the Cochrane Group on Screening and Diagnostic Test Methodology (Cochrane methods) [10], according to Dallinga et al. [7]. Two authors assessed the quality of the included studies (X.X. and X.X.). The 11 items evaluated were: “Study design” (prospective = 1 point; retrospective = 0 point); “Level of Evidence” (level 1 = 5 points; level 2 = 4 points; level 3 = 3 points; level 4 = 2 points; level 5 = 1 point); “Selection criteria” (Inclusion and exclusion criteria clearly described = 1 point); “Setting” (Enough information to identify setting = 1 point); “Demographic information” (mean or median and standard deviation or range of age, and gender reported = 1 point); “Screening tool” (Description of screening tool had sufficient detail to permit replication of the test. Test device or instruments, protocol of screening tool(s) reported = 1 point each); “Statistical analysis” (For variable of interest details given on mean or median, standard deviation or confidence intervals and predictive value = 1 point); “Reliability of screening test” (Reliability reported = 1 point); “Percentage missing” (All included subjects measured and, if appropriate, missing data or withdrawals from study reported or explained = 1 point); “Outcome” (Outcome clearly defined and method of examination of outcome adequate = 1 point); “Confounders” (Most important confounders and prognostic factors identified and adequately taken into account in design study = 1 point). The maximal score that could be reached was, therefore, 16. Since no guidelines on how to rate this score are available, we considered an excellent quality in case of 16 points, good quality with 15−14 points, fair quality with 13−10 points and poor quality with < 10 points.
Statistical analysis
Due to the heterogeneity of the population regarding age, sport and patient sex, of the injuries evaluated and of the methods of balance evaluation, it was not possible to pool the data to perform a meta-analysis. The data were, therefore, presented in a narrative manner with best of synthesis approach, summarizing the main findings of each papers focused on balance evaluation and ankle injuries.
Results
Article selection
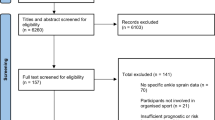
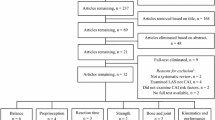
Forty-five articles were obtained in full text based on title and abstract screening. Eighteen articles were excluded, as they did not report the evaluation of balance or postural stability as a risk factor for ankle injuries. Twelve further studies were excluded because they reported the evaluation of lower limb injuries without performing a separate analysis of ankle sprains or because was retrospective. Finally, 15 studies were included in the final systematic review [1, 2, 8, 9, 12, 15, 16, 18, 19, 21, 22, 31, 33,34,35] (Fig. 1).

Flow-chart of the systematic search in the different databases
Quality assessment
The assessment of the methodological quality of the included studies is shown in Table 1. The mean score was 15.3 (range 13–16). Ten studies (67%) reported the maximum available score, therefore, representing an excellent quality, 3 studies (20%) had a good quality while only 2 (13%) presented fair quality. The items assessing the prospective study design, level of evidence I, adequate description of setting, tools, patient’s population, statistical analysis, outcomes and missing patients were rated as the maximum in all the studies. The worst scoring area was the evaluation of confounders, where 5 studies (33%) failed to meet the quality requirements. Therefore, the overall quality of the studies included in this systematic review could be considered of good to excellent.
Patient’s population
Overall, 2860 patients were screened for balance deficit as potential risk factor for ankle sprains within the 15 studies. Eleven studies (73%) evaluated patient populations > 100 athletes. Three studies (20%) analyzed athletes performing non-contact sports, 9 studies (60%) athletes involved in contact sports, and the remaining 3 studies (20%) athletes participating in both contact and non-contact sport activities. Exclusively male or female athletes were considered in 6 (40%) and 2 (13%) studies, respectively. The most relevant exclusion criteria were the presence of current injuries and the history of ankle fracture\sprain\injury (Table 2).
Postural stability evaluation
Various tool were used to assess balance: specific devices such as the New Balance Master, NeuroTest System or Neurocom Blance Master (NeuroCom International, Clackmas, OR, USA), the 3space Fastrak (Polhemus Inc, Colchester, VT, USA) and the Biodex Balance System (Biodex Medical System, Shirley, NY, USA) were used in six studies, force plates in three studies, the Star Excursion Balance Test (SEBT) in three studies, a tilt board in one study and direct evaluation by an examiner in five studies. Three studies combined two different methods.
Every study utilized different tasks, mostly dominant or non-dominant single-leg stance and bilateral stance (Table 3), except for two studies [34, 35] that applied the same protocol in male and female athletes. Therefore, many different measures were obtained to quantify the postural stability, mostly sway of center of gravity when tools were used [2, 19, 21, 33,34,35], and inability to maintain balance according to a predetermined protocol when an examiner observation was employed.
Eleven studies (73%) measured at least another parameter such as ankle ROM, general laxity, muscle strength or anatomical characteristics, other than postural stability, as risk factor for ankle sprain.
Injury evaluation
Each study provided a definition of ankle injury (Table 4). The incidence ranged from 10% in Australian Football male players [19] to 34% in division I–II volleyball male players [16], with a rate ranging from 0.3 sprains per 1000 [12] to 2.2 sprains per 1000 days of exposures [2].
According to the statistical methods used in each study, postural stability deficit was recognized as risk factor for ankle sprain in nine cases. Specifically, decreased postural stability measured with New Balance Master device had a OR = 10.2 of ankle sprain in basketball players [21], while decreased directional control and limit of stability measured with Neurocom Balance Master had higher rate of ankle sprain in freshmen athletes [34, 35]. Decreased balance on bilateral stance and increased medio-lateral and antero-posterior sway measured with force plates had an OR = 1.22–2.44 in 42 basketball [33] and Australian Football athletes, respectively [19]. Using the Star Excursion Balance Test (SEBT), a posterolateral distance < 80, ananterior distance < 63% compared to non-injured side and a posteromedial distance < 77.5% of leg length [1] were risk factors in various athletes [1, 9, 15]. Finally, failure to maintain balance as detected by an examiner was reported as risk factor for ankle sprain as well [31].
In nine cases, the measurement of postural stability did not show any statistical relationship with ankle sprain. Specifically, four studies that employed an examiner evaluation involving dance and University students [9, 18], soccer [12] and netball players, one study using the NeuroTest System [2], one study using the Biodex Balance System [16], one study employing balance on a tilt board [22], one study using the 3Space Fastrak [18] and one study using a force plate [8]. Among the six studies that measured a sway parameter [2, 19, 21, 33,34,35], five were able to detect worst postural stability in athletes that sustained an ankle sprain.
Evaluation of confounding factors
Eleven studies (73%) identified at least one risk factor for ankle sprain other than postural stability deficit (Table 4). Overall, out of the nine studies that accounted history of previous ankle sprain in the statistical models, only five identified balance deficit as risk factor for ankle sprain. In three of the remaining four studies, a positive history of previous sprain was identified a risk factor.
In the studies that excluded patients with history of ankle sprain, or without episodes in the previous 6–12 months, postural stability deficit was reported to be a significant risk factor in five out of six studies (Table 5).
Discussion
The most important finding of the present systematic review was that it is not possible to certainly identify postural stability deficit as a risk factor for ankle sprain, due to the heterogeneity of the results. In fact, in nearly half of the cases, postural stability was not correlated to ankle sprains. Moreover, the identification of the most effective tool in identifying postural stability deficit to predict ankle injuries was unsuccessful. However, most of the studies that employed instruments measuring center-of-gravity sway and those employing the SEBT were able to identify postural stability deficit as risk factor for ankle sprain. Differently, examiner evaluation failed in this task. Finally, after exclusion of patients with history of ankle injuries, a positive relation between postural stability deficit and ankle sprain was present.
Attempts to summarize the evidence of the postural stability role in lower limb injuries and, specifically, ankle sprain have been performed previously [7, 17, 25, 37]. Onate et al. [25] reported that there is a moderate evidence supporting multidirectional balance in high school-aged athletes as risk factor for future ankle sprains, however, based on the analysis of only three studies. Similarly, Witchalls et al. [37], analyzing four studies that measured postural sway with similar instrumented measures (New Balance Master, NeuroTest System, Neurocom Balance Master, force plates), identified higher postural sway and lower postural stability—together with lower eversion strength and higher plantar flexion strength—as risk factors for ankle sprains. Our systematic review was also able to highlight the center-of-gravity sway as risk factor for ankle sprain in five out of six studies. However, due to the limited number of studies included, the use of different tools and protocols, and the lack of discrimination regarding sports, sample size and sex, these finding need further confirmation in homogeneous populations using standardized tools, tests and measures of postural stability. In fact, force plates and similar technologies such as the New Balance Master, Neurocom Balance Master or Biodex Balance System, measure different parameters (e.g., sway velocity, antero-posterior center of gravity sway, directional control, degrees of platform tilt, etc.) and also involve an heterogeneous number of tasks that are grossly categorized as static or dynamic postural stability (e.g., leg stance, sway, jump, external perturbation, etc.). Therefore, their different intrinsic ability to detect a postural stability deficit could possibly mask the effective presence of an intrinsic postural stability deficit, further explaining the lack of agreement.
Regarding the evaluation by an examiner, Witchalls et al. [37] already reported its inability to adequately predict ankle sprains, confirming the findings of this review. They suggested that methods that tests postural stability by scoring the number of errors during a test, involve an increased subjectivity that might increase the variability in scores, rendering them less useful for the purpose of identifying postural stability deficit.
The Star Excursion Balance Test (SEBT) has been utilized in various tasks, including postural stability deficit detection and injury prediction. It has been demonstrated, which is able to differentiate pathological conditions such as chronic ankle instability (CAI), anterior cruciate ligament (ACL) reconstruction and Patellofemoral pain syndrome (PFPS), and to discriminate the effect of external influences such as taping, fatigue and various types of balance training [26]. Plisky et al. identified a composite score for lower limb difference less than 94% and an anterior reach difference of 4 cm or greater as a risk factor for lower limb injuries [28]. Limited to ankle sprains, a posterolateral distance < 80, an anterior distance < 63% compared to non-injured side and a posteromedial distance < 77.5% of leg length were identified as risck factors in 3 studies [1, 9, 14].
However, it should be taken into account that the tasks required to complete the SEBT could actually involve other characteristics than postural stability, such as supinated or pronated foot, joint ROM, flexibility, and muscle activation [5, 11]. Since bad motor performance [20], decreased ankle dorsiflexion [16, 34], increased calcaneal eversion [2], decreased muscle reaction time [34] and decreased dorsiflexion strength [34] have been identified as risk factors for ankle sprain, it could be possible that the results obtained with SEBT could not be related only to the mere capacity to evaluate postural stability. Thus, if the ability of SEBT to predict ankle sprains is strictly related to postural stability deficit or to other neuromuscular or anatomical features remains controversial. However, due to its high intratester (0.85–0.89) and intertester (0.97–1.00) reliability of both the original method and its simplified version (Y Balance test) [27], its simplicity and its limited cost, further studies are encouraged to confirm its ability to predict ankle injuries, possibly compared to other methodologies.
The last interesting consideration emerged from the findings of the present systematic review is the role of previous ankle injuries in the development of further injuries. As reported, only six studies evaluated athletes without history of ankle injuries in the previous 6 months. Since five out of this six studies reported postural stability as risk factor for ankle injuries, it is possible that the evaluation of postural stability deficit in patients without previous sprains is more effective and actually able to predict further injuries. Conversely, when a previous injury is present, a basal postural stability deficit could be already established due to the previous trauma, before the risk exposure. It has been in fact demonstrated a direct relationship between balance and history of ankle injuries or chronic ankle instability [4, 21, 22, 31]. Furthermore, three studies [12, 18, 22] performed a logistic regression with several independent variables in the same model, highlighting the history of previous ankle injuries but not postural stability deficit as risk factor for further ankle injuries. Therefore, this anamnestic detail should always be considered during athletes screening and in the study design of prospective studies. Finally, the results of the present systematic review could guide clinicians in developing screening programs and design further prospective cohort studies comparing different evaluation tools.
The present review has several important limitations. The most important is related to the high heterogeneity of the studies included regarding sex, sport, follow-up, methods of balance evaluation and data analysis. This did not allow the evaluation of the data through a meta-analysis; therefore, the findings obtained by the review of the available literature are based on qualitative evaluation and presented in a narrative form. Furthermore, confounding factors especially history of ankle injuries, despite acknowledged and investigated, could have masked the effect of intrinsic postural stability deficit and distort the reported evidences. Finally, the statistical methods to correlate postural stability evaluation and ankle injury were different between the studies, from multivariate analysis adjusted to confounders to simple Chi-square test, thus introducing a further source of variability.
Future studies should be aimed to evaluate postural stability through standardized instruments, protocols, tasks and measurements of center-of-gravity sway. Moreover, also the ability of SEBT to detect postural stability deficit and predict ankle sprains should be confirmed through further studies on wider and heterogeneous samples, possibly compared to instruments for center-of-gravity sway measurement.
Conclusions
The ultimate role of postural stability as risk factor for ankle sprains was not defined, due to the high heterogeneity of results, patient’s populations, sports and methods of postural stability evaluation. Regarding assessment instruments, measurement of center-of-gravity sway could detect athletes at risk, however, standardized tools and protocols are needed to confirm this finding, while the SEBT could be considered a promising tool that needs further investigation in wider samples. History of ankle sprains is an important confounding factor, since it was itself a source of postural stability impairment and a risk factor for ankle sprains.
References
Attenborough AS, Sinclair PJ, Sharp T, Greene A, Stuelcken M, Smith RM, Hiller CE (2017) The identification of risk factors for ankle sprains sustained during netball participation. Phys Ther Sport 23:31–36
Beynnon BD, Murphy DF, Alosa DM (2002) Predictive factors for lateral ankle sprains: a literature review. J Athl Train 37(4):376–380
Brown CN, Ko J, Rosen AB, Hsieh K (2015) Individuals with both perceived ankle instability and mechanical laxity demonstrate dynamic postural stability deficits. Clin Biomech (Bristol Avon) 30(10):1170–1174
Bullock-Saxton JE (1995) Sensory changes associated with severe ankle sprain. Scand J Rehabil Med 27(3):161–167
Cote KP, Brunet ME, Gansneder BM, Shultz SJ (2005) Effects of pronated and supinated foot postures on static and dynamic postural stability. J Athl Train 40(1):41–46
Crockett NJ, Sandrey MA (2015) Effect of prophylactic ankle-brace use during a high school competitive basketball season on dynamic postural control. J Sport Rehabil 24(3):252–260
Dallinga JM, Benjaminse A, Lemmink KA (2012) Which screening tools can predict injury to the lower extremities in team sports?: a systematic review. Sports Med 42(9):791–815
Dallinga JM, van der Does HT, Benjaminse A, Lemmink KA (2016) Dynamic postural stability differences between male and female players with and without ankle sprain. Phys Ther Sport 16:17:69–75
de Noronha M, França LC, Haupenthal A, Nunes GS (2013) Intrinsic predictive factors for ankle sprain in active university students: a prospective study. Scand J Med Sci Sports 23(5):541–547
Deville ́ WL, Buntinx F, Bouter LM et al (2002) Conducting systematic reviews of diagnostic studies: didactic guidelines. BMC Med Res Methodol 3:2–9
Earl JE, Hertel J (2001) Lower-extremity muscle activation during the Star Excursion Balance Tests. J Sport Rehabil 10(2):93–104
Engebretsen AH, Myklebust G, Holme I, Engebretsen L, Bahr R (2010) Intrinsic risk factors for acute ankle injuries among male soccer players: a prospective cohort study. Scand J Med Sci Sports 20(3):403–410
Fong DT, Hong Y, Chan LK, Yung PS, Chan KM (2007) A systematic review on ankle injury and ankle sprain in sports. Sports Med 37(1):73–94
Gribble PA, Hertel J, Plisky P (2012) Using the Star Excursion Balance Test to assess dynamic postural-control deficits and outcomes in lower extremity injury: a literature and systematic review. J Athl Train 47(3):339–357
Gribble PA, Terada M, Beard MQ, Kosik KB, Lepley AS, McCann RS, Pietrosimone BG, Thomas AC (2016) Prediction of lateral ankle sprains in football players based on clinical tests and body mass index. Am J Sports Med 44(2):460–467
Hadzic V, Sattler T, Topole E, Jarnovic Z, Burger H, Dervisevic E (2009) Risk factors for ankle sprain in volleyball players: a preliminary analysis. Isokinet Exerc Sci 2009 17(3):155–160
Hegedus EJ, McDonough SM, Bleakley C, Baxter D, Cook CE (2015) Clinician-friendly lower extremity physical performance tests in athletes: a systematic review of measurementproperties and correlation with injury. Part 2—the tests for the hip, thigh, foot and ankle including the starexcursion balance test. Br J Sports Med 49(10):649–656
Hiller CE, Refshauge KM, Herbert RD, Kilbreath SL (2008) Intrinsic predictors of lateral ankle sprain in adolescent dancers: a prospective cohort study. Clin J Sport Med 18(1):44–48
Hrysomallis C, McLaughlin P, Goodman C (2007) Balance and injury in elite Australian footballers. Int J Sports Med 28(10):844–847
Janssen KW, van der Zwaard BC, Finch CF, van Mechelen W, Verhagen EA (2016) Interventions preventing ankle sprains; previous injury and high-risk sport participation as predictors of compliance. J Sci Med Sport 19(6):465–469
McGuine TA, Greene JJ, Best T, Leverson G (2000) Balance as a predictor of ankle injuries in high school basketball players. Clin J Sport Med 10(4):239–244
McHugh MP, Tyler TF, Tetro DT, Mullaney MJ, Nicholas SJ (2006) Risk factors for noncontact ankle sprains in high school athletes: the role of hip strength and balance ability. Am J Sports Med 34(3):464–470
Meardon S, Klusendorf A, Kernozek T (2016) Influence of injury on dynamic postural control in runners. Int J Sports Phys Ther 11(3):366–377
Moher D, Liberati A, Tetzlaff J et al (2009) PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6:e1000097
Onate JA, Everhart JS, Clifton DR, Best TM, Borchers JR, Chaudhari AM (2016) Physical exam risk factors for lower extremity injury in high school athletes: a systematic review. Clin J Sport Med 26(6):435–444
Paterno MV, Schmitt LC, Ford KR et al (2010) Biomechanical measures during landing and postural stability predict second anterior cruciate ligament injury after anterior cruciate ligament reconstruction and return to sport. Am J Sports Med 38(10):1968–1978
Plisky PJ, Gorman PP, Butler RJ, Kiesel KB Underwood FB, Elkins B (2009) The reliability of an instrumented device for measuring components of the star excursion balance test. N Am J Sports Phys Ther 4(2):92–99
Plisky PJ, Rauh MJ, Kaminski TW, Underwood FB (2006) Star Excursion Balance Test as a predictor of lower extremity injury in high school basketball players. J Orthop Sports Phys Ther 36(12):911–919
Schneider S, Seither B, Tönges S, Schmitt H (2006) Sports injuries: population based representative data on incidence, diagnosis, sequelae, and high risk groups. Br J Sports Med 40:334–339
Taylor JB, Ford KR, Nguyen AD, Terry LN, Hegedus EJ (2015) Prevention of lower extremity injuries in basketball: a systematic review and meta-analysis. Sports Health 7(5):392–398
Trojian TH, McKeag DB (2006) Single leg balance test to identify risk of ankle sprains. Br J Sports Med 40(7):610–613
Verhagen EA1, Bay K (2010) Optimising ankle sprain prevention: a critical review and practical appraisal of the literature. Br J Sports Med 44(15):1082–1088
Wang HK, Chen CH, Shiang TY, Jan MH, Lin KH (2006) Risk-factor analysis of high school basketball-player ankle injuries: a prospective controlled cohort studyevaluating postural sway, ankle strength, and flexibility. Arch Phys Med Rehabil 87(6):821–825
Willems TM, Witvrouw E, Delbaere K, Mahieu N, De Bourdeaudhuij I, De Clercq D (2005) Intrinsic risk factors for inversion ankle sprains in male subjects: a prospective study. Am J Sports Med 33(3):415–423
Willems TM, Witvrouw E, Delbaere K, Philippaerts R, De Bourdeaudhuij I, De Clercq D (2005) Intrinsic risk factors for inversion ankle sprains in females—a prospective study. Scand J Med Sci Sports 15(5):336–345
Winter DA (1995) Human balance and posture control during standing and walking. Gait Posture 3:193–214
Witchalls J, Blanch P, Waddington G, Adams R (2012) Intrinsic functional deficits associated with increased risk of ankle injuries: a systematic review with meta-analysis. Br J Sports Med 46(7):515–523
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All the authors declare no conflict of interests related to the ideation, preparation and production of the present manuscript.
Funding
No funding was present.
Ethical standards
Due to the review nature of thie paper, no human patients nor animal were involved in any phase of the study preparation.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Grassi, A., Alexiou, K., Amendola, A. et al. Postural stability deficit could predict ankle sprains: a systematic review. Knee Surg Sports Traumatol Arthrosc 26, 3140–3155 (2018). https://doi.org/10.1007/s00167-017-4818-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-017-4818-x